

COVID mRNA vaccine on top of natural immunity is TROUBLE! ‘Prior SARS CoV-2 infection who had detectable antibodies & received 1 or > doses of vaccine had significantly higher S-specific IgG levels &
were more likely to develop severe heart failure or cardiogenic shock after STEMI...association was independent of age & even more pronounced in younger patients in a subgroup analysis.’

There was also evidence early on from Mathioudakis, from Raw, and from Krammer that raises questions on safety. I had written about this in December 2021.
See below for the full prior substack.
But read my conclusion in 2021 when there was pure insanity where everyone was taking the vaccine and it was being promoted even by Malone, Bourla, Bancel, Sahin, Hahn, Redfield, Birx, Walensky et al. All of these IMO psycho people for they were advocating a vaccine with no safety data and even in pregnant women. I even said para well if we must give it, give only ONE dose, only ONE. Yet I was clear NONE should be given.
See my conclusion in 2021…
‘In closing, these results indicate that the vaccines have a potential adverse impact on the vaccinee (from mild to more severe), especially if already COVID-recovered. A policy change whereby only one dose is given in COVID-19 recovered persons would appear to be reasonable and optimal. It could reduce adverse impacts. Overall, the findings appear to associate prior COVID-19 recovered persons who then take COVID vaccines, with elevated incidence of vaccine side effects. This is problematical and warrants urgent study by the CDC and NIH to clarify the extent of this and how serious this is to the vaccinee. It is understood that the vaccine developers e.g. Pfizer and Moderna, did not study the vaccines for the proper and optimal duration of follow-up that could have definitively addressed these emergent concerns. The issue of adverse effects in prior recovered persons who are then vaccinated should have been studied in the registrational trials and acute study and surveillance is urgently needed now. These statements by me must not be taken as my endorsement or support for these vaccines given I have been on record indicating that they were never needed in the first place, were not properly safety tested, and are under no condition needed in healthy children who bring near statistical zero risk with a potent and functional innate immune system.’
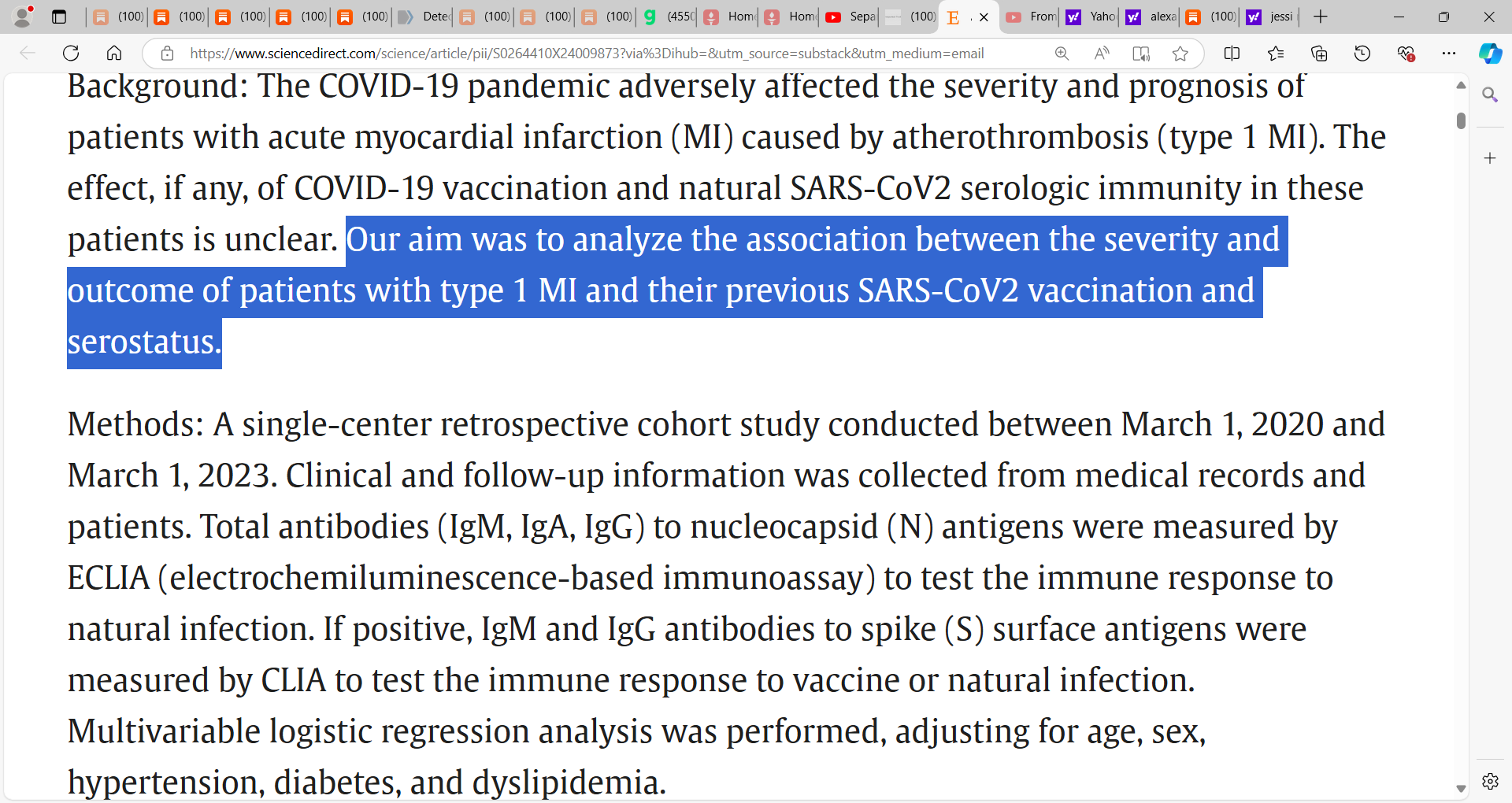
See the new Blasco study:
Blasco et al. (below ‘Association of SARS-CoV-2 immuno-serology and vaccination status with myocardial infarction severity and outcome’) confirmed a stack I wrote prior that if you layer vaccine immunity on top of natural immunity you could be in medical trouble; in other words, if you have had recovered and have natural immunity then you were never a candidate for the fraud COVID mRNA vaccines.
This study again raises serious questions as to how this COVID mRNA vaccine was developed and rolled out. I have always called for the Malone Bourla Sahin et al. mRNA gene vaccine to be stopped. Overall, the findings indicate that the COVID vaccine dramatically elevates your risk of death or heart failure (and after heart failure). And major risk in those who get the shot and have had COVID e.g. recovered (accepting that this was due to a coronavirus for I have argued it could be we will come to learn that this was a toxin or poison provoking similar respiratory symptoms).
Key finding by Blasco et al.:
‘The combination of vaccination and natural immunization against SARS-CoV2 may predispose to the development of severe heart failure and cardiogenic shock in patients with STEMI. This appears to be associated with an enhanced serologic immune response. The combination of vaccination and natural immunization against SARS-CoV2 may also adversely affect the outcome of patients with type 1 infarction in the medium term…
The main finding of the present study was the association between post-infection SARS CoV-2 seropositivity in vaccinated patients and the development of severe heart failure and cardiogenic shock after STEMI.’
But note there are some study methodological constraints and issues to consider as we read the troubling findings, so I caution you:
researchers did not fully analyze the impact of the different vaccine types
whether infection and natural immunity happened prior to or after the vaccinations was not clearly described. And so, the findings may be confounded by this.
impact of COVID severity was not assessed.
New study by Blasco et al.:
My prior stack on this issue:
The accumulated research evidence is now clear (well over 30 studies and pieces of evidence) that the COVID-19 vaccines and particularly the Pfizer vaccine, is ineffective with dramatic lost effectiveness several months after administration (see Brownstone op-ed). There is also clear indication that the vaccinated person can become infected post vaccination, can harbor very high loads of virus, and can even transmit. You may wish to refer to Chau et al., Riemersma et al., Shitrit et al., Singanayagam et al., and Salvatore et al. Deaths post vaccine has also raised serious concern.
Pfizer’s CEO Bourla responded by calling for a 3rd booster and even 4th booster but I argue it is far more serious than this when we are seeing pathophysiological alterations and ramifications from the vaccines. It appears that the COVID-recovered person who has acquired natural exposure immunity is at risk for adverse effects if then vaccinated. Layering vaccine immunity on top of natural immunity seems to be a problem and we argue must be considered and explained as a potential risk to the intended vaccinee. At the very least the person should be allowed to exercise their natural immunity given strong Israeli evidence that vaccine immunity is inferior to natural immunity and even vaccine on top of natural immunity confers no additional significant benefit.
What do we know about the impact of the COVID vaccines on the vaccinee’s physiological responses and if these are problematic or pathological? Well, Liu et al. reported immunological alterations in people following COVID-19 vaccination. Results indicated that vaccination, in addition to stimulating the generation of neutralizing antibodies, “also influenced various health indicators including those related to diabetes, renal dysfunction, cholesterol metabolism, coagulation problems, electrolyte imbalance, in a way as if the volunteers experienced an infection.” In other words, the changes seen in vaccinated persons indicated that the vaccine’s effects mirrored the infection’s effects. Researchers reported that “reduction of CD8+ T cells and increase in classic monocyte contents were exemplary” and that “it is imperative to consider the potential long-term impact of vaccination to certain medical conditions or to general human health.”
Baos et al. also reported on the negative effect of the second dose of the Pfizer BNT162b2 vaccine in a significant percentage of individuals with previous COVID infection. “Humoral immune responses were evaluated in 197 individuals, 98 with a previous COVID-19 infection (PI) and 99 who were infection-naïve (NI).” Researchers reported that “this is the first time that an adverse effect of the second dose is described.” They also discussed the importance of determining the serological response just before the second vaccine dose. In some of these subjects (especially COVID-recovered), it would “probably not be necessary (it may even be adverse) to administer the second dose of the vaccine.”
A recent publication by Ndeupen et al. reported on (via the animal/mouse model) the mRNA-LNP platform's lipid nanoparticle component that is used in vaccine studies and are in the existing vaccines under EUA. The LNPs are the fatty lipid balls that encase the mRNA (the payload) that is injected as part of the COVID-19 vaccines. They found that Acuitas' LNPs used in preclinical nucleoside-modified mRNA vaccine studies are “highly inflammatory in mice. Intradermal and intramuscular injection of these LNPs led to rapid and robust inflammatory responses, characterized by massive neutrophil infiltration, activation of diverse inflammatory pathways, and production of various inflammatory cytokines and chemokines. The same dose of LNP delivered intranasally led to similar inflammatory responses in the lung and resulted in a high mortality rate, with mechanism unresolved.”
There is also evidence from Mathioudakis, from Raw, and from Krammer that raises questions on safety.
Mathioudakis et al. looked at the safety, tolerability and reactogenicity of available COVID-19 vaccines in different recipient groups. The reported on 2,002 respondents, of whom 26.6% had prior COVID-19 infection (68.8% laboratory confirmed). “Prior COVID-19 infection was associated with increased risk of any side effect (risk ratio 1.08, 95% confidence intervals [1.05-1.11]), fever (2.24 [1.86-2.70]), breathlessness (2.05 [1.28-3.29]), flu-like illness (1.78 [1.51-2.10]), fatigue (1.34 [1.20-1.49]) and local reactions (1.10 [1.06-1.15]). It was also associated with increased risk of severe side effects, leading to hospital care (1.56 [1.14-2.12]).”
Krammer et al. examined spike antibody responses and increased reactogenicity in seropositive individuals after a single dose of SARS-CoV-2 mRNA vaccine. They reported that the antibody response to the first vaccine dose in individuals with pre-existing immunity “is equal to or even exceeds the titers found in naïve individuals after the second dose…they also show that the reactogenicity is significantly higher in individuals who have been infected with SARS-CoV-2 in the past.”
Raw et al. studied whether individuals with prior history of COVID-19 were more likely to experience AEs after BNT162b2/Pfizer vaccination, than those without previous COVID-19, and whether COVID-19-vaccination interval influenced AE severity. Researchers reported that of 974 respondents (81% female, mean age 48), “265 (27%) reported previous COVID-19 infection. Within this group (symptoms median 8.9 months pre-vaccination), 30 (11%) complained of Long-COVID. The proportion reporting one moderate/severe symptom was higher in the previous COVID-19 group (56% v 47%, OR=1.5 [95%CI, 1.1–2.0], p=.009), with fever, fatigue, myalgia-arthralgia and lymphadenopathy significantly more common.”
In closing, these results indicate that the vaccines have a potential adverse impact on the vaccinee (from mild to more severe), especially if already COVID-recovered. A policy change whereby only one dose is given in COVID-19 recovered persons would appear to be reasonable and optimal. It could reduce adverse impacts. Overall, the findings appear to associate prior COVID-19 recovered persons who then take COVID vaccines, with elevated incidence of vaccine side effects. This is problematical and warrants urgent study by the CDC and NIH to clarify the extent of this and how serious this is to the vaccinee.
It is understood that the vaccine developers e.g. Pfizer and Moderna, did not study the vaccines for the proper and optimal duration of follow-up that could have definitively addressed these emergent concerns. The issue of adverse effects in prior recovered persons who are then vaccinated should have been studied in the registrational trials and acute study and surveillance is urgently needed now. These statements by me must not be taken as my endorsement or support for these vaccines given I have been on record indicating that they were never needed in the first place, were not properly safety tested, and are under no condition needed in healthy children who bring near statistical zero risk with a potent and functional innate immune system.
___
You must not wait for another catastrophic crisis (at times manufactured but we are prevented from making our own basic personal decisions or accessing needed drugs and response tools) to catch you off-guard. We must take charge and be prepared today so that we can enjoy peace of mind tomorrow.
Enter the Wellness Company as a solution and a willing participant in the health care conversation. From telemedicine, prescriptions, memberships, and supplements, TWC is leading America with alternative choices to the traditional health care model.
Firstly, please consider going from an UNPAID subscriber or follower to a PAID at $5 per month or $30 per year. This can provide me help. If this is not possible at this time, this is ok, please remain a subscriber for FREE and there is no difference between FREE and PAID. No restrictions.
Alternatively, if you wish to give a donation to help, you can at:
Zelle:
sr7283@gmail.com
Or Ko-Fi
Ko-fi.com/drpauleliasalexander
Or to my address at:
150 South 8th Street
Unit 170
Lewiston, New York
14092
Please consider support of a good company Drs. McCullough, Risch, Thorp, myself support (they are our sponsors), The Wellness Company; see the emergency preparation kit (with antibiotics you were denied by doctors, pharmacists, governments during the fraud COVID), first aid kit, travel emergency kit, contagion control kit etc. Please consider the SPIKE SUPPORT (spike protein DETOX dissolving) formula with NATTOKINASE as well as the triple formula (SPIKE SUPPORT, BROMELAIN, CIRCUMIN)
if you continue these Malone Bancel Sahin et al. mRNA shots you could die, no more boosters, most of the world was exposed to whatever this was...have natural immunity...these deadly vaccines on top of natural immunity can harm you (also vaccine then exposure which is the unlikely sequence now)
I really enjoy receiving information that confirms my first understanding that allowing a doctor to inject me with Covid 19 death juice would have killed me. An internist recently tried to convince me that I was in great need of vaccination...I refused, and he removed me from his patient list...good. Improves my longevity substantially. Thanks Doc. I intend to resist being forced to get vaccinated...at all cost. Amen.