

COVID-19 vaccine-induced myocarditis (mRNA technology Moderna, Pfizer) in young persons (mostly male but female also) with chest pain, arrhythmias & cardiac arrest post mRNA shot; McCullough WARNS!
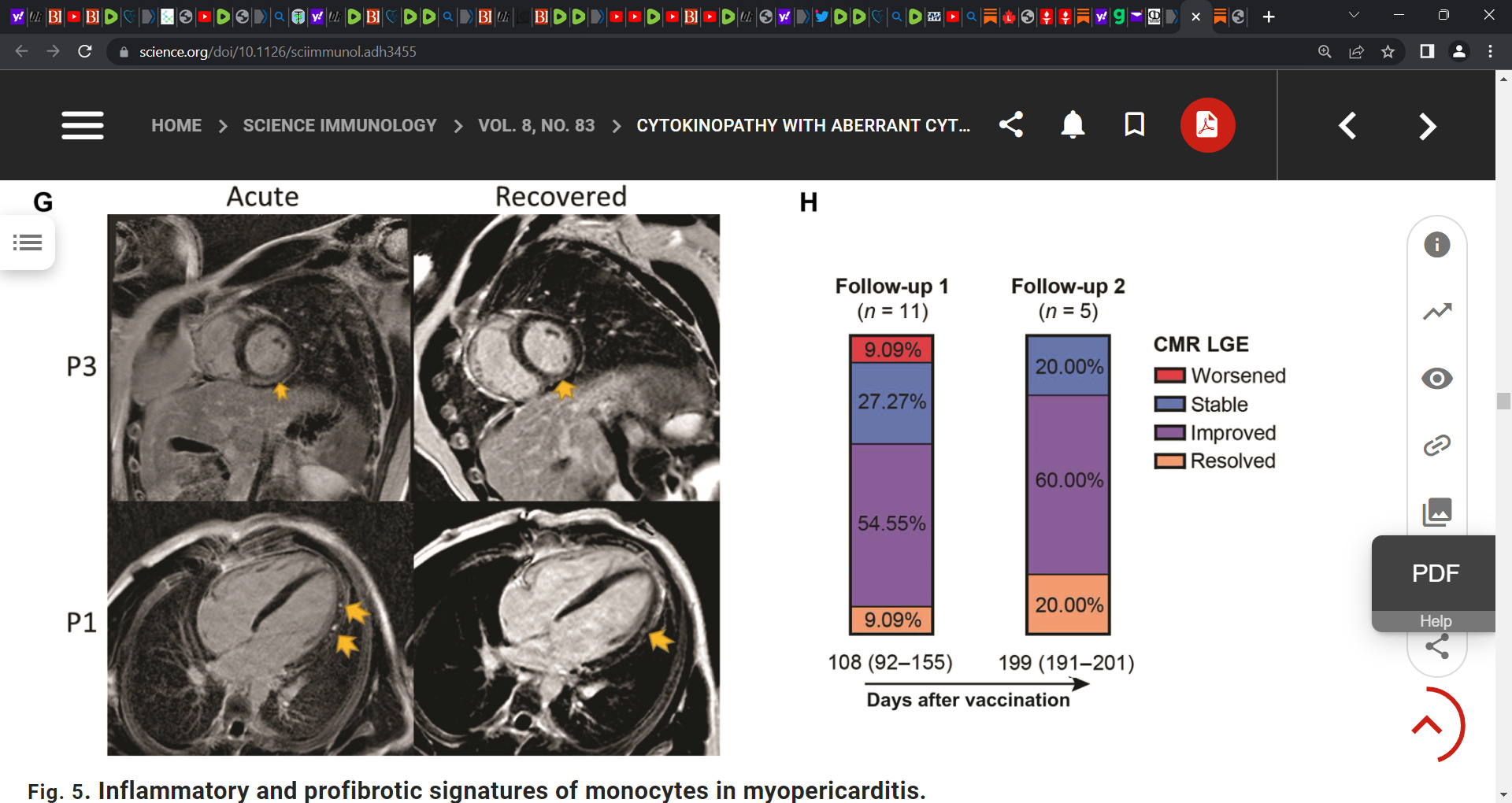
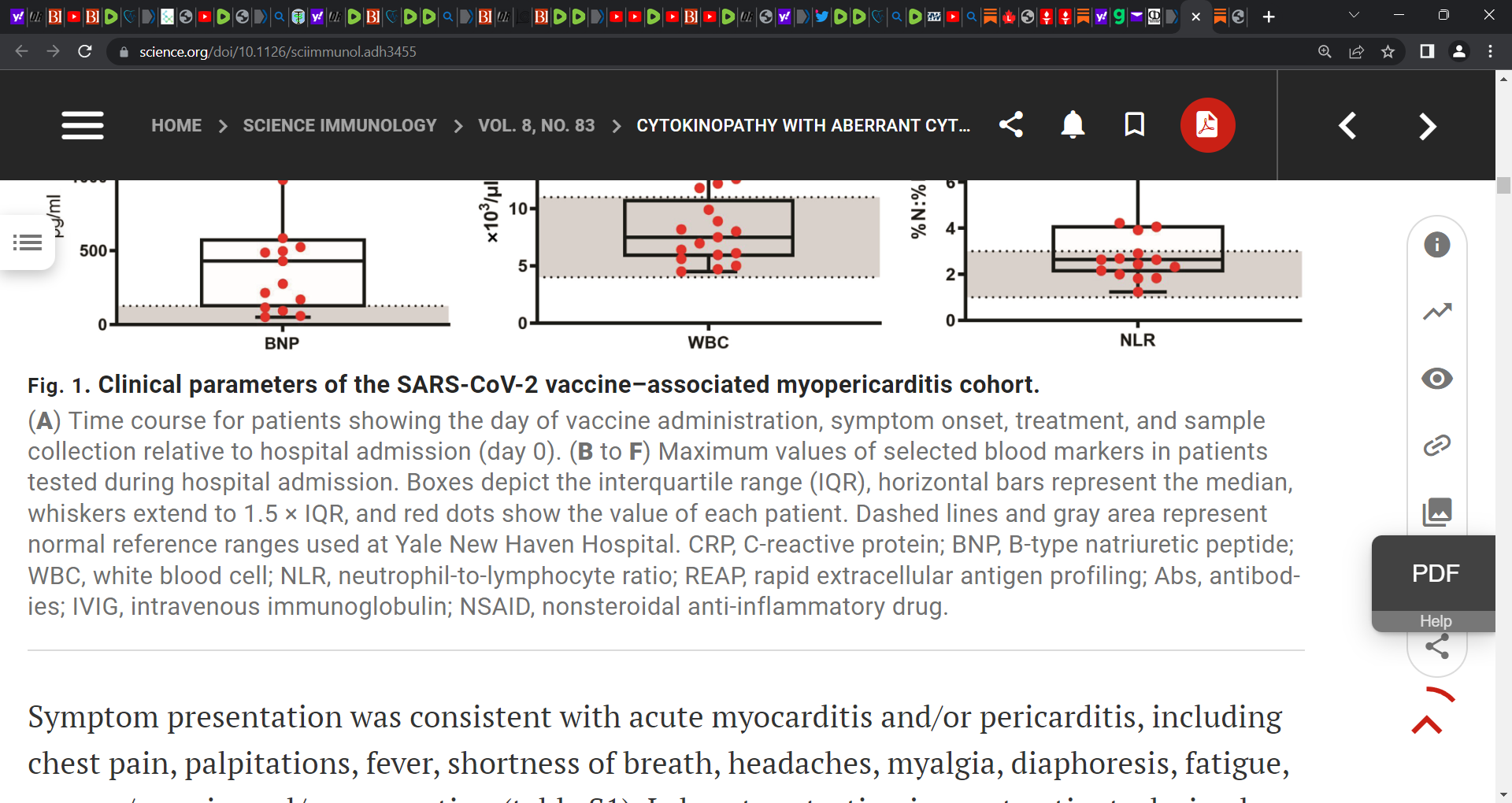
ongoing inflammation due to continued production of the vaccine-induced Spike protein (Pfizer or Moderna mRNA technology vaccines); McCullough cites Barmada et al. study; only 20% resolved at 6 mths


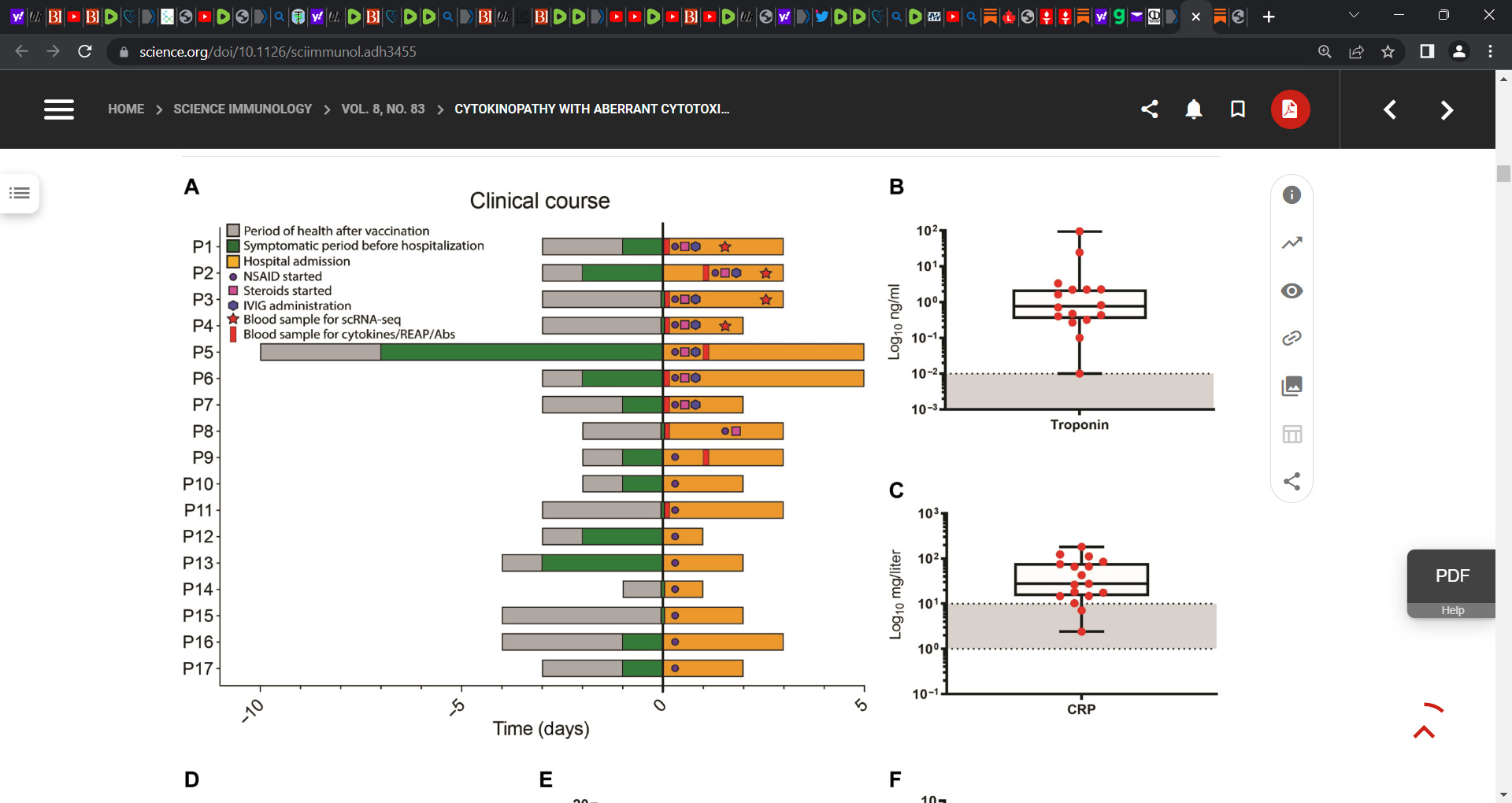
Critical piece of data that McCullough warns about whereby only 20% resolved at 6 months:
This suggests that there could be longer term cardiac damage post COVID mRNA technology based gene injection. Thus must cardiologists be on the lookout and to initiate tests e.g. EKGs, late contrast gadolinium chest MRIs? D-dimers? high-sensitivity troponin test?
We argue and McCullough and Oskoui and Stock and Thorp et al. have raised the issue of (including myself) the potential for cathecholamine surges e.g. adrenaline bathing the myocardial scarred heart and leading to cardiac arrest as the heart is placed under too much strain with the already sub-optimal electrical conduction across the scarred (dead) myocardial muscle. Is this a serious issue that those with silent myocarditis post shot must be concerend with?
How much risk are our children at now? Our teens? Those who are active. Pilots under stress?
Is this a ticking time bomb in someone post shot to go off one day with increased physical activity?
It is a debate that must take place and steps taken to exclude silent myocarditis as the outcome can be catastrophic.

See related research that adds to the discussion:
Circulating Spike Protein Detected in Post-COVID-19 mRNA Vaccine Myocarditis.
Yonker LM, et al. Circulation. 2023. PMID: 36597886 Free PMC article.
Cardiac MRI Findings of Myocarditis After COVID-19 mRNA Vaccination in Adolescents.
Chelala L, et al. AJR Am J Roentgenol. 2022. PMID: 34704459
SARS-CoV-2 vaccination and myocarditis or myopericarditis: population based cohort study.
Husby A, et al. BMJ. 2021. PMID: 34916207 Free PMC article.
Myocarditis With COVID-19 mRNA Vaccines.
Bozkurt B, et al. Circulation. 2021. PMID: 34281357 Free PMC article. Review.
COVID-19 Vaccine-Related Myocardial and Pericardial Inflammation.
Furqan M, et al. Curr Cardiol Rep. 2022. PMID: 36441403 Free PMC article. Review.
McCullough’s stack is excellent on this:

We have a mountain of evidence these shots should be pulled, but the agenda is to cull the herd. They have likely already doomed several Billion people to certain death- even if it takes a few years to accomplish the mission. All of these moves to tighten control over movement and communication are being set up to prevent any pushback once the sheeple realize what is going on. Peace and love.
I love it when the CDC and folks like the devil in carnate Peter Hotez claim that there's nothing to worry about since most cases of myocarditis are mild. Well, the clinical presentations could be mild to subclinical. But the intermediate and longterm sequelae are anything but mild. The risk for life altering cardiac disease is increased. In fact increased to the point where early death can be anticipate or if lucky, need for a hopefully successful heart transplant. The scar tissues advance all the time I believe. And if a patient continues to produce spike protein, and who really knows how long this occurs, the damage will only continue. IMHO these people require longterm medical management. And based on some insights related to research I was involved in, it's possible that management of post-myocarditis disease could be enhanced with the use of doxycycline which has antiinflammatory effects as well as the ability to inhibit matrix metalloproteinases (MMPs), the latter playing an important role in scar tissue advancement.