
COVID Bivalent booster vaccine effectiveness (VE) 'FAILS' again & Shrestha et al. shows us this: "Effectiveness of the Coronavirus Disease 2019 (COVID-19) Bivalent Vaccine"; VE of 30% (95% CI 20-39%)
COVID Bivalent booster vaccine effectiveness (VE) 'FAILS' again & Shrestha et al. shows us this: "Effectiveness of the Coronavirus Disease 2019 (COVID-19) Bivalent Vaccine"; VE of 30% (95% CI 20-39%)
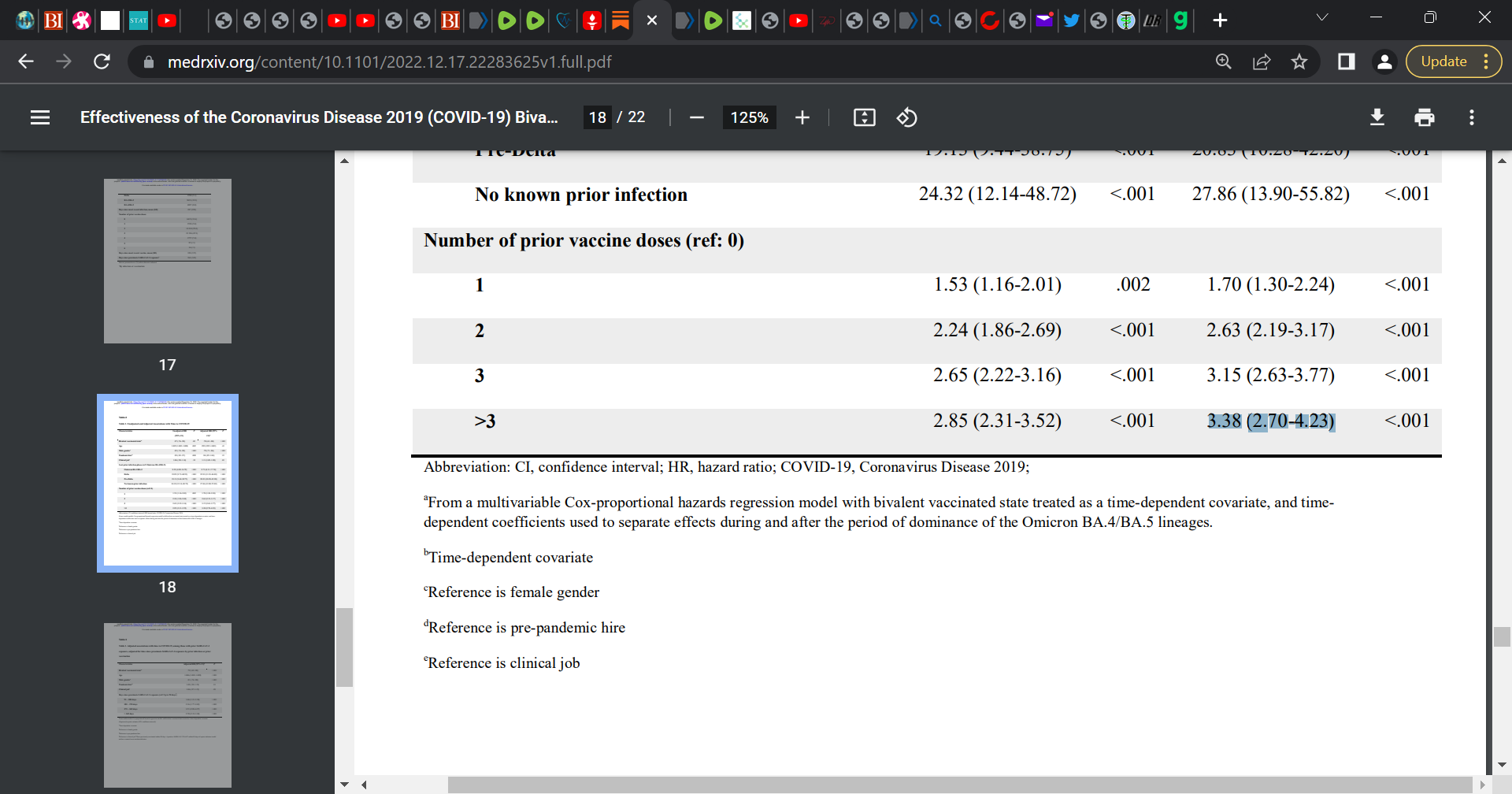
Multivariable analyses also found that the greater the number of vaccine doses previously received the greater the risk of COVID

Mass vaccination into a pandemic across all age groups and ‘rapid’ mass vaccination at that, while there is massive infectious pressure (circulating virus trying to infect the population) and using a non-neutralizing vaccine whereby the virus has become largely resistant to the vaccine induced antibodies (now non-sterilizing, non-neutralizing so does not stop infection, replication, or transmission), then selection pressure (natural selection) will select for the most fittest infectious variants that would become enriched in the environment and now become the dominant variants e.g. BQ.1.1 now replaces BA.5. There is original antigenic sin (OAS and I call it ‘mortal’ antigenic sin as the fixation cannot be reversed and prejudices the sub-optimal antibody response ‘life-long’) (immune priming and imprinting based on the initial prime or exposure), viral immune escape, and antibody-dependent enhancement of infection (ADEI) and disease (ADED).
This is what this study shows. OAS.
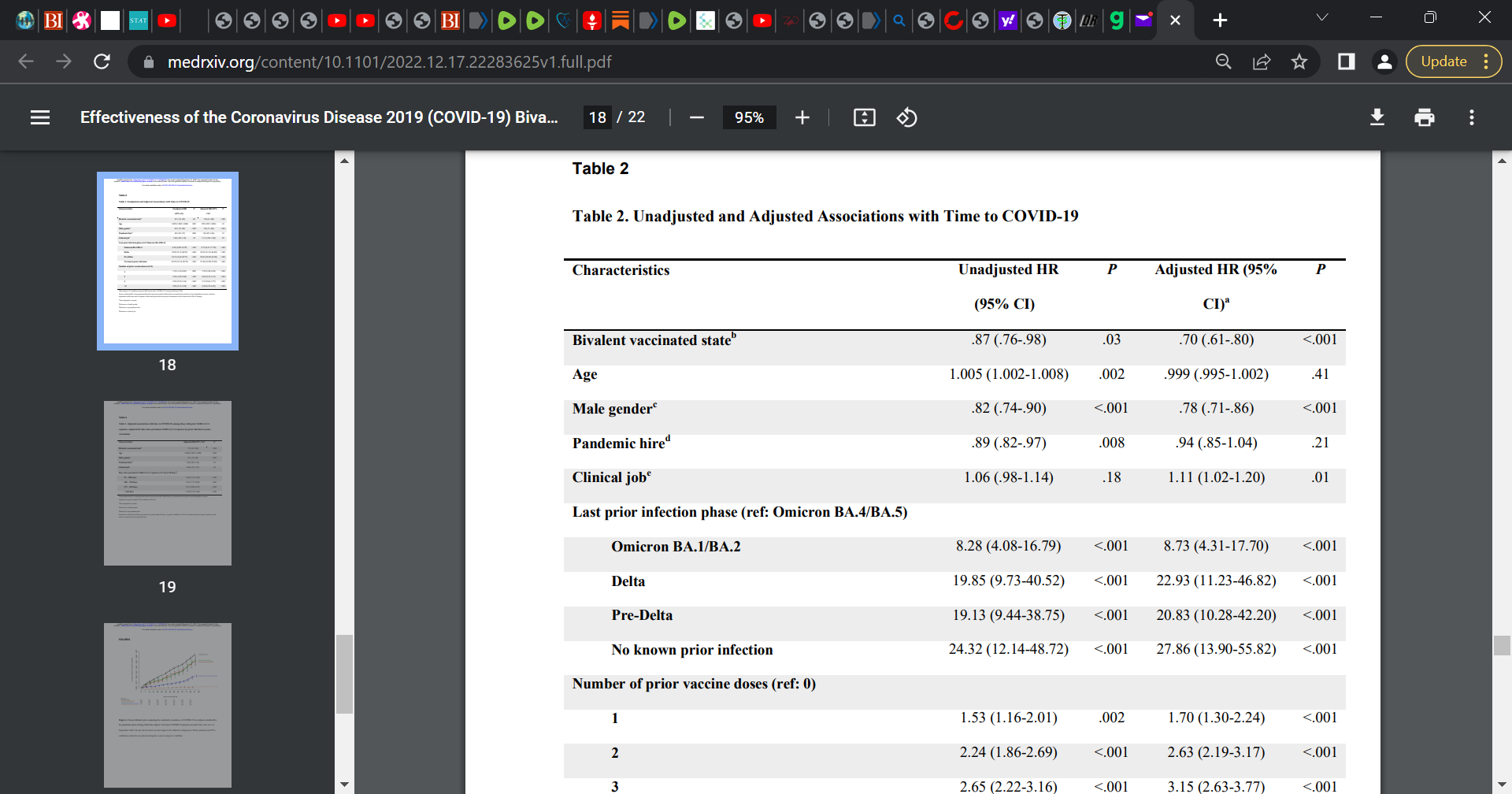
Overall, a key message is that they bivalent booster is at most 30% effective at preventing infection. This is a pure failure and does not even reach the 50% effectiveness threshold requested by WHO. The data appears to show an incremental infection risk based on the number of doses (3 times more risk with 3 or greater doses) (Table 2). Risk of infection goes up as one gets additional doses.
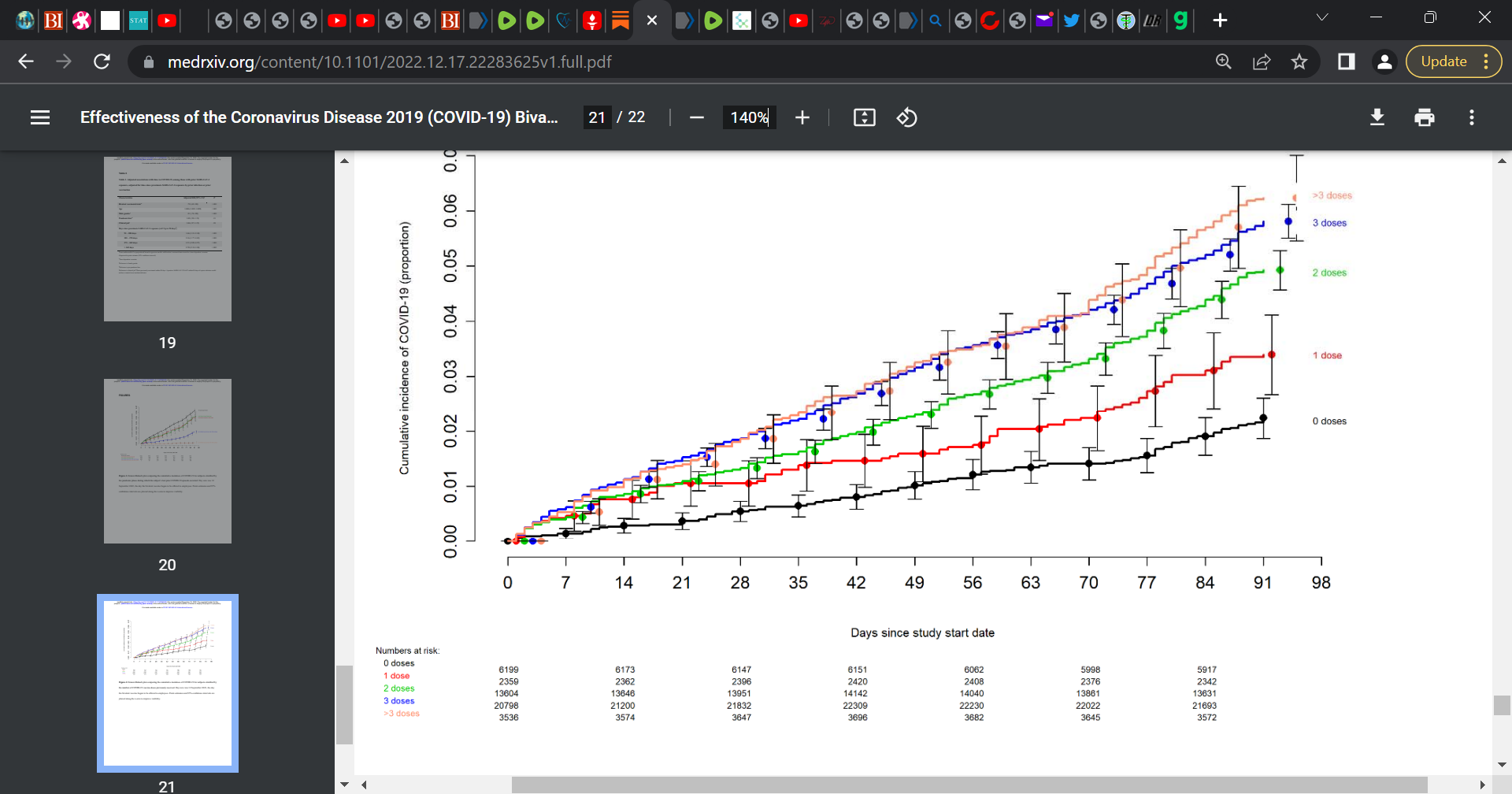
The following figure 2 is also key and it is a plot comparing the cumulative incidence of COVID-19 for subjects stratified by the number of COVID-19 vaccine doses previously received. As you see, those with no shots (0) performed best (lowest cumulative incidence of infection).
SOURCE:
https://www.medrxiv.org/content/10.1101/2022.12.17.22283625v1

More details on the study:
A retrospective cohort study conducted at the Cleveland Clinic Health System (CCHS) in the United States.
Researchers included employees on the very day that the bivalent COVID-19 vaccine was first available.
‘Protection provided by vaccination (analyzed as a time-dependent covariate) was evaluated using Cox proportional hazards regression.’
Findings focused on 51,011 employees of which 20,689 (41%) had a prior documented COVID-19 infection (episode), and whereby 42,064 (83%) received at least two doses of the vaccine.
‘The majority of infections in Ohio were caused by the BA.4 or BA.5 lineages of the Omicron variant during the first 10 weeks of the study, based on SARS-CoV-2 variant monitoring data available from the Ohio Department of Health. By December, the BQ.1, BQ.1.1, and BF.7 lineages accounted for a substantial proportion of the infections.’
‘By the end of the study, 10804 (21%) were bivalent vaccine boosted. The bivalent vaccine was the Pfizer vaccine in 9595 (89%) and the Moderna vaccine in the remaining 1178. Altogether, 2452 employees (5%) acquired COVID-19 during the 13 weeks of the study.’
‘The calculated overall vaccine effectiveness from the model was 30% (95% C.I., 20% – 39%)…when the Omicron BA.4/BA.5 lineages were the predominant circulating strains.’
‘The multivariable analyses also found that, the more recent the last prior COVID-19 episode was the lower the risk of COVID-19, and that the greater the number of vaccine doses previously received the higher the risk of COVID-19.’
Please consider ordering my book ‘Presidential Takedown’:
Order via this LINK


Dear Readers,
I also embed this short piece on The Wellness Company and The UNITY Project.
First, The Wellness Company.
I am proud to announce a unique partnership with The Wellness Company and everyone who believes in medical freedom. My dear and esteemed colleagues Dr. Peter McCullough and Dr. Harvey Risch are also in partnership with The Wellness Company which provides telemedicine services for long-haul COVID, vaccine injury, and medical exemptions along with supplements and products that are fully aligned with our values. This support for The Wellness Company stems from the sub-optimal medical care and response that we experienced throughout the pandemic. It became apparent that there are many glaring gaps in our healthcare system and people were not properly treated. Thus, the pivot by us to support The Wellness Company. Take a stand against a broken healthcare delivery system with a membership in The Wellness Company, which directly funds our fight against medical tyranny. Click here The Wellness Company for more information.
I also provide scientific support to The UNITY Project out of California. A magical organization for good. I support this tremendous initiative with some fine colleagues who have been warriors in the fight against all the wrongs in COVID. The UNITY Project aligns with my core values for it is very fierce in its fight to protect children from the danger of the largely safety untested COVID gene injection (The Unity Project Formed by Concerned Parents to Coordinate Opposition to California's K-12 COVID-19 Vaccination Mandate).
Sadly, we can’t trust anything our government recommends regarding our medical care.
No Covid or flu shots for me.
Take more shots, get more "COVID". Die soon.
A safe assumption would be they are putting the poison in everything.