CRISPR/Cas9 (clustered interspaced short palindromic repeats; DNA editing, point mutation-gene insertion), mRNA technology vaccines (Malone Bourla Weissman et al.), siRNA (small interfering RNA), RNA
helicase enzymes, ribonuclease targeting chimeras (RIBOTACs)...these entities, especially CRISPR, siRNA, mRNA technology vaccines (encapsulated lipid-nano particle/LNP platform); get to know them


Re-post given the significance!
Get familiar with these mRNA technology vaccine related technical terms for they will rule humanity long-term whether you like it or wanted it!
They are bringing a fake fraud avian bird flu, PCR manufactured, just like COVID. Be warned!
It is no longer is it efficacious or effective (proven in ideal and real-world settings), is it safe (proven safe where harms have been excluded via the proper duration of follow-up studies/RCTs etc.) and is it NEEDED (is it something society demands or wants or can use or has value-added)…no no no, these demons in pharma etc. do not care if you need it. They are giving it to you.
There is a line between good and evil, and we are at the line and crossed over into ‘evil’. These mRNA MADMEN and MADWOMEN! They must be called out, dragged into courts with judges and juries, examined under oath and if shown caused harms and deaths, as declared by judges and juries, then they must be jailed or executed.
mRNA gene-based technology vaccines were imposed on society, mandated, as part of OWS (the ‘crown jewel of OWS) with no safety testing, nothing, despite out of the box showing the vaccine did not stop infection or transmission (thus non-sterilizing) and thus was moot, dead, without care for the long-term implications and you could not stop them during COVID. The ‘powers at be’ decided what they were going to do in order to gain power, control, money.
If a vaccine does not stop transmission, it cannot be mandated as confers no societal benefit. Period! Yet that did not stop the evil beasts we confronted at CDC and FDA and HHS and NIH etc. Did not stop our corrupt inept, academically lazy, intellectually sloppy, specious, non-sensical medical doctors, our scientists…no no no…they were power-drunk and money-craven.
And we are off the cliff now with this mRNA technology and it is bumping into AI (artificial intelligence) and the dangers AI poses. The makers of AI, their intended uses. As soon as humanity discovered atomic/nuclear fission, what did we do? We invented the atomic bomb to kill people. And we did. Human beings take technology and advancements and somehow figure out how to harm with it FIRST and the problem with mRNA technology is that it gets at the very core of humanity and civilization, this being the human genome, DNA. And interferes with it. And we have no understanding of the long-term implications.
Yet we know one thing thus far:
The OWS mRNA vaccines (and DNA viral vector platforms that were also made) did not work, never worked, and caused tremendous harms and death. Still are!
I am going to study this further (while I have a decent enough understanding) and I wish to read Hulscher’s paper on siRNA (small interfering RNAs) and RIBOTACs as well as Sasha Latypova’s rebuttal that raises serious and key questions. Latypova’s questions are really simple, and they are mine which is, all of the implications of present mRNA technology and vaccine, all of the drawbacks and harms, apply to siRNA technology etc. Also not studied on populations, not studied for harms, not studied for long-term implications on DNA and the human genome.
In short, based on the molecular tools (all surrounding manipulation in some manner of human DNA/genetic material) I describe below, and their evil intentions (the ‘makes), our daily lives will be changed forever with this mRNA (RNA) technology. This is their intention, BIG business, BIG pharma, BIG evil, BIG cabal, BIG globalists, which is to make perpetual money, never ending, and at our expense. They do not care about your well-being. This is about MONEY. These beelzebub beasts have no care for our safety and survival. Just their fame, money, power, control. Worse.
If we do not get on top of this now, if we do not understand this and have the urgent necessary discussions societally, then this Malone Bancel et al. mRNA technology and gene-based vaccine and platform, it’s unison with CRISPR, siRNA etc., then we will be in serious harm trouble, from a HUMANITY point of view.
Yet it is happening ‘while you sleep’. The ‘powers at be’ are rolling this out and mainstreaming it, and we seem powerless. But if we do not stop this now, our lives will be changed negatively forever for there have never been the proper clinical studies and particularly study that could ‘exclude’ harms. No study has been or is slated to demonstrate safety in this era of mRNA technology. Moreover, as of now, the evidence clearly shows this technology is problematic and dangerous.
The Operation Warp Speed (OWS) mRNA COVID vaccines were NOT needed, did not work, and showed a dangerous prior safety history in all attempts to study it or apply it, and have been a catastrophic failure yet the merchants of death, the modern day Mengeles, Klaus Barbies, Hesses etc. with their mRNA technology, will not stop.
What do we do? Well, we have to stop them! So, who will be the mRNA technology Pretorians? The Vanguards to safeguard humanity?
What Robert Malone, Moncef Slaoui, Albert Bourla, Bancel, Ugur Sahin, Katalin Karikó, Drew Weissman, General Perna, Ozlem Tureci et al., these people, have done to the world with a safety untested mRNA technology and the Pfizer, Moderna, BioNTech vaccine is monstrous. Monstrous.
I continue to call for a complete ban, not a study of, not a review, but a 100% ban on all RNA products, any mRNA product, LNP product, or any such OWS ‘countermeasure’ product as part of any human vaccines e.g. the current mRNA COVID related vaccines must be stopped in full. All the evidence to date shows these mRNA gene-based technology vaccines to be ineffective (negative effectiveness, non-sterilizing/non-neutralizing) and harmful, deadly. Must be stopped in toto. And if I can get it back into the genie box, then forever! It has no place.
mRNA vaccines under OWS were not needed, never needed and did not work! Anyone who said they worked and that they saved lives…lied to you! Deceived you!
Complete and now! There is no evidence anywhere in the entire world showing the synthetic mRNA (on its own) technology or as part of the LNP (delivery platform) is safe or effective. It must be stopped! It has shown itself to be just too harmful. There is no, not ONE, none, ZERO, randomized clinical trials, no proper comparative effectiveness research studies that have shown that any of the OWS mRNA technology gene-based vaccines (in adults or children) worked to reduce hospitalizations, ICU, severe harms, or deaths. Not one! As of today! And all of this work remains on emergency use (EUA) because FDA knows if they put these through their proper regulatory assessment framework, their BLA process, that they will fail. So, these MUST remain on EUA. Imagine that!
We have been set up as a society, as people by evil people.
I might be willing to consider that these entities (listed above) will all need to be taken back to the lab for at least 100 more years of bench research using all types of animal models etc. (harms completely excluded) and with the proper ethical debate before ever brought back in front of the population to consider in a vaccine and always in 100 years, based on proper benefit versus risk informed consenting. A vaccine maker making something does not mean the population has to accept it. Or will accept it. 100 years before we look at this again and a core aspect is it must be shown that it does not and cannot interface or re-integrate or interfere in any manner, with the underlying human DNA. Conclusively shown. Exhaustive definitive evidence of safety with harms excluded, remains a basic ingredient for us to even look at this in 100 years and no sooner. For us to discuss, not for us to implement. The population must be core to any debate as to IF they want it. A religious component is key also.
I have tabled the key molecular entities here within this new deadly arena of mRNA technology platform vaccines (created by Malone Bourla Bancel Sahin Weissman Katalin Karikó et al. and disastrously used in the fake fraud PCR-created COVID non-pandemic yet positioning to become part of your daily life replacing all therapeutics) that include the CRISPR/Cas9 gene editing platform and siRNA. We are entering into a very dangerous arena now, that will transform our lives. We argue catastrophically. Many involved seek to make money, PERIOD. mRNA technology researchers, vaccine makers like Pfizer, Moderna etc. They do not care about the ethics of this, or the safety of this. Just money! Thus far mRNA vaccines have proven ineffective and deadly.
These molecular entities and tools e.g. CRISPR/Cas9 (clustered interspaced short palindromic repeats; DNA editing, point mutation-gene insertion), mRNA technology vaccines (Malone Bourla Weissman et al.), siRNA (small interfering RNA), RNA helicase enzymes, ribonuclease targeting chimeras (RIBOTACs) are changing and about to radically transform our lives. In terrible ways given the harms we know so far. Moreover, the type of ethics debates needed are not happening.
Not because pharma can create something means we the population wants it or desires it.
So these molecular tools and entities I have names above now must be studied, discussed and Hulscher et al. and Sasha Latypova now centers the debate.
I thank them.
My first blush tells me that it is outrageous to consider a mRNA vaccine (siRNA etc.) to fix or detoxify or suppress or de-activate the existing mRNA technology vaccine (created by Malone Bourla Bancel Sahin Weissman Katalin Karikó et al.). We need proper oversight of all of this insanity.
"Pre-medication", or how to sell $50 worth of generic drugs for $600,000!
The curious case of Onpattro, siRNA in lipid nanoparticle now being considered by some as a potential treatment for mRNA injuries
Jun 17
‘I had a friend in school, who needed a “pre-dinner” before dinner, and then a pizza slice after the dinner. He was skinny. I still hate him.
This is not a hit piece. This is a “pre-crime” novel.
Due Diligence and Art is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber.
A couple of weeks ago, many of us were rather shocked by the following publication:

Courageous Discourse™ with Dr. Peter McCullough & John Leake
By Peter A. McCullough, MD, MPH As the world is waking up to nearly two thirds with potential future disease and disability from the long-lasting mRNA coding for the dangerous Wuhan Spike protein, the search is on for ways to stop this molecular monster from doing more damage…
In their review paper, Huschler, McCullough and Marotta proposed that treatment of mRNA induced vaccine injury may be mitigated with small interfering RNA (siRNA) and ribonuclease targeting chimeras (RIBOTACs). Quoting from the Substack post by Dr. McCullough:
It may seem unfathomable for doctors to inject more RNA to deactivate Pfizer and Moderna synthetic mRNA that has accumulated in the body after multiple injections. However, siRNA used today in my practice (patisiran, inclisiran) appears to be safe and well-tolerated only notable for injection site reactions.
I am one of the people for whom this idea is unfathomable, and I would like to provide some reasons as to why. I am not accusing anyone of anything. I believe that there is important information missing from this review, which I am going to discuss here.
While proposing siRNA as a treatment for mRNA injury, the paper does not discuss the current on-market siRNA drugs (patisiran - Onpattro, and inclisiran- Leqvio) in detail.
To address Leqvio briefly: it is administered by subcutaneous injection that targets the liver, has many severe counterindications, is known to cause fetal damage, has warnings for cardiovascular adverse events (while being indicated to presumably improve cardiac condition!), and it has never been shown to improve any real health outcomes. As many “new-new-science” drugs on the market, it treats test results, flowcharts, “standards of care” and income statements, not real humans. It is designed to “modify lipids”, i.e. make your cholesterol test look better in the eyes of the establishment/government medicine. The label states that “the effect of inclisiran on cardiovascular morbidity and mortality has not yet been determined”.
This article will focus on Onpattro, as it is similar to the covid shots, being a synthetic RNA (albeit a much smaller strand vs mRNA), encapsulated in LNP containing polyethylene glycol (PEG) - a known extremely toxic substance, which may account for a large % of known covid jab toxicities.
Onpattro (patisiran) is an injectable small interfering RNA that may be used to treat polyneuropathy (multiple nerve damage) caused by hereditary transthyretin-mediated amyloidosis (ATTR) in adults. ATTR occurs when liver produces faulty transthyretin (TTR) proteins and TTR deposits accumulate in organs and tissues, most commonly the peripheral nerves. While I have not delved into ATTR, when exactly it was discovered and what evidence makes it hereditary, I strongly suspect that it is yet another BS new “rare genetic disease” made up as a cover for vaccine and/or environmental toxicity.
The mechanism of action for Onpattro is described as breaking down mutant and wild-type transthyretin (TTR) proteins through RNA interference. TTR is a protein primarily produced by the liver, that carries the thyroid hormone thyroxine and retinol (vitamin A) throughout the body.
Onpattro was FDA-approved on August 10, 2018.
Reviewing the FDA-approved label, I was immediately struck by the following (p.1, Dosage and Administration):
Premedicate with a corticosteroid, acetaminophen, and antihistamines
All patients should receive premedication prior to ONPATTRO administration to reduce the risk of infusion-related reactions (IRRs) [see Warnings and Precautions (5.1)]. Each of the following premedications should be given on the day of ONPATTRO infusion at least 60 minutes prior to the start of infusion:
• Intravenous corticosteroid (e.g., dexamethasone 10 mg, or equivalent)
• Oral acetaminophen (500 mg)
• Intravenous H1 blocker (e.g., diphenhydramine 50 mg, or equivalent)
• Intravenous H2 blocker (e.g., ranitidine 50 mg, or equivalent)
Pre-medication here is a requirement and involves 4 generic drugs, including a steroid, a known big “fire extinguisher” for any inflammatory symptoms. It is not something that should be used long term. Yet, here we have prescribed chronic use of it, for life. Long-term side effects of steroids include:
Long-term side effects:
Osteoporosis (bone loss)
Aseptic necrosis (death of bone tissue)
Adrenal insufficiency (reduced adrenal gland function)
Cataracts
Glaucoma
Increased risk of infections
Mood disorders (depression, anxiety, psychosis)
Reduced libido
Weight gain and obesity
Skin thinning and easy bruising
Hair loss
Increased risk of diabetes
High blood pressure
Cardiovascular disease
Other risks:
Withdrawal symptoms when stopping steroid use, such as fatigue, muscle weakness, and joint pain
Increased risk of developing osteoporosis and fractures
Reduced immune system function
Increased risk of infections, including pneumonia and tuberculosis
Increased risk of gastrointestinal problems, such as stomach ulcers and bleeding
Was Onpattro, the first-ever synthetic RNA product approved for market, ever studied alone, without the use of 4 “pre-medications”?
Turns out, no!
I found the published Phase 3 study for Onpattro, based on which it received the FDA approval. In my opinion, the study has a lot of highly questionable design features. I am not a clinical trial statistician, so I can’t provide a re-analysis and I am not sure it is possible from the information given in the paper. I am just going to list what I find very concerning:
The study was small (~225 patients enrolled, 193 completed the study), and the number of clinical sites is very large 44 in 19 countries. This means, on average, 1 clinical trial site handled ~4-5 patients in the period of ~3+ years it took to complete the study. A small study divided among a large number of international sites is a recipe for large variability in a small dataset, and also an easy scenario for data manipulation. This is also a market-capture strategy. Pay lavish fees to every “key” doctor in a particular disease area to participate in the clinical trial where they might have to see a couple of patients a year and they become your devoted sales team. They get to be co-authors of the prestigious NEJM paper discussing “first”, “breakthrough”, “innovative” tech that Elon Musk says will cure cancer one day! Who cares about little things like data variability, we are saving the world here!
While using 5 (!!!) drugs in the study regimen (4 “pre-medications” + Onpattro), none of them are studied alone. Onpattro is never studied alone. The 4 pre-meds are not studied alone in this patient population either! We have no idea what each drug does by itself in this patient population. There are only 2 arms in the study - “pre-meds”+ saline IV and “pre-meds”+Onpattro. This is not a valid clinical trial design for a new medicine, and remember that this was the first and only “real” approval of RNA+LNP therapeutic. So, we are not just talking new medicine, but an entire new medicine class.
siRNA (just as mRNA products) is a pro-drug! It makes your liver act in certain way and produce the medicinal effect (allegedly). Again, combining a pro-drug with 4 drugs - who knows what interactions are happening? Nobody does…
The patients in the treatment arm were allowed to leave the study if the treatment didn’t work for them. Reasonable for severely ill people. However, this of course creates a bias for the study results, similar to what happens to your GPA if you are allowed to drop a course that you know you are going to fail. It is not explained in the paper whether this bias was properly handled in the statistics.
The study was not entirely blinded. Due to infusion-reactions, which were far more numerous, and characteristic in the active group of the study, it is likely that the investigators became unblinded after the first visit where a patient experienced a particular reaction. There was no mention of how this potential bias was handled.
The rate of adverse events was a staggering 97% in both placebo and active groups, but there was a much higher rate of severe and serious adverse events in the placebo group (4 generics + IV saline) vs the treatment group. The frequency of severe adverse events (28% in the patisiran group and 36% in the placebo group) and serious adverse events (36% and 40%, respectively). Adverse events leading to discontinuation of the trial regimen occurred more frequently with placebo (14%) than with patisiran (5%). Death occurred in seven patients (5%) in the patisiran group and in six patients (8%) in the placebo group. All seven deaths in Onpattro group were cardiac arrests or failure. All deemed “unrelated”! This is absolutely staggering - 7 deaths in 18 months in 140 people who all received “new, innovative, breakthrough, we-are-going-to-Mars” medicine. Same cause of death.
At best, I would consider this study inconclusive. The study proclaims Onpattro is efficacious and similarly “safe” as the placebo regimen. However, from presented data, a conclusion can be made that the 4 generic drugs in the “placebo” regimen are dangerous for this patient population. In addition, a conclusion can also be made that apparent “efficacy” of Onpattro is simply due to the study design that favored those in whom the 4 generics produced an improvement (steroids will make some people feel much better) to complete the Onpattro group of the study. In other words, the $50 regimen can be now marketed for $600K!
Another reason that I think siRNA is not a great idea to treat the mRNA injury: the covid jabs already contain (in addition to the toxic PEG) synthetic siRNA and miRNA in unpredictable quantities! Therefore, it is possible that covid vaccine injuries at least in some people are DUE TO these substances, and thus proposing the same as treatment is like pouring gasoline on a fire.
I have reported on this eons ago. At the time of issuing the EUA for these shots, the manufacturers could not demonstrate that they were able to make mRNA-LNP product even close to the specification. The RNA is supposed to be certain length of molecule to “instruct” your cells to make the specific antigen, remember? It’s supposed to be the mRNA for the “Wuhan variant”, or for “Omicron”, or for “RSV”, and those are quite different mRNAs! However, an ability to make such precise molecule reliably has never been demonstrated, by anyone. The regulators simply changed the prior standard of acceptance of RNA conformity to 50% of the batch being approximately the weight that the specified molecule should have, and the rest could be shards and pieces of RNA, including siRNAs and miRNAs. All of this was of course based solely on manufacturer self-certification, no independent analysis of batches was done by regulators.
However, we have a lot of data from independent vial tests since then. One such analysis was done by Vanessa Schmidt-Kruger in Germany in 2022, and here are her results for RNA composition by weight (length) in a Pfizer vial.
The first line is what was supposed to be found for RNA sequence in a Pfizer vial which is claimed to induce the cells to make a very specific protein against the “Wuhan” variant of SarsCov2 (should be 4300 nucleotides in length). The rest of the lines is what was actually found.
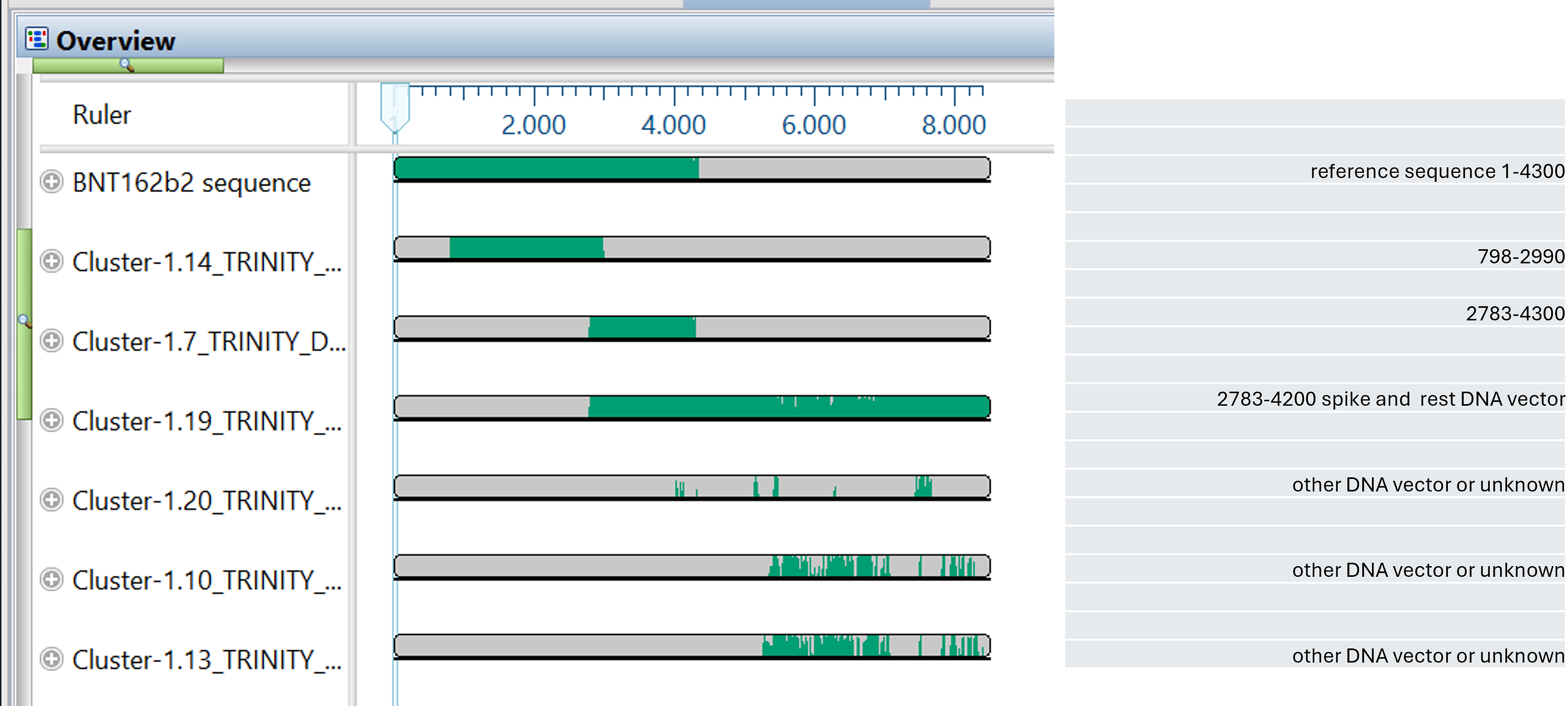
detail:
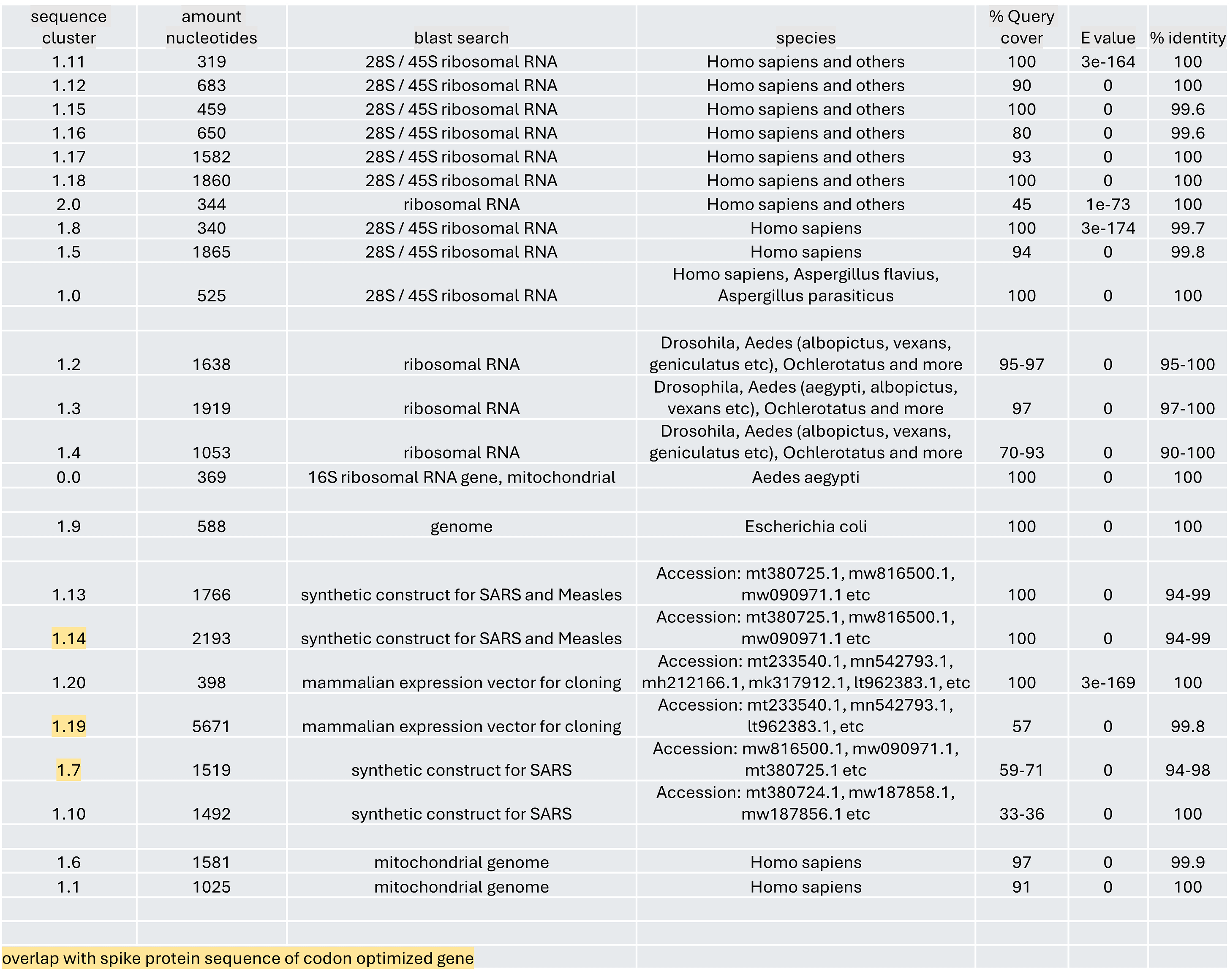
None of the findings correspond to what is supposed to be there for mRNA molecule composition. There are some strands that would pass the weight (length) test set by the FDA’s fake-acceptance criteria, but none have the composition that is claimed to produce some specific protein! There are many shorter clusters of RNA which would further degrade into shorter components such as siRNA or miRNA. It is important to emphasize, all these designations are models. There isn’t even a consensus on what the model of miRNA should be.
Side note: if you need another confirmation that it is not possible to make weaponized pandemic-causing viruses via gain-of-function molecular engineering in a lab, this is it. You are looking at the current, technological cutting-edge, state-of-the-art precision capabilities of making RNA viruses in labs! The GOF uses the same non-functioning biomanufacturing tools to allegedly build even larger very precise RNA constructs (full genome SarsCov is ~30K base pairs), reproducibly, in quantity, without a single error! They can’t make an RNA strand of ~4000 nucleotides to specification, even when it’s stabilized and encased in LNP, yet the fear porn producers tell you they can certainly make a “live virus” with scary-sounding features like “HIV insert” and “furin cleavage site”. This is when even 1 nucleotide error/change renders a potentially lethal virus into a dud. Yet, we must believe this is a world-ending scenario and demand banning this dangerous activity everywhere, but conveniently forgetting Fort Dietrick, because they are just poor confused soldiers following orders from bad Fauci, and also forgetting that this activity is already internationally banned. I agree, let’s ban this some more…
Finally, let’s examine the financial model:
In the United States, the cost of Onpattro is around $10,313 for a supply of 5 milliliters, depending on the pharmacy. The annual cost is estimated to be around $451,430 to $677,145 per patient, depending on the patient’s weight.
Inclisiran (Leqvio), an add-on therapy to other LDL-lowering drugs (statins and monoclonal antibodies), is priced at $3250/dose. I could not find annual cost estimates.
In case you didn’t know this, Medicare is not allowed to negotiate drug prices, and all private insurers follow Medicare’s pricing lead paying whatever price is demanded by pharma companies. Additionally, insurers are NOT interested in lowering costs of healthcare in general or drugs in particular. That is because their business model is based on charging a “premium”, which is dependent on the prior years’ cost increases. The more costs increase, the higher the “premium”, and thus profit. Finally, your doctor is also not interested in treating you with cheap generic medicines or things that make no profit at all, like lifestyle and diet changes. That is because the “physician charge” component for generics is zilch, while a $600,000/year treatment will have a pretty hefty allowance in the physician’s bill for the in-office infusion. Yes, they are all in on it.’
You must not wait for another catastrophic crisis (at times manufactured but we are prevented from making our own basic personal decisions or accessing needed drugs and response tools) to catch you off-guard. We must take charge and be prepared today so that we can enjoy peace of mind tomorrow.
Enter the Wellness Company as a solution and a willing participant in the health care conversation. From telemedicine, prescriptions, memberships, and supplements, TWC is leading America with alternative choices to the traditional health care model.
Firstly, please consider going from an UNPAID subscriber or follower to a PAID at $5 per month or $30 per year. This can provide me help. If this is not possible at this time, this is ok, please remain a subscriber for FREE and there is no difference between FREE and PAID. No restrictions.
Alternatively, if you wish to give a donation to help, you can at:
Zelle:
sr7283@gmail.com
Or Ko-Fi
Ko-fi.com/drpauleliasalexander
Or to my address at:
150 South 8th Street
Unit 170
Lewiston, New York
14092
Please consider support of a good company Drs. McCullough, Risch, Thorp, myself support (they are our sponsors), The Wellness Company; see the emergency preparation kit (with antibiotics you were denied by doctors, pharmacists, governments during the fraud COVID), first aid kit, travel emergency kit, contagion control kit etc. Please consider the SPIKE SUPPORT (spike protein DETOX dissolving) formula with NATTOKINASE as well as the triple formula (SPIKE SUPPORT, BROMELAIN, CIRCUMIN)
Hi doc .. I haven’t read of all of your what must be an exhaustive article ..
Thanks .. I will h go o through all later..!
It’s crazy...
The people that think this is a good idea ???
So many of the things that I are in the medical health institutions /corporations do nothing to improve the health and well being of a population.
In fact you are describing the most devastating collection of weapons of mass destruction that I’ve ever seen!
The silent war ..!
Someone labelled the health system that if I remember correctly!
A friend in Japan has told
me they are rolling out the
“self replicating” one at the moment.
It reminds me of an article by a scientist that worked on the neutrino array in Antarctica.
He said it makes HAARP look like a toy.
The he said that the definition
used to describe it within the government and corporate system was the equivalent of calling a machine gun a bullet storage device !!!
So maybe that’s how they get these evil projects past the dumbass corrupt fools that are suppose to have everyone’s best interest in mind when the demons and sock puppets are busy attempting to destroy everything on this planet including us!
Question: are they stupid corrupt or ignorant ..
Down in Gitmo one can imagine a meme borrowed from a famous war film ..
slightly changed
“ I love the smell of rope early in the morning”!
What’s Clint Eastwood doing these days ?
Dr Alexander, all of the people pushing this "vaccine" made sure that they were exempt. They haven't died. Their families haven't died, so no, this profit driven "medication" was never needed.