
Devastating week 9 UK PHE COVID infection and death data; look at the data, look at the impact on the viral dynamics of continuous infectious pressure up against mounting sub-optimal immune pressure
Devastating week 9 UK PHE COVID infection and death data; look at the data, look at the impact on the viral dynamics of continuous infectious pressure up against mounting sub-optimal immune pressure
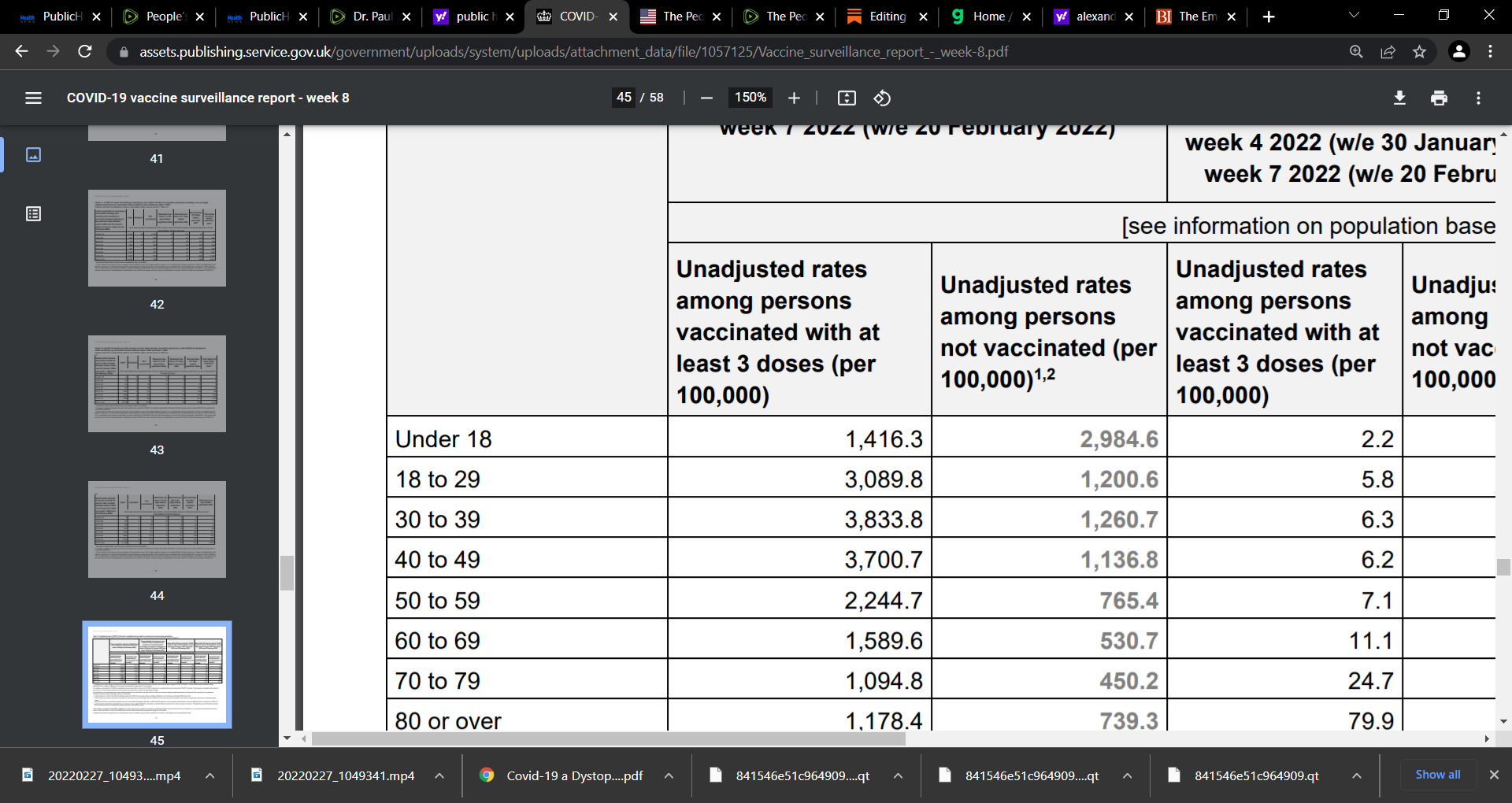
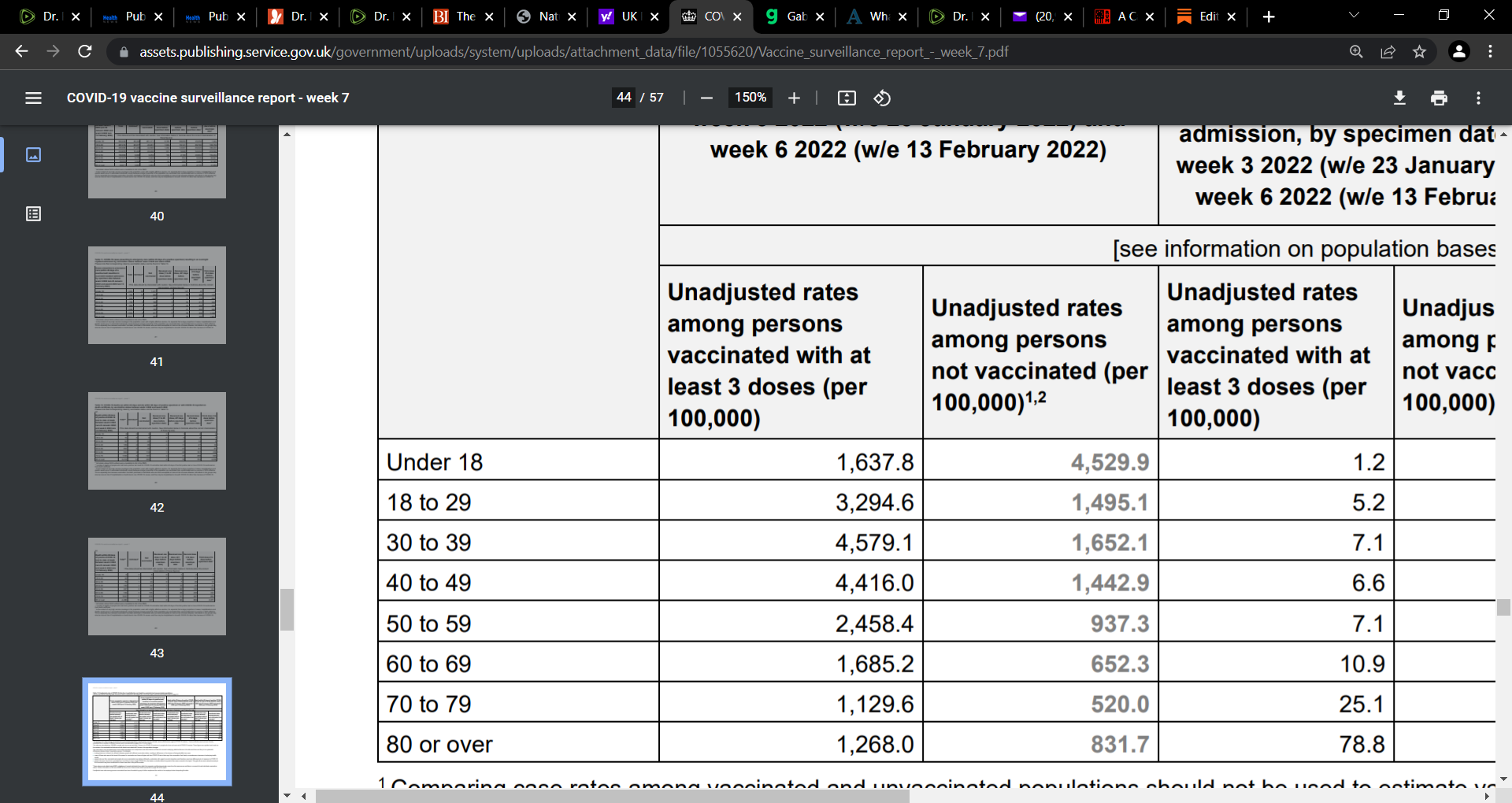
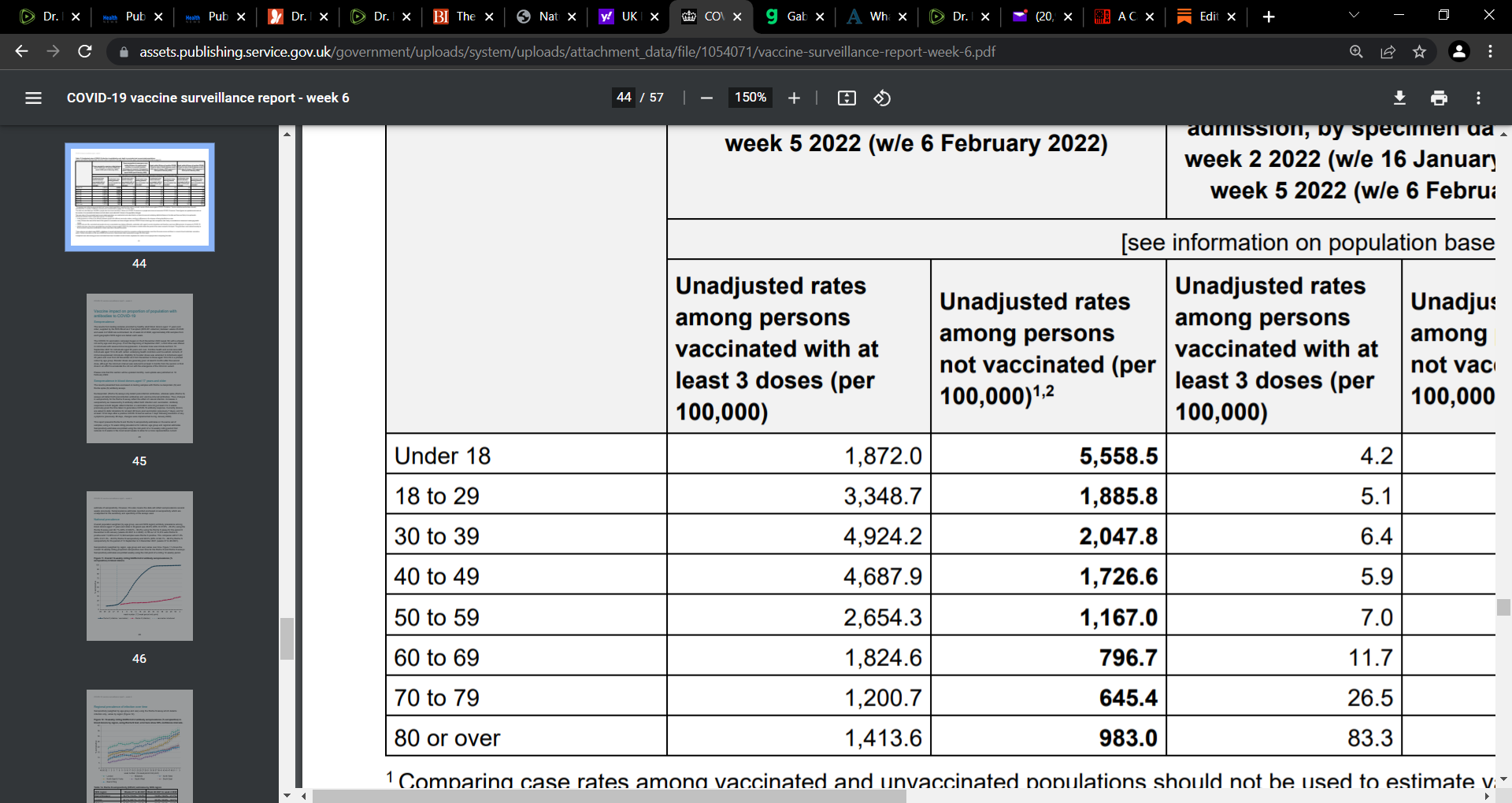
I have included weeks 5, 6, 7, and 8 to compare to the current week 9; do you see any pattern? We see for week 9 relative to week 8, across all vaccinated & unvaccinated, there is infection decline

OK, so let us try to look at the data to make some sense of it, to let it tell us a story.
Week, 9, 2022
We see that infection risk is declined across all age-groups week 8 to 9. Why? We see the same pattern for infection for the prior weeks too? Why? This goes back to what I had shared in a prior post and I confess I have developed appreciation from my study of Dr. Vanden Bossche’s thinking. I will explain it in a manner stripping away the complex aspects that I too get confused over;-) …so here goes:
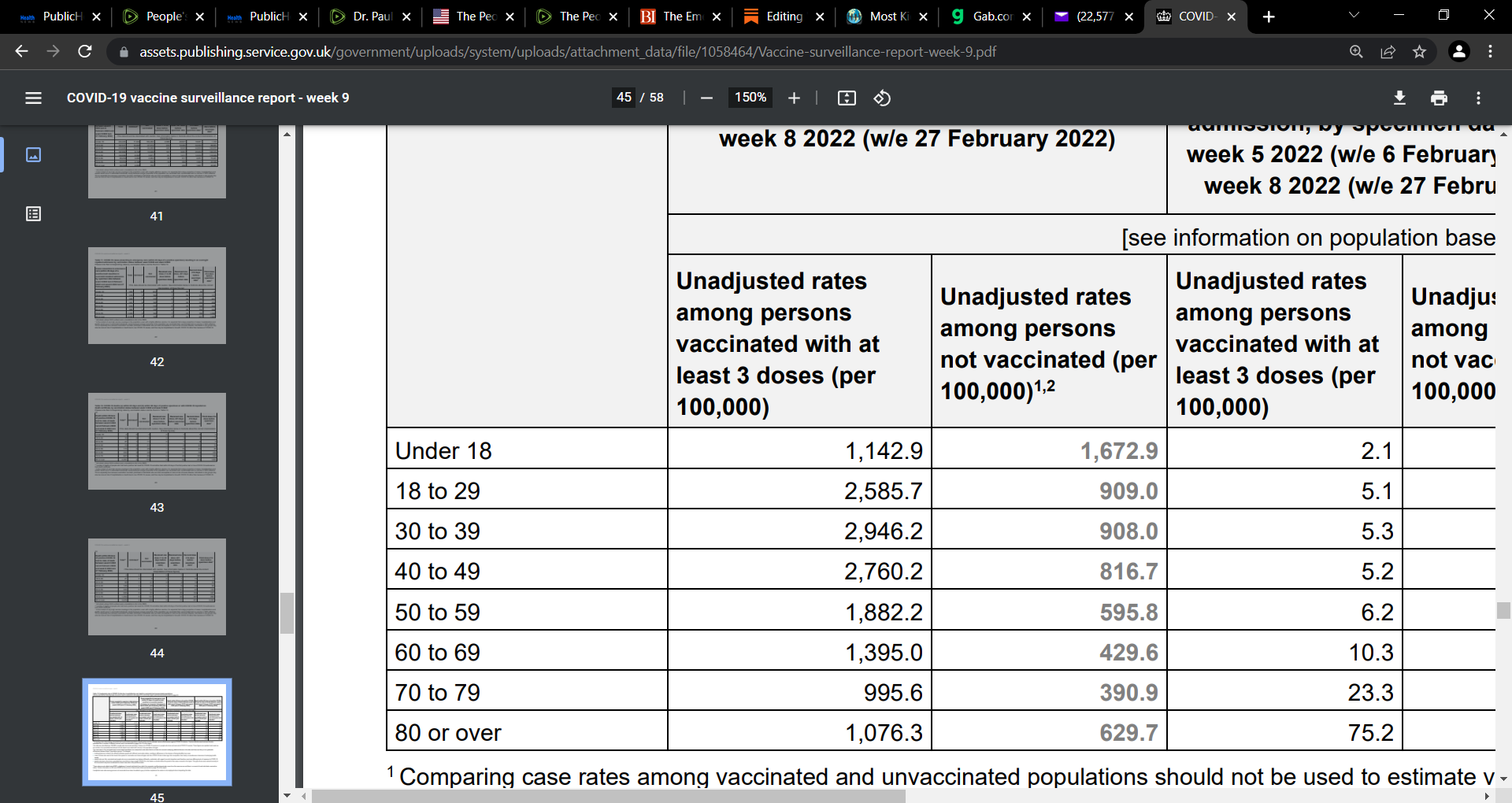
As to the vaccinated (2nd column from the left, persons in receipt of the 3rd booster in week 9, 8, 7 etc.), the theory is (and likely what is happening) that by vaccinating with the current mRNA vaccines that induces antibodies (Ab) to the original Wuhan strain, then the vaccine cannot hit the current dominant omicron (OMI) variant. There is resistance of OMI spike to the vaccinal Abs and due to this resistance, the natural innate immunity, and specifically the innate Abs, are no longer subverted and outcompeted by the vaccinal Abs. Remember, vaccinal Abs are high affinity and more specific than the low affinity and specific innate Abs (though very potent and broad); thus if the neutralizing vaccinal Abs can no longer outcompete the innate Abs, then the innate Abs are ‘set free’ and over time (across weeks, as seen here), regains its functional capacity to eliminate the virus (sterilize the virus).
We know that the vaccinal Abs cannot stop infection or transmission. As such, there is reduced infection across age-groups as time passes given the resistance to the vaccinal Abs. In other words, populations are benefitting from the resistance of the OMI variant to the vaccinal Abs by now unleashing (freeing up) the innate Abs to sterilize the virus (stopping infection etc.). The issue is if we go forward with Pfizer’s OMI specific vaccine, we will destroy this resistance and destroy this improved innate Abs functional capacity and this will cause very severe illness. Why? Because the vaccinal Abs will outcompete the innate Abs for the antigen, but remember, the vaccinal Abs cannot sterilize the virus (does not stop infection or transmission) and so while it will still bind to the virus if an OMI specific vaccine is made, it cannot sterilize (stop infection etc.). The vaccinal Abs in this case actually facilitates the entry of virus into the susceptible host cells and this can be catastrophic. This is ADE.
With regards to the 3rd column from the left (the unvaccinated), we again see the declines in infection across age groups. Why? And this decline is being seen across time, week by week. We speculate that persons who are not vaccinated and due to constant exposure, are allowing their innate immunity to be ‘trained’. Remember, it is the natural innate immunity (our first line of immune defense before the natural acquired-adaptive system kicks in if the innate is breached), that is potent and usually handles coronaviruses and influenza. This ‘training’ of innate Abs etc. puts them in a position whereby they are better able to compete with the vaccinal Abs and not be readily outcompeted for the antigen. This yields better protection from the innate Abs across time in the unvaccinated. This is what we are seeing in the data with the declines in infection in the unvaccinated.
Week 8, 2022
UK COVID-19 vaccine surveillance report Week 7 17 February 2022
Week 7
COVID-19 vaccine surveillance report Week 6 10 February 2022
Week 6:
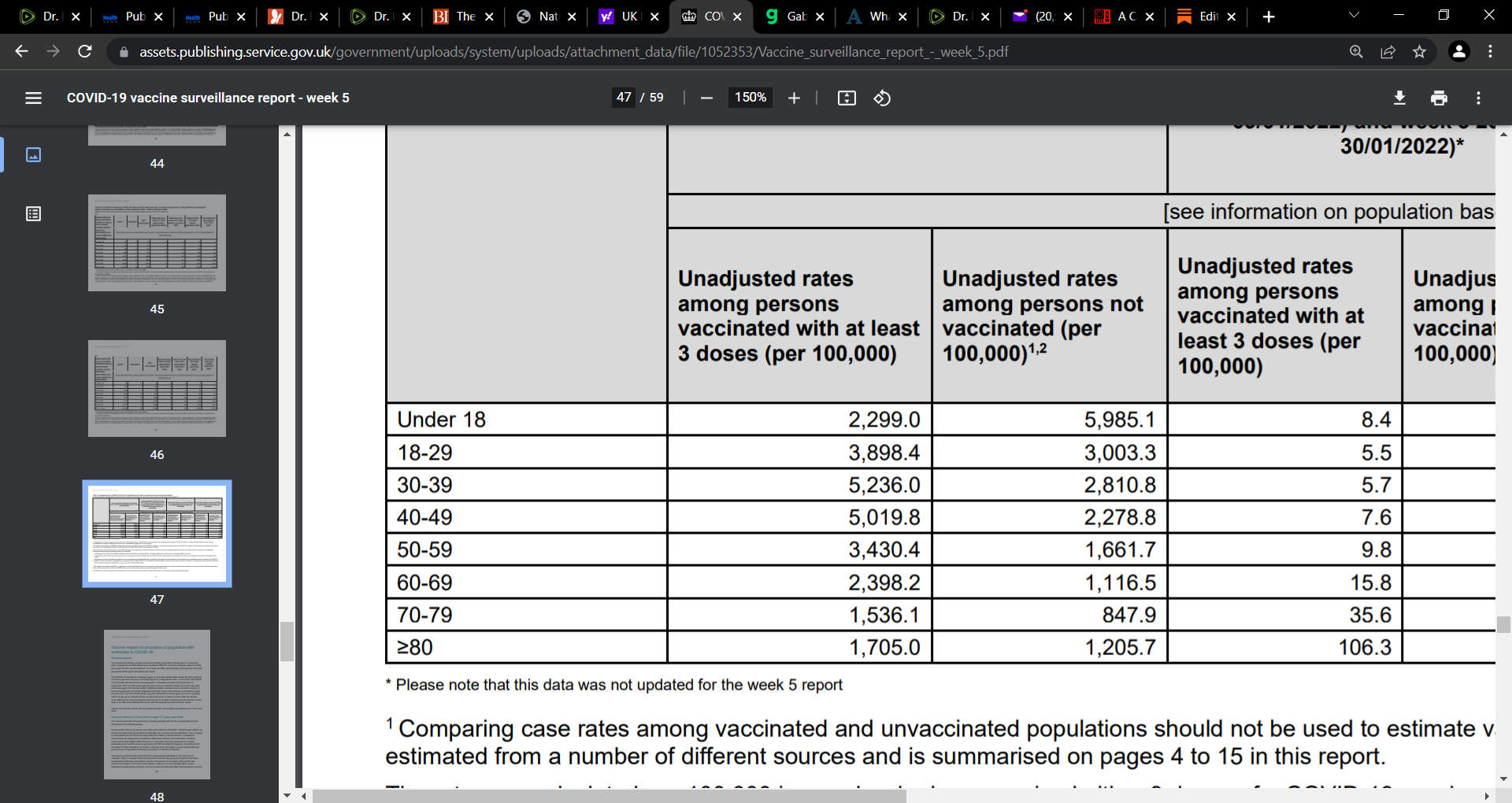
COVID-19 vaccine surveillance report Week 5 3 February 2022
Week 5
Infection:
Did you observe the pattern? It is very interesting and eye-opening. What is your view on why this is happening?
If they make an Omi specific booster, isn't it possible that the resultant vaccinal antibodies could sterilize / neutralize the virus? (Assuming they are capable of producing an effective Omi booster).
I believe Geert's major concern was that they take the current situation - in which both vaccinated and unvaccinated are training their natural immunity with Omi - and mass vaccinate for Omi (edit - with another leaky vaccine). This would place enormous mutational pressure on the virus that would likely result in a mutation whereby the virus uses a different receptor. This would result in dramatically exacerbated disease in anyone with a vaccinal antibody response - as the vaccinal antibodies will attach to an obsolete spike. By the time the natural immunity kicks in, it may be too late to avoid significant illness.
Geert appealed to the WHO to take this opportunity we now have to achieve herd immunity. As we are seeing it unfold. He was on to this months ago. And he is correct yet again.
The disaster may occur if we see mass vaccination against Omi, in which the scenario above plays out (Geert's major concern).
I think I have that right. Please feel free to correct any misapprehensions. Thanks.
Whilst you’ve been distracted by Russia’s invasion, the UK Gov. published data confirming the Fully Vaccinated are now up to 3.2x more likely to die of Covid-19 than the Unvaccinated
https://dailyexpose.uk/2022/03/04/russia-distracts-uk-gov-reveal-vaccinated-more-likely-to-die-covid/