

Ammirati et al.: "Temporal relation between second dose Pfizer BNT162b2 mRNA Covid-19 vaccine and cardiac involvement in a patient with previous SARS-COV-2 infection"
we do have indications from Krammer, Raw et al. that such persons with prior infection are at greater risk of adverse effects when COVID vaxx immunity is layered on top of prior infection

SOURCE:
https://www.sciencedirect.com/science/article/pii/S2352906721000622?via%3Dihub
This case highlights a potential relation between the second dose of a COVID-19 vaccine and acute myocarditis in an otherwise healthy patient with a previous exposure to SARS-COV-2 infection.
‘An otherwise healthy 56-year-old man presented to the emergency department complaining of acute onset of chest pain 3 days after the second dose of BNT162b2 mRNA COVID-19 vaccine. He did not report fever, systemic symptoms or cutaneous rash after the first and second dose of the vaccine. He had no history of allergy. Nine months earlier he experienced mild signs of COVID-19 infection with fever lasting for 3 days and cough for 1 week, but he did not complain of chest pain or dyspnea. He was not hospitalized, and he took only acetaminophen.
Nasopharyngeal swabs by real-time reverse-transcriptase–polymerase-chain-reaction (rRT-PCR) assay, had been persistently positive for 1 month while he did not undergo any blood tests during that period. One month later, anti-SARS-COV-2 serology demonstrated presence of IgG anti S1 and S2 proteins (titer of 60 AU/mL with positive threshold above 15).
On arrival at the emergency department arterial blood pressure was 165/95 mmHg, heart rate 81 beats per minute, oxygen saturation 99% while breathing ambient air and body temperature 36.2 °C. Electrocardiogram (ECG) showed sinus rhythm, and minimal ST elevation on precordial leads, with peaked T waves. The chest x-ray was unremarkable (Supplemental Fig. 1A-B). Laboratory tests revealed elevated levels of biomarkers of myocardial necrosis, i.e. high-sensitivity (hs) troponin T 289 ng/L, and C-reactive protein 2.9 mg/L with normal blood cell counts, without evidence of peripheral eosinophilia (Table 1). Urgent coronary angiography carried out to rule out an acute coronary syndrome (Fig. 1A-B). Cardiac ventriculography showed preserved global left ventricular function. Chest pain resolved spontaneously within 4 h of admission. The patient was therefore transferred to the cardiology ward with a diagnosis of suspected acute myocarditis.
He underwent nasopharyngeal swabbing and the specimens were tested for common respiratory viruses by RT-PCR and resulted all negative. As expected, anti-SARS-COV-2 serology revealed a high-titer of IgG anti S1 and S2 proteins (titer > 400 AU/mL), and positive anti-nucleocapsid antibodies due to previous exposure. Hs-troponin T and CK-MB peaked on day 1 with values of 515 ng/L and 27 µg/L, respectively. No specific anti-inflammatory or steroidal therapy was administered, and CK-MB normalized at day 5 while hs-troponin T normalized within 7 days. Cardiac MRI showed non-dilated ventricles with preserved left (63%) and right ejection fraction (60%). There was focal subepicardial-intramyocardial (non-ischemic pattern) late gadolinium enhancement (LGE) involving the basal and apical segments of the infero-lateral wall, colocalized with signs suggestive for edema on T2 weighted images (Fig. 1C-1D), consistent with the diagnosis of acute myocarditis [7].’
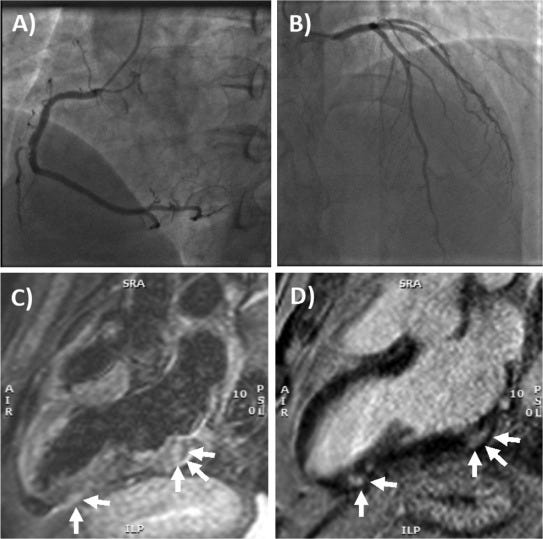
‘Fig. 1. Coronary angiography and cardiac MRI. (A) The right coronary artery only had a mild plaque (<30% luminal diameter) in the mid portion, while (B) left main stem, left anterior descending artery and circumflex artery had no evidence of coronary plaques. (C) T2- weighted 3-chamber view on cardiac MRI, showing focal areas of edema involving the subepicardial-intramyocardial regions of the basal and apical segments of the infero-lateral wall (arrows). (D) Late gadolinium enhancement confirmed the presence of non-ischemic myocardial lesions in the basal and apical segments of the infero-lateral wall (arrows) consistent with acute myocarditis.’
Remember when some folks talked about hybrid immunity? It was more lies to pump up the profits of Big Pharma
It's presumptious and premature to think that SARS-CoV-2 infection causes only a mild respiratory illness. Numerous serious illnesses including polio and HIV begin with mild flu-like symtoms. To give an mRNA injection to someone who has had covid is reckless endangerment.