

Canadian Bridle unravels a flawed study in his substack: "Let's See How COVID-19 'Vaccine' Papers Can Be Misleading; Don't Use Bad Science To Push More RNA Shots"
The paper is entitled “Repetitive mRNA vaccination is required to improve the quality of broad-spectrum anti–SARS-CoV-2 antibodies in the absence of CXCL13”; a fatally flawed experimental design!

Start Bridle’s excellent scholarship here:
‘A colleague and friend asked me what I thought of a recent publication. For the benefit of others, I will provide a critique of it here. Why is this important?
Because it shows people how to differentiate the experts they should be listening to from those who stand on a foundation of fatally flawed science.
The Paper
The paper is entitled “Repetitive mRNA vaccination is required to improve the quality of broad-spectrum anti–SARS-CoV-2 antibodies in the absence of CXCL13”, and it can be found here (Da Silva, et al., 2023).
Overview
The paper assesses antibody responses targeting two proteins from severe acute respiratory syndrome-coronavirus-2 (SARS-CoV-2), which is the causative agent in some people of the coronavirus disease that was identified in 2019 (COVID-19). Specifically, the amount and quality of antibodies were evaluated in four groups of people, including:
Those that had been infected with SARS-CoV-2 and then recovered, thereby having naturally acquired immunity.
Those with naturally acquired immunity who were subsequently treated with a COVID-19 shot containing modified synthetic RNA molecules encased in lipid nanoparticles (henceforth called a ‘COVID-19 shot’).
Those that received two COVID-19 shots.
Those that received three COVID-19 shots.
Although the title seems to imply that multi-dosing beyond the two standard doses is necessary, it is misleading. In fact, when one reads the concluding paragraph, the authors failed to provide any meaningful clinical advice. In fact, the data in the paper can be used to draw an important and obvious conclusion that authors chose to ignore: COVID-19 shots offer no benefit over and above naturally acquired immunity.
Let’s begin a thorough review. This is how an expert dissects a paper before drawing their own conclusions…
Starting on the Wrong Foot: A Misleading Title
First, there is a mistake in the title. The paper is not about anti-antibodies, which are antibodies that bind to other antibodies. Rather, it is about ‘SARS-CoV-2-specific antibodies’, also known as ‘antibodies against SARS-CoV-2’; these are very different. I would recommend that the authors familiarize themselves with this difference by reading the following paper…
Gell PG, Kelus AS. Anti-antibodies. Advanced Immunology 1967;6:461-78. doi: 10.1016/s0065-2776(08)60526-x. PMID: 4167364.
Second, the title implies that the data in the paper support taking three COVID-19 shots. Indeed, many ‘experts’ have already parroted this message to promote this concept. But, the data do not support this. Instead, the latter half of the title holds the important message. The authors provide convincing data showing two fundamental flaws with the COVID-19 shots that make them far from being ideal vaccines. As a result of these inherent weaknesses in the technology, if people want to artificially maintain peak, yet far from optimal COVID-19 shot-induced immune responses, they will be compelled to take endless shots at ridiculously short time intervals.
A more accurate title for the paper would be:
Naturally acquired immunity from a single exposure to SARS-CoV-2 proved to be superior to COVID-19 shot-induced immune responses, even when using a three-dose regimen, and even when the research was designed with biases to favour the shots.
The Introduction
Scientific papers begin with an overview of relevant background science so the reader can understand what is being discussed with respect to the new research. It also provides the rationale for the research (i.e., the reason why it was worth doing the study in the way it was performed) and lists the objectives of the study. What this particular introduction lacked was a hypothesis. This is when someone predicts the outcome of the research based on their understanding of the underlying science. The experiments then determine whether the hypothesis was correct or not. Hypothesis-driven research is considered the gold standard in science. Studies that lack a hypothesis are sometimes referred to as ‘fishing studies’. So, this was a fishing study.
“Since the initial SARS-CoV-2 […] pandemic related to the Wuhan strain, several viral variants have emerged. These variants […] represent a major challenge for immune control, especially in the context of vaccination. Most of the mutations that differentiate these strains from the original isolate are localized in the two domains of the spike (S) protein”
…I agree. What is implied but not clearly stated (and should be) is that this is less of a challenge in the context of naturally acquired immunity. New variants have a tougher time evading naturally acquired immunity, which is much broader than COVID-19 shot-induced immune responses. It targets multiple proteins, including ones that are not mutating nearly as quickly as the spike protein, which is the only target for the shots.
“An incomplete natural immunity against variants has been also reported in convalescent individuals, who displayed lower quality of Fc-mediated antibody responses compared to individuals vaccinated with two“
…this is only partially true. The authors failed to place this into the context of COVID-19 shots, which is essential for people to make informed decisions. Like all endemic viruses that we live with, SARS-CoV-2 can change over time (likely accelerated by the use of shots that apply a non-lethal selective pressure), rendering it able to begin evading immune responses against fundamentally different historical versions of the virus. However, naturally acquired immunity wanes far slower than the shot-induced immune responses. The claim about people with naturally acquired immunity having “lower quality” antibody responses is simply not true and based on a scientific sleight of hand. People who have received two shots will have mounted what immunologists call a ‘secondary immune response’. Those who have recovered from an infection will have mounted a ‘primary response’. Antibodies are qualitatively superior during a secondary response. A person exposed to second infection with SARS-CoV-2 would also mount a secondary immune response in which the antibodies would be of better quality. So, this is an ‘apples versus oranges’-type of trick in science.
A second aspect to this scientific deception is that, ‘Fc-mediated responses’ refers to just one of several ways that antibodies can eliminate viruses from the body. Evaluating just one of these mechanisms leads to an underestimation of how protective antibodies really are.
Yet another ‘trick’ used to argue the failure of naturally acquired immunity over time is by limiting testing such that only immune responses against the spike protein, which is the most rapidly mutating part of the virus, are evaluated. What gets left out of most studies is an assessment of naturally acquired immunity against the non- or slow-mutating proteins. These studies would show that naturally acquired immunity remains more effective than spike-specific immunity. However, conducting this fair analysis would highlight that COVID-19 shots fail to confer any protection against these other targets.
In summary, it takes longer for naturally acquired immunity to become irrelevant and, when it does, the partial protection that remains will mean that most people will experience, at most, only mild disease when exposed to a downstream variant. The authors wrote a highly biased introduction.
“While most of the studies have assessed the role of neutralizing IgG [a type of antibody], little is known about mucosal humoral response induced by vaccines. Studies including ours have shown that, early after SARS-CoV-2 infection, a dominant IgA humoral response is induced against the nucleocapsid (N) and S proteins . The presence of IgA [they mean ‘the presence of IgA in the respiratory tract, not the blood’] in vaccinated individuals would be extremely important in the event of further contact with the virus, particularly during the first days of infection. The IgA in the mucosal tissue could limit viral dissemination and disease outcome, but little is known on the delay and durability of this response in individuals, with or without previous infection, who have received a vaccine boost.“
…there is a lot to unpack here…
“little is known about mucosal humoral response induced by vaccines.“
Sadly, this is true. Studying antibody responses in the respiratory system has largely been ignored despite this being the most relevant place to look. After all, this is where SARS-CoV-2 infects people and this is where people need antibodies if they are going to have a chance of avoiding COVID-19 and preventing transmission of SARS-CoV-2 to others. Sadly, the authors of this study failed to contribute any knowledge to this area. So, including this in the text is misleading. Their data have nothing to do with ‘mucosal (respiratory) immunity’.
“Studies including ours have shown that, early after SARS-CoV-2 infection, a dominant IgA humoral response is induced against the nucleocapsid (N) and S proteins.“
IgA and IgG are two of five types of antibodies. The authors mean ‘antibody response’ when they say “humoral response”. This particular statement is true and important to note. This confirms that naturally acquired immunity targets more than just the spike protein of SARS-CoV-2. It also targets what is called the ‘nucleocapsid protein’ (or ‘N’ protein), as well as other components of the virus that were not listed. Remember, COVID-19 shots only target the spike. This becomes important later on.
“The presence of IgA in vaccinated individuals would be extremely important in the event of further contact with the virus, particularly during the first days of infection.“
This statement is misleading. It implies that the authors conducted research on IgA that is relevant to protection against infection with SARS-CoV-2. They did not do such research. Instead, the authors studied IgA in the blood, which is not the relevant location. They should have studied IgA in the airways where it is relevant to infection. When saying “The presence of IgA” they actually mean ‘the presence of IgA in the respiratory tract, not the blood’.
“The IgA in the mucosal tissue could limit viral dissemination and disease outcome“
“Mucosal tissue” means ‘the airways’. This is absolutely true, but the authors’ research did nothing to address this. We know that naturally acquired immune responses are great at inducing a form of IgA in the airways that is called ‘secretory IgA’. In contrast, injecting COVID-19 shots into the shoulder muscle is good at inducing what is called ‘circulating IgA’ in the blood, but poor at getting these antibodies produced in the airways. The authors looked in the blood, not the relevant location.
“but little is known on the delay and durability of this response in individuals, with or without previous infection, who have received a vaccine boost.“
True, but two highly relevant groups have generally been left out of the historical literature in this area:
a. People with naturally acquired immunity and no ‘vaccine boost’. Thankfully, the data in the paper being discussed does address this.
b. People with naturally acquired immunity from a single infection that have been boosted by a second natural infection. My educated guess is that these responses induced by a natural prime-boost regimen would be very impressive.
Results Section
The groups of people that were studied:
“To determine the impact of mRNA vaccination boosts, we analyzed humoral responses in different groups of donors. Individuals included (i) nonvaccinated convalescent individuals, from whom samples were collected 6 months after SARS-CoV-2 infection; (ii) convalescent individuals vaccinated with BNT162b2 (1 to 3 months after vaccination), so called hybrid immune responders; and (iii) individuals only vaccinated with two doses (samples collected at two time points: 1 to 3 months after vaccination and 4 to 6 months after vaccination) or (iv) with three doses of mRNA vaccines (1 to 2 months after vaccination) and a group of naïve individuals as a negative control“
…this section of the text is extremely important because it reveals fatal flaws with this study. A fatal flaw is one that should prevent a paper from being published and that should trigger a retraction if such a paper was published.
Five groups of people were studied. One group had naturally acquired immunity from a single infection with SARS-CoV-2. The second group had naturally acquired immunity that was boosted with a COVID-19 shot. The third and fourth groups lacked naturally acquired immunity but had immune responses induced by two or three COVID-19 shots, respectively. The fifth group were stated as being “naïve”, meaning that they lacked immune responses against SARS-CoV-2. This latter concept was a major misconception during the declared pandemic. Many people failed to recognize that there was clear evidence early on that some of the immunity that people had against other coronaviruses could cross-react with (meaning ‘also recognize’) SARS-CoV-2 to a certain degree (Majdoubi, et al., 2021). Indeed, one of the ‘naïve’ individuals in the current paper being discussed had a weak but detectable antibody response against the spike protein (Figure 1c of the paper).
Fatal Flaw #1: Timing of Blood Sampling
In the quote above, I bolded the times at which blood samples were taken from the groups that were studied. Note that they vary substantially. Most importantly, the group with the longest delay between the initiation of an immune response and taking a sample to study that response was for those with naturally acquired immunity. Isn’t that interesting!
To be fair, blood sampling should have been done in all groups at the peak of each response, or at the end of the response when a plateau has been reached. As can be seen in the schematic below, blood sampling was done in a way that biased the results towards showing superior antibody responses against the spike protein in people that had received COVID-19 shots…

Fatal Flaw #2: Failure to Account for ‘Primary’ and ‘Secondary’ Immune Responses
The first time the immune system mounts a response against a target, we call that a ‘primary immune response’. If the immune system sees the target a second time, the resultant response is called a ‘secondary response’. After that, a person mounts a ‘tertiary [third] response’, etc. The difference between primary and secondary (or subsequent) responses is profound. Primary responses are of relatively low magnitude. In stark contrast, secondary responses are of much higher magnitude. Secondary responses are also usually qualitatively superior. This is why we usually don’t get sick if we get infected with the same virus a second time; the immune response clears the virus before it can cause disease.
So, to compare primary responses to secondary or further downstream responses is like comparing apples to oranges. This is precisely what the authors did in this paper, but they failed to discuss this. For the group with naturally acquired immunity, the authors do not identify how many infections these people had recovered from. However, since the sampling was done relatively early in the declared COVID-19 pandemic, it is likely that most, if not all of these people had experienced a single infection. In other words, what was being studied in the group with naturally acquired immunity was predominantly a primary immune response. In stark contrast, what was being studied in every other group in this study that had received a COVID-19 shot was a secondary or even tertiary immune response. In other words, they compared apples to oranges; a weaker response (but one that results in excellent downstream protection) to inherently robust responses. Keep this in mind, because I am going to show you that the data in this paper prove the superiority of naturally acquired immunity despite this massive bias.
Also, remember that almost everyone on earth has now been subjected to multiple infections with SARS-CoV-2, which means that almost all people who did not take COVID-19 shots have naturally mounted robust secondary or tertiary immune responses. Despite this fact, I have yet to see anyone compare a naturally acquired secondary immune response to the responses induced by the COVID-19 shots. In other words, looking at people who recovered from an initial infection followed by a second infection (likely with mild disease, at most) with a variant that had mutated enough to begin partially evading the initial immunity. I hypothesize that natural secondary responses would blow shot-induced responses out of the water.
Fatal Flaw #3: Ignorance of Naturally Acquired Immunity is Not a Justification for More Shots
The authors of this paper used a dirty trick to make it appear that all people need COVID-19 booster shots. Specifically, check out this statement…
“Together, our results confirm the need for repeated administration of mRNA vaccines, with at least three doses to induce a humoral response against S like that seen in individuals previously infected by SARS-CoV-2 and boosted with mRNA vaccine.“
Let me break this statement down. First, by ‘humoral response’, the authors mean ‘antibody response’. There is far more to a ‘humoral’ response than just antibodies, but they only assessed the latter. Second, note that they have limited this statement to the ‘S’ protein of SARS-CoV-2, which is the spike. This is the key to the false conclusions that many people draw from papers such as this one. The authors want you to focus solely on the immune responses against the spike protein. If you do this, then many of their statements appear to be valid. As an expert in this area, I find this to be potentially nefarious and let me explain why.
The authors present data for antibody responses against the N protein of SARS-CoV-2, but then proceed to ask the reader to focus only on the spike-specific antibody responses. The N protein is a piece of what makes the SARS-CoV-2, just like the spike protein. Designers of COVID-19 shots targeted the spike because antibodies against this protein can ‘neutralize’ the virus. This means the antibodies can prevent the virus from infecting our cells. However, nucleocapsid-specific antibodies can neutralize SARS-CoV-2, just like spike-specific antibodies can (Dogan, et al., 2021). To translate, this means that the antibody response against the N protein can be just as protective as the response against the S protein. Now, let me show you why ignoring the immune response against the N protein in people that recovered from a natural infection is nonsensical…
I will start with an investment analogy. Let’s assess two investors. One has gone all-in on a single stock. The other is a diversified investor; they have invested their monetary resources into multiple stocks. The all-in investor has $1 million in a single stock. The diversified investor has $500,000 in each of three stocks, one of which is the same as investor #1. So, who is richer? If one only looks at the first stock, one would erroneously conclude that investor #1 is richer ($1 million versus $500,000). This would suggest that everyone should invest in a single stock. But this misses the obvious reality, which is that investor #2 is richer overall; richer by $500,000 to be exact ($1 million versus $1.5 million). So, in reality, you would want to mimic the strategy of the diversified investor.
Similarly, when it comes to immune responses against SARS-CoV-2, far too many people have been claiming that the ‘vaxxed’ are richer (have more antibodies) on the basis of looking at investments in a single stock (antibodies against the spike protein). But, those with naturally acquired immunity have diversified their investment into multiple stocks (antibodies against multiple proteins from SARS-CoV-2, including plenty against the spike protein, but also things like the N protein). Like the investment analogy, people with naturally acquired immunity are ‘richer’ than those who took the shots when one looks at the overall investment portfolios. Unfortunately, this common-sense reality has not been obvious to far too many medical and scientific ‘experts’.
And note that the above analysis, which favours those with naturally acquired immunity, would be even more exaggerated in their favour if a major bias were to be corrected. Specifically, the sampling timepoints that I mentioned earlier should have been equivalent across groups. Instead the samples were taken at a much later timepoint in those with naturally acquired immunity, which biased that group towards showing weaker antibody responses. This is like comparing the investment strategy of a teenager to that of a retiree. The latter has had a lot more time to accrue money; this does not mean their strategy was superior; the teenager could very well end up richer when they reach retirement.
Plus, the authors of the paper we are discussing made no mention of the fact that those with immune responses induced by COVID-19 shots would have T cell responses that can only recognize the spike protein. In contrast, those with naturally acquired immunity would have T cell responses against the spike, plus multiple other proteins from SARS-CoV-2. So, the investment analogy gets amplified even further in favour of the diversified investor when one takes into account other investments, such as mutual funds, etc.
So, if you were to take the investment analogy from above and account for both antibodies (investments in stocks) and T cells (investments in mutual funds), those who had three shots would have a total investment of: $1 million (for stocks in antibodies against spike) + $1 million (for mutual funds in T cells against spike) = $2 million overall.
But those with naturally acquired immunity have a total investment of: $500,000 (for stocks in antibodies against spike) + $500,000 (for stocks in antibodies against nucleoprotein) + $500,000 (for stocks in antibodies against other proteins) + $500,000 (for mutual funds in T cells against spike) + $500,000 (for mutual funds in T cells against nucleoprotein) + $500,000 (for mutual funds in T cells against other proteins) = $3 million. In other words, when the overall investment portfolios are analyzed, those with naturally acquired immunity are actually $1 million richer (not $500,00 when looking at antibodies only) than those who took the shots!
With these principles in mind, lets take the antibody responses against the spike protein that were disclosed in the paper and focus on the two extremes of the spectrum; those with naturally acquired primary immune responses (the diversified investor) versus those with tertiary COVID-19 shot-induced immune responses (the non-diversified investor)…
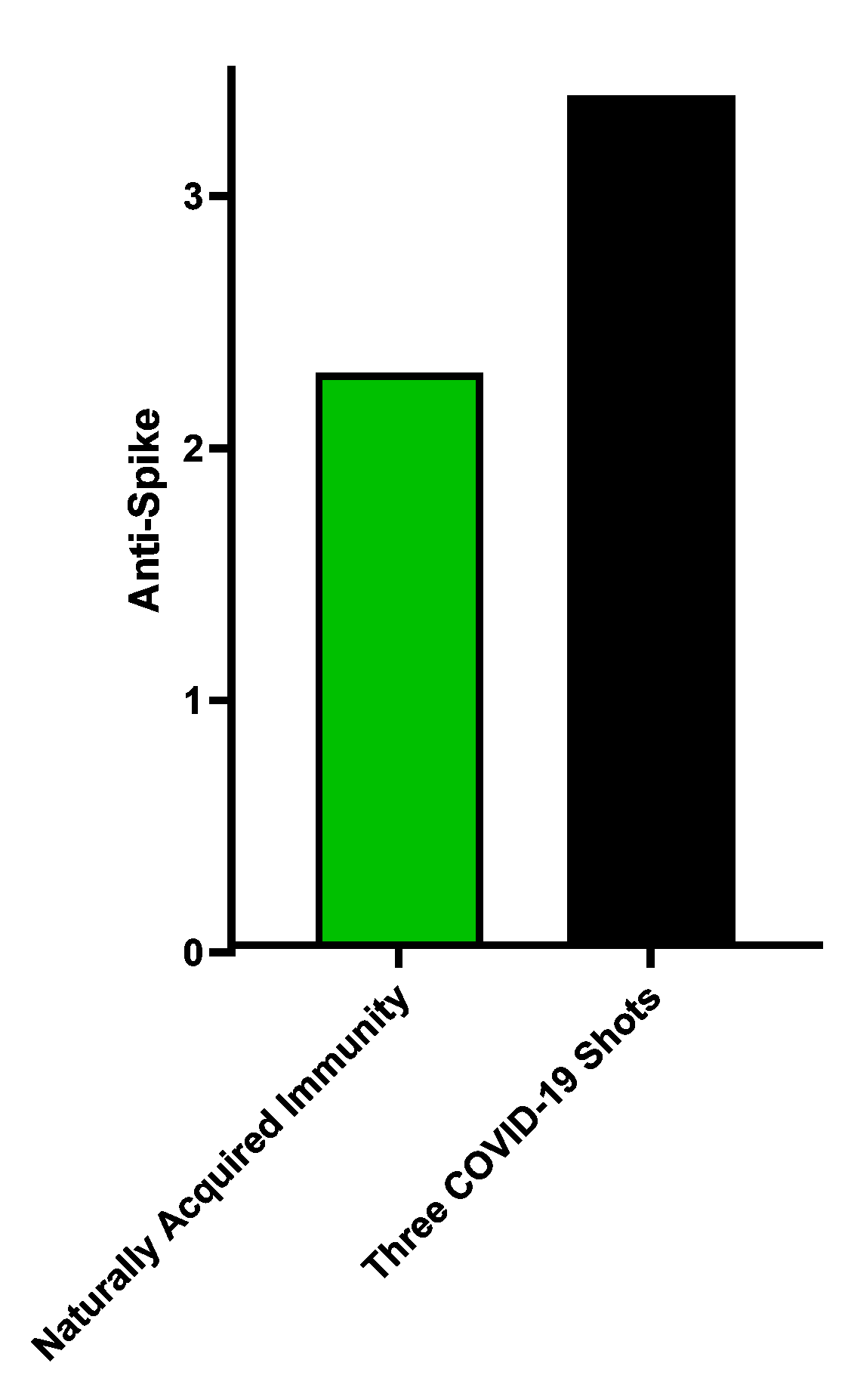
…it appears that targeting the spike protein with three COVID-19 shots is the better strategy, doesn’t it? But, here is what the antibody response against the N protein looked like…
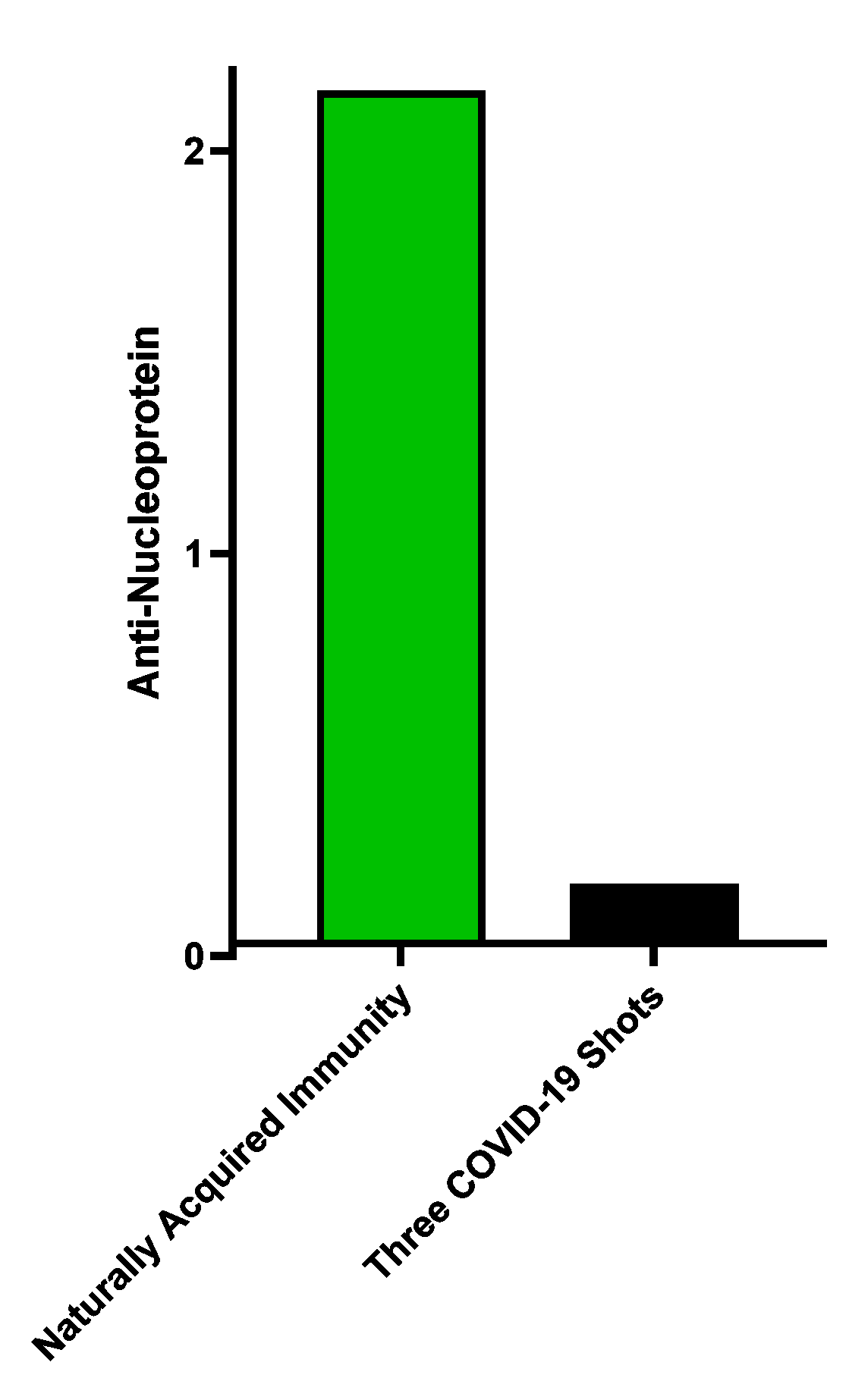
…now a very different conclusion is drawn. The antibody response is vastly superior to that in people who received the shots (who did not mount a response against this protein; what you see for the black bar is merely the ‘background signal’ for this test).
So, to be fair, lets take a look at what happens when these two response get added together…
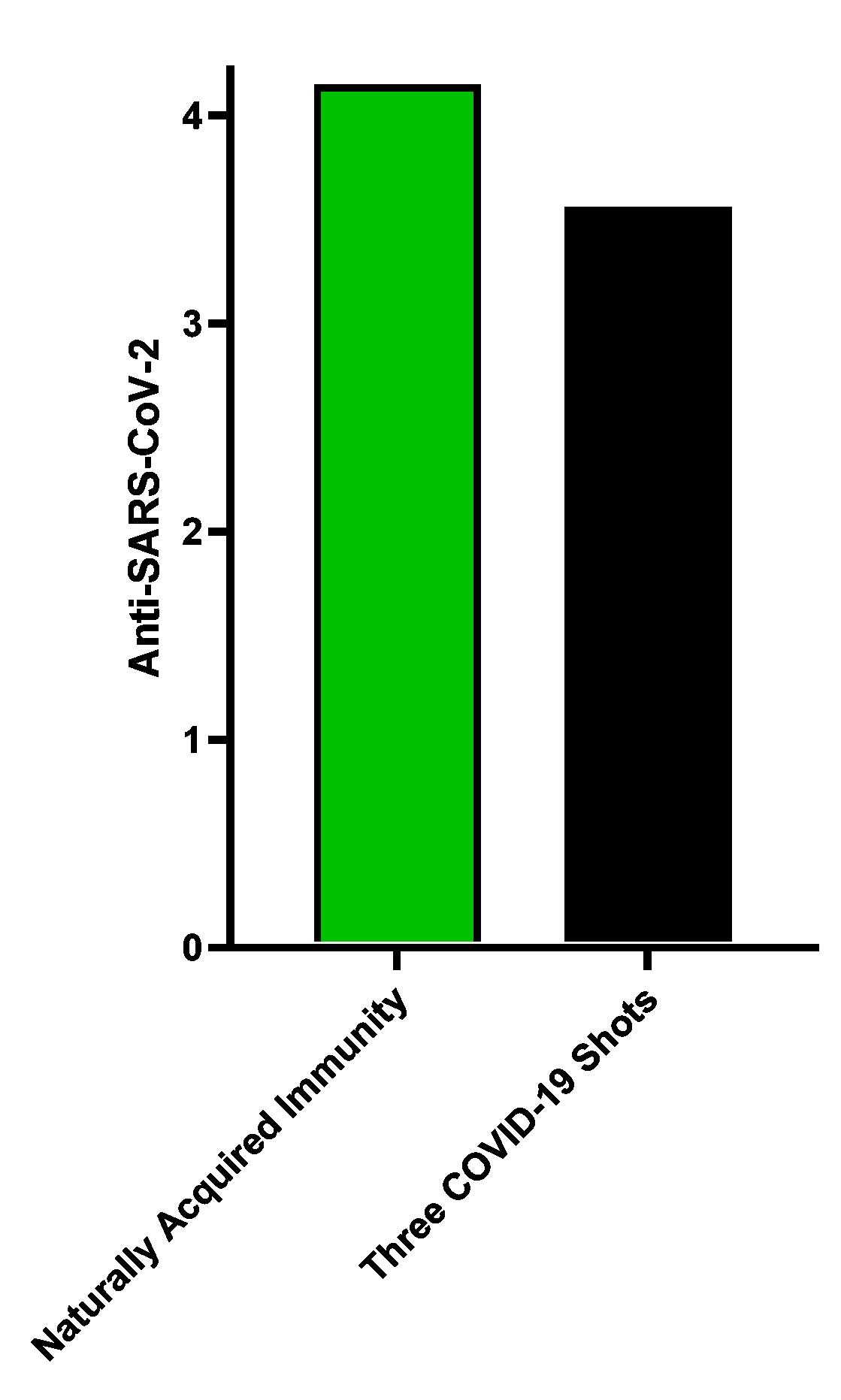
…once again, the diversified investment (naturally occurring immunity) beats the strategy of putting the whole nest egg in a single investment (COVID-19 shot-induced immune responses).
Keep in mind, that this paper only looked at responses against two pieces of the virus. If responses against the other parts were taken into account, this difference in favour of naturally acquired immunity would be further exaggerated. And this would be exaggerated even more if other aspects of the immune response were accounted for, such as T cell responses.
An Unwanted Side-Effect of COVID-19 Shots: Evidence of Immunological Imprinting
“Although the OD values of anti-N IgG antibodies were significantly different (P = 0.048), the levels of anti-S1 IgG were clearly higher in convalescents boosted with a vaccine dose (hybrid immunity, Pre + V: 3.37 ± 0.22) compared with nonvaccinated convalescent individuals”
As a scientist, I can tell you that this statement is incredibly biased and has no place in a peer-reviewed scientific publication. The authors admit that the magnitude of N-specific antibodies (not anti-antibodies) differed between people with naturally acquired immunity versus those that took COVID-19 shots despite having superior naturally acquired immunity. However, they refused to clearly state in which direction this difference occurred. So, let me clarify this. People with naturally acquired immunity who then had this ‘boosted’ with a COVID-19 shot (a secondary response) had significantly lower magnitude antibody responses against the N protein of SARS-CoV-2 than people who retained their primary natural immune responses. In other words, the ‘boost’ focused the immune response against the spike protein, which is the one that is most rapidly mutating. This caused an increase in spike-specific antibodies, but at the expense of the response against the N protein. And for all we know, this might hold true for the responses against all the other proteins.
This is a classic case of immunological imprinting, also sometimes called ‘original antigenic sin’. Shots given to people with naturally acquired immunity are reducing the breadth of the immune response against SARS-CoV-2. This makes it easier for the virus to mutate over time to evade these more narrowly-focused immune responses.
Pulling the Wool Over the Eyes of the Reader
Check out this statement made by the authors in their results section…
“The presence of IgA, boosted by the mRNA vaccine, could be of importance, since IgA is the most abundant antibody isotype in the mucosa, where these antibodies provide the first line of immune defense against pulmonary viral infections“
This is yet another highly misleading statement. First, these kinds of interpretive or contextual statements are not supposed to be in the results section of a paper. They are to be reserved for the later discussion section. This is to avoid introducing biases into the minds of readers so they can make fully objective assessments of the raw data that are presented in the results section.
Now, is the above statement inherently true? Yes, it is. But, the authors studied the presence of IgA in the irrelevant location of the blood, not the mucosal surface of the respiratory tract! What the authors of have done here is make a correct statement, but one that does not apply in any way to their own findings. This is a classical scientific ‘trick’ used to encourage readers to make erroneous connections between the actual results and what they mean in the real world.
So, to clarify, the results that the authors show are applicable to blood, which is not where the virus enters the human body. There is no direct link between what they found and what occurs in the lungs. In fact, it well known that a critical failure of the COVID-19 shots is that they were injected into the shoulder muscle, which is a great way to generate antibody responses in blood, but an ineffective way to get antibodies generated in the upper respiratory tract.
The Farcical Conclusion Drawn By The Authors
This paper enshrines many of the problems with COVID-19 science (and science in general, for that matter). ‘Experts’ will use the title, which says “Repetitive mRNA Vaccination is Required…” to claim this paper is proof that such a policy is essential. There are many other apparently compelling sound bites that can be generated from the main text of the paper. But they are garbage. As evidence provided from the authors themselves, check out the overall conclusion they were compelled to draw from their own work…
“In conclusion, in the context of the generalized third dose of vaccination, our study provides novel findings regarding the levels of protection and the impact of vaccine strategy to control the dynamics of COVID variants.“
Translation:
We presented a lot of garbage data encased among many misleading statements. Our data do not support pushing booster shots on anyone. In fact, our data clearly demonstrate the superiority of naturally acquired immunity if anyone is willing to look at the data in an objective fashion. As such, we are unable and, therefore, unwilling to provide any definitive clinical recommendations because the reality of our work contradicts the current narrative. But the good news is that our many misleading statements, including the title of the paper, can be taken out of context to provide excellent verbiage/evidence to be used in courts and by policy-makers.
What An Objective Conclusion Looks Like
First, the data in this study are impossible to interpret fairly due to a fatally flawed experimental design that biased the results heavily in favour of trying to demonstrate a benefit of COVID-19 shots. This issue was further confounded by the authors via their selectively biased interpretations. Long story made short, and based on the totality of the evidence provided by the authors, and even in the face of the heavy bias, naturally acquired immunity is as good as it gets. Overlooking this reality does not render it invalid. There is nothing in this paper that convinces me that people with naturally acquired immunity against SARS-CoV-2 require booster shots. In fact, the evidence provided by the authors suggests that getting booster shots risks narrowing the focus of naturally acquired immunity against a single target on SARS-CoV-2; a target that the virus has shown a propensity to mutate. And I suspect there are next to no people left on earth who have not been infected with and subsequently cleared SARS-CoV-2 from their body.
Having ignored this fact over the past three years makes all the harms perpetrated against those who didn’t take the shots and all the hatred that was heaped upon them, wrong.
Scientists Who Publish ‘Bad Science’ Should Be Held Accountable
Scientists who have ‘massaged’ their data to sell a particular narrative have revealed inherent biases and should have their papers retracted, and discipline stemming from academic misconduct should be considered.
Non-Experts Use Flawed Science to Accuse Others of Spreading Misinformation
What I have demonstrated here is how a genuine expert is able to break down and assess an extremely complicated, difficult-to-read scientific article. People who merely parrot statements made by authors of papers like this are not true experts. All they are doing is regurgitating hearsay evidence. Let this be a lesson for policy makers, judges, juries, and everyone for that matter, when they attempt to discern who they should be listening to.
Bridle expertly exposes the fraudulent faux 'scientists' in this particularly precise forensic analysis. Every so-called 'expert' using fraudulent papers to push the death-jab agenda is culpable and should be publicly stripped of any authenticity and credibility, jailed for a long minimum, and forced to undergo re-education along with the perp politicians romancing with the WEF. Could anyone please elect Dr. Byram Bridle to replace the entire Canadian federal cabinet so that we could again trust someone in government? I say we should seize the personal assets of everyone on the board of the College of Physicians and Surgeons of Ontario and award them to Dr. Bridle, to compensate him for their inexcusable abuse of an honest and decent truly talented doctor. Freedom Convoy 2 is on it's way east. Thank you Dr. Alexander for posting his paper for our education and ammo re-supply.
Enjoyed that very much ,Thankyou.