Tolerance? Irrang et al.: "Class switch towards non-inflammatory, spike-specific IgG4 antibodies after repeated SARS-CoV-2 mRNA vaccination"; researchers show multiple boosters subvert immune response
Alarming & Importantly: this class switch was associated with reduced capacity of the spike-specific antibodies to mediate antibody-dependent cellular phagocytosis & complement deposition. TOLERANCE??

The issue of immune tolerance we have raised prior (Vanden Bossche, myself, McCullough and other scientists and doctors) and is very important and troubling if this study is clarifying it and definitively pointing to it due to the COVID gene therapy injection (especially the boosting). Are we now facing down a quartet of deranged dysfunctional sequelae post COVID gene injection namely i) viral immune escape, ii) original antigenic sin (immune imprinting, fixation, prejudicing), iii) antibody-dependent enhancement of infection (ADEI) and of disease (ADED) and now iv) immune tolerance?
Holy moly, Robin! to the bat-cave, this is very dangerous! This is where we need expertise of someone like Dr. Geert Vanden Bossche or Dr. Peter McCullough or Dr. Ramin Oskoui, not the so called ‘expert’ morons and buffoons like Njoo and Tam and Walensky et al. who have gotten us into this mess with a fraud ineffective, harmful, non-safety tested, non-sterilizing, non-neutralizing gene injection. That these idiots continue to roll-out while there is massive infectious pressure.
Geert, where are you when we need you, we need some logic here!
The thing is that Bourla of Pfizer and Bancel of Moderna and Fauci and Francis Collins, these four Horsemen of the Apocalypse have really screwed us good with this fraud gene therapy injection.
But first:
It’s the vaccine, you stupid, it’s the vaccine, NOT the virus!
I remind you again. It is a sub-optimal non-sterilizing, non-neutralizing vaccine that is implemented in the midst of ongoing infection (massive infectious pressure) that is driving not just more infectious variants, but for the selection of more virulent variants. Natural selection pressure (due to a sub-optimal vaccine with induced antigen-specific vaccinal antibodies that do not get to their maximal ‘full’ binding affinity) on the infectiousness of the virus will continue to drive infectious variant, one after the other. Be warned! You never ever vaccinate while there is virus circulating, while a pandemic is raging as we did starting February or so 2021. Insanity! The vaccine makers Moderna et al. and CDC and NIH and FDA and Fauci and Francis Collins et al. know exactly what they are doing. This pandemic will never ever end. They set it up so, and with this fraud ineffective deadly ‘gene injection’ vaccine. It has never worked! That’s the big secret!
SOURCE:
https://www.science.org/doi/10.1126/sciimmunol.ade2798?utm_source=substack&utm_medium=email
First, let us calm down as we read this paper on 29 health care workers and try to understand the implications. No doubt, IgG4 is poorly studied and understood and our experience is that it plays the least role among other IgG antibodies in the immune response (IgG immunoglobulins).
So not sure yet if this is entirely alarming, in my capacity. Is this a good thing or a bad thing, in terms of class switching to IgG4 antibodies? We need experts to weigh in on this for IMO the researchers did not properly interpret their own research findings. So not sure if we are to worry about this but the issue of tolerance is important if this is unfolding and this is shown definitively and stably. In fact, it is devastating. In short, the immune system is being told to stand down based on the surge of IgG 4 antibodies. Do not attack. We are thus open to all things with these gene injections that have proven to be deadly and we are seeing it constantly in the published data.
Yet is the class switch thus irrelevant in terms of the impact on subsequent infection, vaccinal antibody protection? Is there any in the first place? Is this indicative of some type of tolerance? My understanding of the immune response is that IgG4 plays a key role in ‘tolerance’ as it is pivoted to (shifted to) when you are repeatedly exposed to environmental entities that are benign e.g. pollen. If the entity must be tolerated due to it being a regular or routine part of your environment like some pollen, then you have to tolerate it else you will get very symptomatic and ill each time with subsequent exposures. Thus the million dollar questions is: is the vaccinated person’s immune system learning to ‘tolerate’ spike protein and especially with repeated boosting? Is the surge in IgG4 indicative of this?
Thus does greater levels of IgG4 post 3rd booster (and more) place you onto a path of more severe disease? Is this due to the spike protein or the mRNA itself? Does this happen with other pathogen? We need this answered too.
But all the well, let us look at the findings.
Key statement:
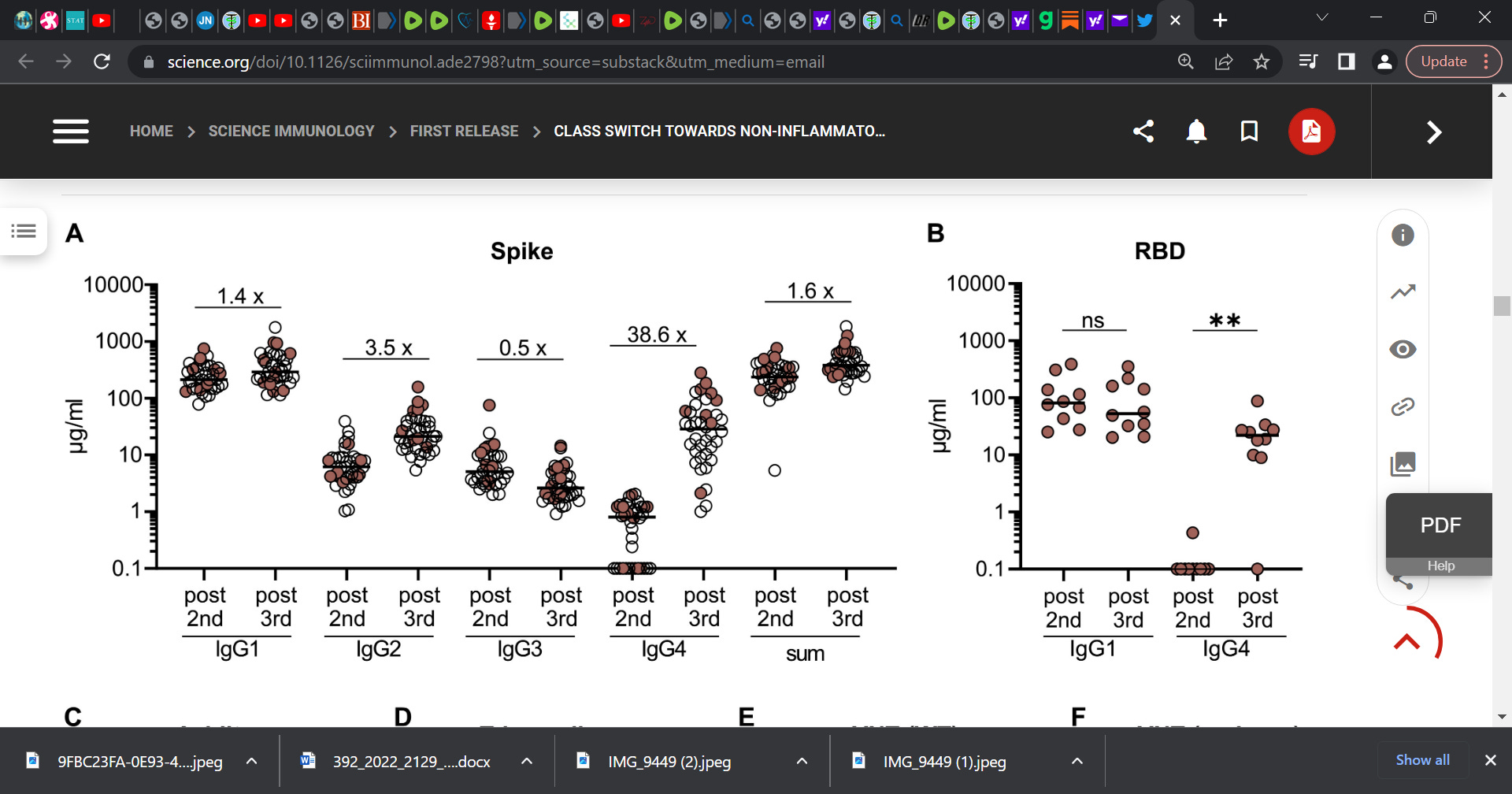
‘We report that several months after the second vaccination, SARS-CoV-2-specific antibodies were increasingly composed of non-inflammatory IgG4, which were further boosted by a third mRNA vaccination and/or SARS-CoV-2 variant breakthrough infections. IgG4 antibodies among all spike-specific IgG antibodies rose on average from 0.04% shortly after the second vaccination to 19.27% late after the third vaccination. This induction of IgG4 antibodies was not observed after homologous or heterologous SARS-CoV-2 vaccination with adenoviral vectors.’
Question is, so what? We knew that IgG4 has the far least role in immune response that other classes have. ‘The pathophysiology of the disease is complex and should start with the description of the IgG4 molecule. IgG4 has a concentration of less than 5% of total IgG immunoglobulins, being the subclass with the most stable interindividual concentration. IgG4 does not activate the classical complement pathway and plays a limited role in the immune process.’ (see R Opriţă et al.).
Researchers also reported:
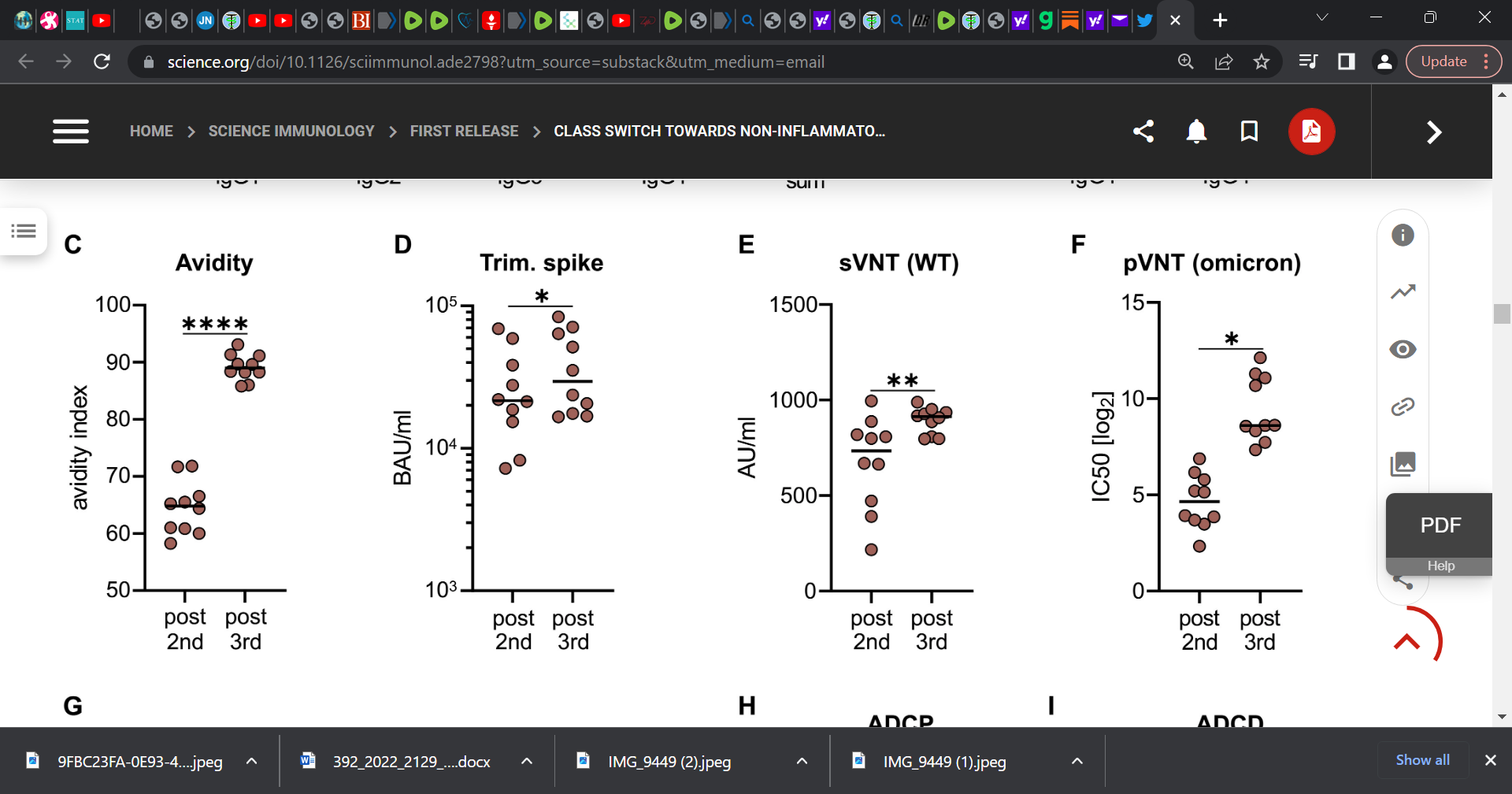
‘improved avidity and neutralizing potential of vaccine-induced antibodies after the third vaccination (9–11). However, the large number of breakthrough infections caused by the Omicron variant indicates that current vaccination regimens do not confer sterilizing protection.’
So with this finding, again, so what? We knew the vaccine fails, does not neutralize or sterilize the virus. Is this a real concern? In some sense yes when we consider the reporting “Importantly, this class switch was associated with a reduced capacity of the spike-specific antibodies to mediate antibody-dependent cellular phagocytosis and complement deposition.”
This is a concern.
We need to unpack this with further study (reduced antibody-dependent cellular phagocytosis and complement deposition post booster) as it raises questions as to the role of the boosters in hobbling or hampering immune system response.
Further:
‘Several months after the second vaccination, SARS-CoV-2-specific antibodies were increasingly composed of non-inflammatory IgG4, which were further boosted by a third mRNA vaccination and/or SARS-CoV-2 variant breakthrough infections…
Single-cell sequencing and flow cytometry revealed substantial frequencies of IgG4-switched B cells within the spike-binding memory B-cell population (median 14.4%; interquartile range (IQR) 6.7–18.1%) compared to the overall memory B-cell repertoire (median 1.3%; IQR 0.9–2.2%) after three immunizations…
Importantly, this class switch was associated with a reduced capacity of the spike-specific antibodies to mediate antibody-dependent cellular phagocytosis and complement deposition. Since Fc-mediated effector functions are critical for antiviral immunity, these findings may have consequences for the choice and timing of vaccination regimens using mRNA vaccines, including future booster immunizations against SARS-CoV-2.’
‘There are very few reports on the induction of IgG4 after natural infection with SARS-CoV-2. The dominant subclasses were mostly IgG1 and IgG3 (54–56). Nevertheless, a Brazilian study during the early phase of the pandemic correlated an early onset and high levels of anti-spike IgG4 antibodies with a more severe COVID-19 progression after SARS-CoV-2 infection, which might indicate a less effective antibody response (56).’
Key statement:
‘In our study, antibody-mediated phagocytic activity and complement deposition were reduced in sera after the third immunization, in parallel to higher proportions of anti-spike IgG4 antibodies. However, how these changes affect subsequent virus infections remains unclear.’
The researchers are raising the alarm and the mechanism or role is yet understood. This warrants study and in terms of applicability of mRNA-based vaccine against other pathogens. IMO, the mRNA with LNP platform is very dangerous, not yet studied, and it is not understood and must be stopped. So far, the only parties to have benefitted are the vaccine makers, patent holders, and government alphabet agency officials. People, vaccinees, have died due to this gene platform. We need to understand the underlying immunological mechanisms underpinning this class switch.
Researchers further reported: ‘In summary, our study demonstrates an mRNA vaccine-induced antiviral IgG4 antibody response appearing late after secondary immunization. Further investigations are needed to clarify the precise immunological mechanisms driving this response and to evaluate whether an IgG4-driven antibody response affects subsequent viral infections and booster vaccinations. This is not only relevant for potential future vaccine campaigns against SARS-CoV-2, but also for new mRNA-based vaccine developments against other pathogens.’
See class IgG4:

Please consider an annual subscription (paid) for $39.99 ($3.30 month); your support is appreciated to help me disseminate the knowledge that is blocked by mainstream media; help me fight the censorship I and others have been faced with
Dear Readers,
I also embed this short piece on The Wellness Company and The UNITY Project.
First, The Wellness Company.
I am proud to announce a unique partnership with The Wellness Company and everyone who believes in medical freedom. My dear and esteemed colleagues Dr. Peter McCullough and Dr. Harvey Risch are also in partnership with The Wellness Company which provides telemedicine services for long-haul COVID, vaccine injury, and medical exemptions along with supplements and products that are fully aligned with our values. This support for The Wellness Company stems from the sub-optimal medical care and response that we experienced throughout the pandemic. It became apparent that there are many glaring gaps in our healthcare system and people were not properly treated. Thus, the pivot by us to support The Wellness Company. Take a stand against a broken healthcare delivery system with a membership in The Wellness Company, which directly funds our fight against medical tyranny. Click here The Wellness Company for more information.
I also provide scientific support to The UNITY Project out of California. A magical organization for good. I support this tremendous initiative with some fine colleagues who have been warriors in the fight against all the wrongs in COVID. The UNITY Project aligns with my core values for it is very fierce in its fight to protect children from the danger of the largely safety untested COVID gene injection (The Unity Project Formed by Concerned Parents to Coordinate Opposition to California's K-12 COVID-19 Vaccination Mandate) (contact: info@theunityproject.org).
Thr unholy trifecta of ADE, immune fixation and now immune tolerance = VAIDS.
It is NOT a vaccine!