'A summary of the evidence against the COVID vaccines; Here's a quick summary of the key pieces of evidence that taken together show that the COVID vaccines are unsafe and that the medical community
should not be trusted.' Good substack by Steve Kirsch & I will present his substack but prior, I remind Steve & you of my seminal review listing out all key studies early on showing the vaccine FAILED

Steve failed to include my review so I will do it here, and I commend his strong scholarship here, a tremendous lot of good information is contained within:
https://brownstone.org/articles/16-studies-on-vaccine-efficacy/
Example of studies below:
1) Gazit et alshowed that “SARS-CoV-2-naïve vaccinees had a 13-fold (95% CI, 8-21) increased risk for breakthrough infection with the Delta variant compared to those previously infected.” When adjusting for the time of disease/vaccine, there was a 27-fold increased risk (95% CI, 13-57).
2) Acharya et al.Ignoring the risk of infection, given that someone was infected, Acharya et al. found “no significant difference in cycle threshold values between vaccinated and unvaccinated, asymptomatic and symptomatic groups infected with SARS-CoV-2 Delta.”
3) Riemersma et al.found “no difference in viral loads when comparing unvaccinated individuals to those who have vaccine “breakthrough” infections. Furthermore, individuals with vaccine breakthrough infections frequently test positive with viral loads consistent with the ability to shed infectious viruses.” Results indicate that “if vaccinated individuals become infected with the delta variant, they may be sources of SARS-CoV-2 transmission to others.” They reported “low Ct values (<25) in 212 of 310 fully vaccinated (68%) and 246 of 389 (63%) unvaccinated individuals. Testing a subset of these low-Ct samples revealed infectious SARS-CoV-2 in 15 of 17 specimens (88%) from unvaccinated individuals and 37 of 39 (95%) from vaccinated people.”
4) Chemaitelly et al.In a study from Qatar, Chemaitelly et al. reported vaccine efficacy (Pfizer) against severe and fatal disease, with efficacy in the 85-95% range at least until 24 weeks after the second dose. As a contrast, the efficacy against infection waned down to around 30% at 15-19 weeks after the second dose.
5) Riemersma et al.From Wisconsin, Riemersma et al. reported that vaccinated individuals who get infected with the Delta variant can transmit SARS-CoV-2 to others. They found an elevated viral load in the unvaccinated and vaccinated symptomatic persons (68% and 69% respectively, 158/232 and 156/225). Moreover, in the asymptomatic persons, they uncovered elevated viral loads (29% and 82% respectively) in the unvaccinated and the vaccinated respectively. This suggests that the vaccinated can be infected, harbor, cultivate, and transmit the virus readily and unknowingly.
6) SubramanianSubramanian reported that “at the country-level, there appears to be no discernable relationship between percentage of population fully vaccinated and new COVID-19 cases.” When comparing 2947 counties in the United States, there were slightly less cases in more vaccinated locations. In other words, there is no clear discernable relationship .
7) Chau et al.looked at transmission of SARS-CoV-2 Delta variant among vaccinated healthcare workers in Vietnams. Of 69 healthcare workers that tested positive for SARS-CoV-2, 62 participated in the clinical study, all of whom recovered. For 23 of them, complete-genome sequences were obtained, and all belonged to the Delta variant. “Viral loads of breakthrough Delta variant infection cases were 251 times higher than those of cases infected with old strains detected between March-April 2020”.
8) Brown et al.In Barnstable, Massachusetts, Brown et al. found that among 469 cases of COVID-19, 74% were fully vaccinated, and that “the vaccinated had on average more virus in their nose than the unvaccinated who were infected.”
9) Hetemäli et al.Reporting on a nosocomial hospital outbreak in Finland, Hetemäli et al. observed that “both symptomatic and asymptomatic infections were found among vaccinated health care workers, and secondary transmission occurred from those with symptomatic infections despite use of personal protective equipment.”
10) Shitrit et al.In a hospital outbreak investigation in Israel, Shitrit et al. observed “high transmissibility of the SARS-CoV-2 Delta variant among twice vaccinated and masked individuals.” They added that “this suggests some waning of immunity, albeit still providing protection for individuals without comorbidities.”
11) UK COVID-19 vaccine Surveillance Report for week #42In the UK COVID-19 vaccine Surveillance Report for week #42, it was noted that there is “waning of the N antibody response over time” and “that N antibody levels appear to be lower in individuals who acquire infection following 2 doses of vaccination.” The same report (Table 2, page 13), shows the in the older age groups above 30, the double vaccinated persons have greater infection risk than the unvaccinated, presumably because the latter group include more people with stronger natural immunity from prior Covid disease. As a contrast, the vaccinated people had a lower risk of death than the unvaccinated, across all age groups, indicating that vaccines provide more protection against death than against infection. See also UK PHE reports 43, 44, 45, 46 for similar data.
12) Levin et al.In Israel, Levin et al. “conducted a 6-month longitudinal prospective study involving vaccinated health care workers who were tested monthly for the presence of anti-spike IgG and neutralizing antibodies”. They found that “six months after receipt of the second dose of the BNT162b2 vaccine, humoral response was substantially decreased, especially among men, among persons 65 years of age or older, and among persons with immunosuppression.”
13) Rosenberg et al.In a study from New York State, Rosenberg et al. reported that “During May 3–July 25, 2021, the overall age-adjusted vaccine effectiveness against hospitalization in New York was relatively stable 89.5%–95.1%). The overall age-adjusted vaccine effectiveness against infection for all New York adults declined from 91.8% to 75.0%.”
14) Suthar et al.Suthar et al. noted that “Our data demonstrate a substantial waning of antibody responses and T cell immunity to SARS-CoV-2 and its variants, at 6 months following the second immunization with the BNT162b2 vaccine.”
15) Nordström et al.In a study from Umeå University in Sweden, Nordström et al. observed that “vaccine effectiveness of BNT162b2 against infection waned progressively from 92% (95% CI, 92-93, P<0·001) at day 15-30 to 47% (95% CI, 39-55, P<0·001) at day 121-180, and from day 211 and onwards no effectiveness could be detected (23%; 95% CI, -2-41, P=0·07).”
16) Yahi et al.Yahi et al. have reported that “in the case of the Delta variant, neutralizing antibodies have a decreased affinity for the spike protein, whereas facilitating antibodies display a strikingly increased affinity. Thus, antibody dependent enhancement may be a concern for people receiving vaccines based on the original Wuhan strain spike sequence.”
17) Goldberg et al. (BNT162b2 Vaccine in Israel) reported that “immunity against the delta variant of SARS-CoV-2 waned in all age groups a few months after receipt of the second dose of vaccine.”
18) Singanayagam et al.examined the transmission and viral load kinetics in vaccinated and unvaccinated individuals with mild delta variant infection in the community. They found that (in 602 community contacts (identified via the UK contract-tracing system) of 471 UK COVID-19 index cases were recruited to the Assessment of Transmission and Contagiousness of COVID-19 in Contacts cohort study and contributed 8145 upper respiratory tract samples from daily sampling for up to 20 days) “vaccination reduces the risk of delta variant infection and accelerates viral clearance. Nonetheless, fully vaccinated individuals with breakthrough infections have peak viral load similar to unvaccinated cases and can efficiently transmit infection in household settings, including to fully vaccinated contacts.”
19) Keehner et al.in NEJM, has recently reported on the resurgence of SARS-CoV-2 infection in a highly vaccinated health system workforce. Vaccination with mRNA vaccines began in mid-December 2020; by March, 76% of the workforce had been fully vaccinated, and by July, the percentage had risen to 87%. Infections had decreased dramatically by early February 2021…”coincident with the end of California’s mask mandate on June 15 and the rapid dominance of the B.1.617.2 (delta) variant that first emerged in mid-April and accounted for over 95% of UCSDH isolates by the end of July, infections increased rapidly, including cases among fully vaccinated persons…researchers reported that the “dramatic change in vaccine effectiveness from June to July is likely to be due to both the emergence of the delta variant and waning immunity over time.”
20) Juthani et al.Juthani et al. sought to describe the impact of vaccination on admission to hospital in patients with confirmed SARS-CoV-2 infection using real-world data collected by the Yale New Haven Health System. “Patients were considered fully vaccinated if the final dose (either second dose of BNT162b2 or mRNA-1273, or first dose of Ad.26.COV2.S) was administered at least 14 days before symptom onset or a positive PCR test for SARS-CoV-2. In total, we identified 969 patients who were admitted to a Yale New Haven Health System hospital with a confirmed positive PCR test for SARS-CoV-2”…Researchers reported “a higher number of patients with severe or critical illness in those who received the BNT162b2 vaccine than in those who received mRNA-1273 or Ad.26.COV2.S…”
21) the CDCA very recent study published by the CDC reported that a majority (53%) of patients who were hospitalized with Covid-19-like illnesses were already fully vaccinated with two-dose RNA shots. Table 1 reveals that among the 20,101 immunocompromised adults hospitalized with Covid-19, 10,564 (53%) were fully-vaccinated with the Pfizer or Moderna vaccine (Vaccination was defined as having received exactly 2 doses of an mRNA-based COVID-19 vaccine ≥14 days before the hospitalization index date, which was the date of respiratory specimen collection associated with the most recent positive or negative SARS-CoV-2 test result before the hospitalization or the hospitalization date if testing only occurred after the admission). This highlights the ongoing challenges faced with Delta breakthrough when vaccinated.
22) Eyre, 2021 The impact of SARS-CoV-2 vaccination on Alpha & Delta variant transmission.Eyre, 2021 looked at The impact of SARS-CoV-2 vaccination on Alpha & Delta variant transmission. They reported that “while vaccination still lowers the risk of infection, similar viral loads in vaccinated and unvaccinated individuals infected with Delta question how much vaccination prevents onward transmission… transmission reductions declined over time since second vaccination, for Delta reaching similar levels to unvaccinated individuals by 12 weeks for ChAdOx1 and attenuating substantially for BNT162b2. Protection from vaccination in contacts also declined in the 3 months after second vaccination…vaccination reduces transmission of Delta, but by less than the Alpha variant.”
23) Levine-TiefenbrunLevine-Tiefenbrun, 2021 looked at Viral loads of Delta-variant SARS-CoV-2 breakthrough infections after vaccination and booster with BNT162b2, and reported the viral load reduction effectiveness declines with time after vaccination, “significantly decreasing at 3 months after vaccination and effectively vanishing after about 6 months.”
24) Puranik, 2021 Comparison of two highly-effective mRNA vaccines for COVID-19 during periods of Alpha and Delta variant prevalencePuranik, 2021 looked at a Comparison of two highly-effective mRNA vaccines for COVID-19 during periods of Alpha and Delta variant prevalence, reporting “In July, vaccine effectiveness against hospitalization has remained high (mRNA-1273: 81%, 95% CI: 33–96.3%; BNT162b2: 75%, 95% CI: 24–93.9%), but effectiveness against infection was lower for both vaccines (mRNA-1273: 76%, 95% CI: 58–87%; BNT162b2: 42%, 95% CI: 13–62%), with a more pronounced reduction for BNT162b2.”
25) Saade, 2021 Live virus neutralization testing in convalescent patients and subjects vaccinated against 19A, 20B, 20I/501Y.V1 and 20H/501Y.V2 isolates of SARS-CoV-2Saade, 2021 looked at Live virus neutralization testing in convalescent patients and subjects vaccinated against 19A, 20B, 20I/501Y.V1 and 20H/501Y.V2 isolates of SARS-CoV-2, and reported as “Assessed the neutralizing capacity of antibodies to prevent cell infection, using a live virus neutralization test with different strains [19A (initial one), 20B (B.1.1.241 lineage), 20I/501Y.V1 (B.1.1.7 lineage), and 20H/501Y.V2 (B.1.351 lineage)] in serum samples collected from different populations: two-dose vaccinated COVID-19-naive healthcare workers (HCWs; Pfizer-BioNTech BNT161b2), 6-months post mild COVID-19 HCWs, and critical COVID-19 patients… finding of the present study is the reduced neutralizing response observed towards the 20H/501Y.V2 variant in fully immunized subjects with the BNT162b2 vaccine by comparison to the wild type and 20I/501Y.V1 variant.”
26) Canaday, 2021 Significant reduction in humoral immunity among healthcare workers and nursing home residents 6 months after COVID-19 BNT162b2 mRNA vaccinationCanaday, 2021 looked at Significant reduction in humoral immunity among healthcare workers and nursing home residents 6 months after COVID-19 BNT162b2 mRNA vaccination, reporting “Anti-spike, anti-RBD and neutralization levels dropped more than 84% over 6 months’ time in all groups irrespective of prior SARS-CoV-2 infection. At 6 months post-vaccine, 70% of the infection-naive NH residents had neutralization titers at or below the lower limit of detection compared to 16% at 2 weeks after full vaccination. These data demonstrate a significant reduction in levels of antibody in all groups. In particular, those infection-naive NH residents had lower initial post-vaccination humoral immunity immediately and exhibited the greatest declines 6 months later.”
27) Israel, 2021 Large-scale study of antibody titer decay following BNT162b2 mRNA vaccine or SARS-CoV-2 infectionIsrael, 2021 looked at Large-scale study of antibody titer decay following BNT162b2 mRNA vaccine or SARS-CoV-2 infection, and reported as “To determine the kinetics of SARS-CoV-2 IgG antibodies following administration of two doses of BNT162b2 vaccine, or SARS-CoV-2 infection in unvaccinated individuals…In vaccinated subjects, antibody titers decreased by up to 40% each subsequent month while in convalescents they decreased by less than 5% per month. Six months after BNT162b2 vaccination 16.1% subjects had antibody levels below the sero-positivity threshold of <50 AU/mL, while only 10.8% of convalescent patients were below <50 AU/mL threshold after 9 months from SARS-CoV-2 infection.”
28) Eyran, 2020 The longitudinal kinetics of antibodies in COVID-19 recovered patients over 14 monthsEyran, 2020 examined The longitudinal kinetics of antibodies in COVID-19 recovered patients over 14 months, and found “a significantly faster decay in naïve vaccinees compared to recovered patients suggesting that the serological memory following natural infection is more robust compared to vaccination. Our data highlights the differences between serological memory induced by natural infection vs. vaccination.”
29) Salvatore et al.Salvatore et al. examined the transmission potential of vaccinated and unvaccinated persons infected with the SARS-CoV-2 Delta variant in a federal prison, July-August 2021. They found a total of 978 specimens were provided by 95 participants, “of whom 78 (82%) were fully vaccinated and 17 (18%) were not fully vaccinated….clinicians and public health practitioners should consider vaccinated persons who become infected with SARS-CoV-2 to be no less infectious than unvaccinated persons.”
30) Andeweg et al.Andeweg et al. analyzed 28,578 sequenced SARS-CoV-2 samples from individuals with known immune status obtained through national community testing in the Netherlands from March to August 2021. They found evidence for an “increased risk of infection by the Beta (B.1.351), Gamma (P.1), or Delta (B.1.617.2) variants compared to the Alpha (B.1.1.7) variant after vaccination. No clear differences were found between vaccines. However, the effect was larger in the first 14-59 days after complete vaccination compared to 60 days and longer. In contrast to vaccine-induced immunity, no increased risk for reinfection with Beta, Gamma or Delta variants relative to Alpha variant was found in individuals with infection-induced immunity.”
.
.
.

Start Kirsch here:
‘Here is a short list of reasons that everyone should be concerned about the COVID vaccine. This is not an exhaustive list.
Doctors are told to trust the FDA and CDC, but not verify, when prescribing vaccines. All the post-marketing safety data is kept hidden by health authorities so not even doctors can look at the data themselves to find out if any vaccine is safe. Doctors have to trust the authorities. They are essentially told: “trust, do not verify.”

The CDC itself doesn’t have the data to make a post-marketing independent vaccine safety assessment and they are not interested in obtaining the data either! The CDC relies on the FDA who relies on the manufacturer to test the product. The CDC could ask states for vaccination records tied to death records, but they don’t want to even ask because if they did an analysis, it could be discovered in a FOIA request. The CDC basically has no interest whatsoever in verifying what the actual safety data is.
Lack of transparency by health authorities. Not a single health authority anywhere in the world has ever released anonymized record-level patient data for independent researchers to assess the safety of any vaccine. There isn’t any paper in a peer-reviewed journal showing that health outcomes are improved if public health data is kept secret.
Lack of interest in data transparency by the medical community. Can you name a single high-profile pro-vaccine member of the medical community who has called for data transparency of public health data? Time-series cohort analyses can be easily produced by health authorities and published for everyone to see. These would show safety signals and do not jeopardize patient privacy. These are all kept hidden.
We aren’t allowed to see even the simplest of charts. Wouldn’t it be great to define two cohorts on July 1, 2021: COVID vaccinated vs. COVID unvaccinated. Then you simply record the deaths from that point forward and plot them. Why isn’t this being published?
Misinformation is deemed to be a problem, but the people making these statements are unwilling to take any steps to stop the so-called misinformation. These steps include: open public discussion to resolve differences of opinion and making public health data available/public in a way that preserves privacy. For example, HHS (as well as every state health department) should welcome all of us with open arms and invite us to query their databases (such as VSD and Medicare in the case of HHS) and publish whatever we find. Why does this information need to be hidden? The numbers tell the story, not the individual records.
No response from health authorities to reasonable requests. I’ve sent emails to Sarah Caul of the UK ONS on four ways the ONS can increase data transparency. There was no response.
No response when asked to explain damaging evidence. When credible scientists receive government data that shows very troubling safety signals, there is a total unwillingness of any health authority to discuss the matter and resolve it.
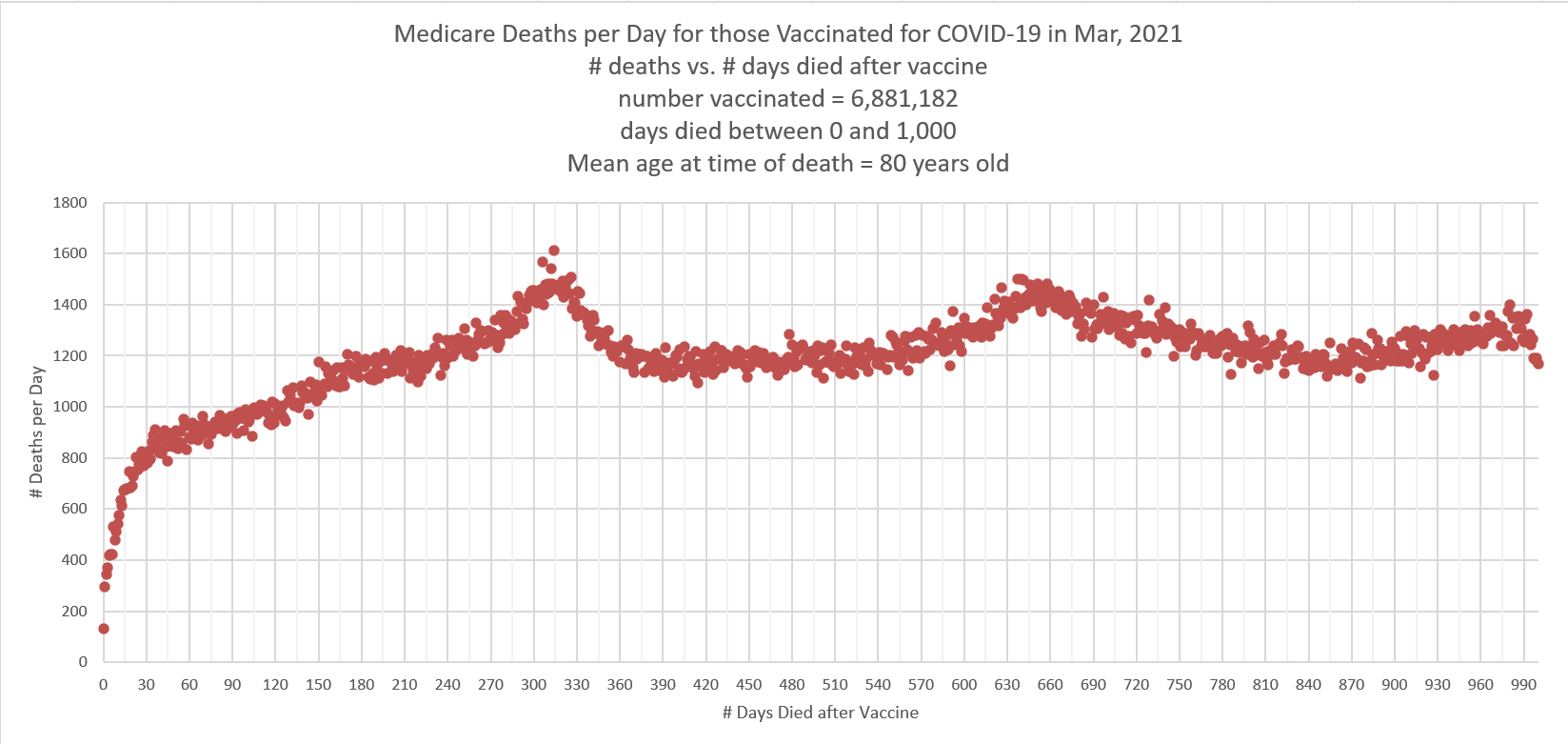
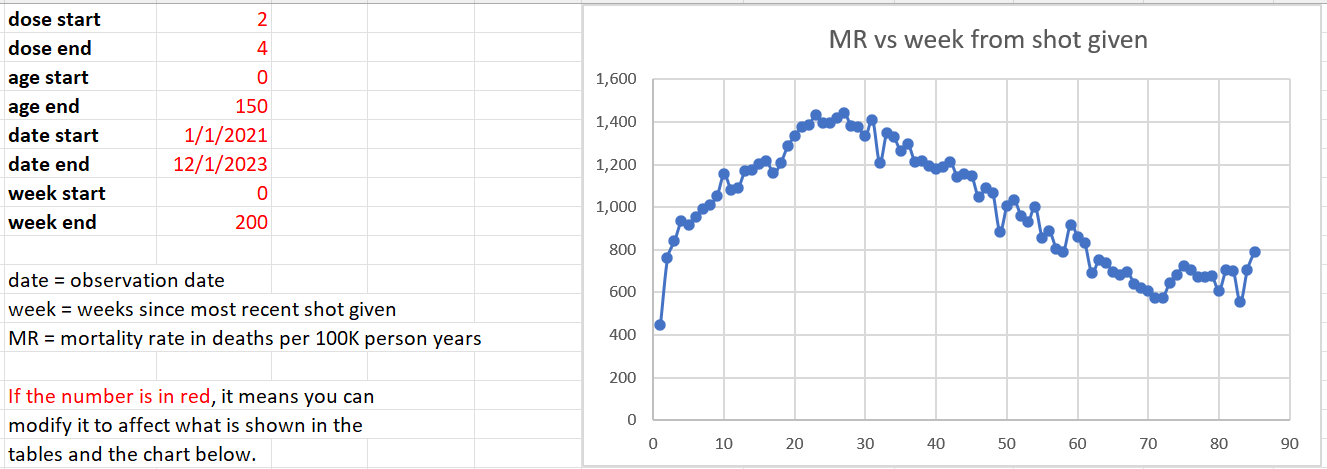
The US Medicare data clearly shows mortality increases after people take the jab. Is there any epidemiologist who can explain why deaths rose during a period in time when they should have been falling (per the Medicare death data)?
The patient-level data released from NZ data confirms that mortality increases after the shots are given despite the fact that most of the shots were given during time periods when deaths were falling
Anecdotes such as the one from Jay Bonnar who lost 15 of his DIRECT friends unexpectedly since the shots rolled out. Four of the 15 died on the same day as that vaccine was given. Before the shots rolled out, Jay had lost only one friend unexpectedly. The probability this happened by chance is given by poisson.sf(14, .25) which is 5.6e-22. So this can’t happen by chance. SOMETHING killed Jay’s friends and 4 of the 15 died on the same day as they were vaccinated. Is there a more plausible explanation for what killed Jay’s friends? All of them who died were vaccinated with the COVID vaccines.
Well done studies like the one done by Denis Rancourt showing 1 death per 800 shots on average. Jay Bonnar estimates he has around 14,000 friends so Jay’s numbers are consistent with Rancourt’s results.
Survey data like Skidmore and Rasmussen Reports showing that hundreds of thousands of Americans have been killed by the COVID shots. There have never been any counter surveys published showing this not to be the case.
The lack of any success stories. It appears that “vaccine success stories” where COVID infection fatality ratios dropped or that myocarditis cases plummeted do not exist. The US Nursing home data shows that the infection fatality rate (IFR) increased after the vaccine rolled out. There is nobody using that data making the claim it reduced the IFR.
Anecdotes from healthcare are extremely troubling. One nurse reported a hospital admission rate that was 3X higher than anything in the 33-year history of the hospital after the COVID vaccines rolled out. Symptoms rarely ever seen were common after vaccines rolled out in that age group.
Lack of autopsies in clinical trials and post-marketing. The CDC doesn’t request anyone to do autopsies even for people who die on the same day as they got the vaccine. Don’t they want to know what killed those people… just to be sure?
Young people dying in sleep. There are way too many cases of young people who die in their sleep after being vaccinated. Doctors say this is a rare event. Now it is much more common. If the shots are safe, why is this happening?
I have direct personal experience with the vaccine: two people I know were killed by the vaccine, none from COVID. I know many people who are vaccine injured from the COVID vaccine.
Corruption in the VAERS system used to track adverse events. See this presentation by Albert Albert Benavides. In addition, the v-safe system showed that 8% of the people who got the vaccine had to see medical attention (which is in itself a train wreck), but the CDC refused to voluntarily disclose this important information and even today they don’t talk about it.
The CDC covered up 770 safety signals. They didn’t tell the public about them at all. Not even hinting at them. A safety signal is very serious. To get one safety signal would be concerning. But to get 770 safety signals triggered (on 770 different adverse event types) and then not say anything to the public about it is a sure sign of a very corrupt public agency whose job is to protect the manufacturers, not the public.
Ed Dowd’s book statistics. This very popular book (“Cause Unknown”) listed 500 who died unexpectedly. Ed didn’t know how many were unvaccinated. Only one person has come forward saying that one of the people in the book who died after the vaccines rolled out was unvaccinated.
Prominent doctor/scientists switching sides. Paul Marik is one of the top intensivists in the world. After seeing many COVID vaccine injured patients, he changed his mind about the safety of vaccines. When he was not allowed to practice medicine consistent with his Hippocratic Oath, he resigned his position.
The corruption with COVID protocols. The COVID hospital protocols likely caused 90% of the COVID deaths in hospitals. This led to Paul Marik resigning. See details in this article. Why are doctors forced to use hospital protocols that kill a huge percentage of patients instead of using their best judgment to save patients?
This JAMA paper shows that COVID and influenza vaccines don’t work. Why are we pushing a vaccine where the statistics clearly show the vaccines don’t work?
The consistency of the data. There have been no counter-anecdotes showing the vaccines are safe. I keep looking for one and come up empty.
No debates with anyone prominent promoting the government narrative. Those who promote the narrative refuse to engage in any scientific discussions to resolve differences of opinion. This is similar to the question of whether vaccines cause autism: nobody who thinks it doesn’t is willing to engage in a public discussion about it to discuss the evidence. Why not resolve the issue through dialog? It isn’t resolved in the peer-review literature where half the papers say vaccines cause autism and the other half don’t. Why can’t we talk about it?
Fear and intimidation tactics are used to silence dissent. Open debate would be more productive. But people are not allowed to hold or discuss views that go against the “consensus” or they will lose their jobs, their certifications, or their medical licenses. Health care workers are told they will be fired if they report an adverse event to VAERS, there are nurses who won’t talk about anaphylaxis after getting the vaccine for fear of being fired, vaccine injuries are covered up, hospital workers are afraid to talk about it at work.
The cognitive dissonance is very disturbing. When healthcare workers bring up the topic of mortality and morbidity due to the vaccine, their peers say nothing and walk away.
Censorship tactics employed by the US government to silence dissent instead of public recorded open debates. History has shown that purveyors of censorship are always on the wrong side of the issue.’
Go and take your ivermechtin everyone a pet parasite medication. Only 45.99 for 6 tablets. Thats their method of detox to the people of the world. Turn and rely on their big pharma and fill their fucking pockets. So many natural detox methods many need to be made aware of. They will never tell you cause then they do not fill their own pockets and keep all of us sick and relying on the next pharma
Love it Dr. Paul! This evidence is like receiving new munitions in a war to protect those we love.