Did a Case-Control Study in Japan's Small & Medium-Sized Enterprises by Nakatani et al. show a higher incidence of COVID infection among vaccinated persons? Yes! Indicative of dose-response, antibody-
dependent enhancement (ADE) of infection (and of disease) or original antigenic sin (OAS)/immune imprinting/immune priming/immune fixation/prejudice to the initial prime or exposure


The risk (odds) of contracting COVID-19 increased with the number of vaccine doses: one to two doses (OR: 1.63, 95% CI: 1.08-2.46, p = 0.020), three to four doses (OR: 2.04, 95% CI: 1.35-3.08, p = 0.001), and five to seven doses (OR: 2.21, 95% CI: 1.07-4.56, p = 0.033).
Methods
‘A case-control study was conducted using data collected from a survey administered by the Japan Small and Medium Enterprise Management Council in December 2023. Participants included individuals who were part of the Yamato Project, not necessarily limited to SME employees. The survey gathered information on demographic characteristics, COVID-19 infection status, vaccination history, health status before January 2020, and various preventive behaviors. The primary outcome was the presence or absence of COVID-19 infection. Data were analyzed using univariate and multivariate logistic regression models to calculate odds ratios (ORs) and 95% confidence intervals (CIs) for the association between vaccination status and COVID-19 infection.
Results
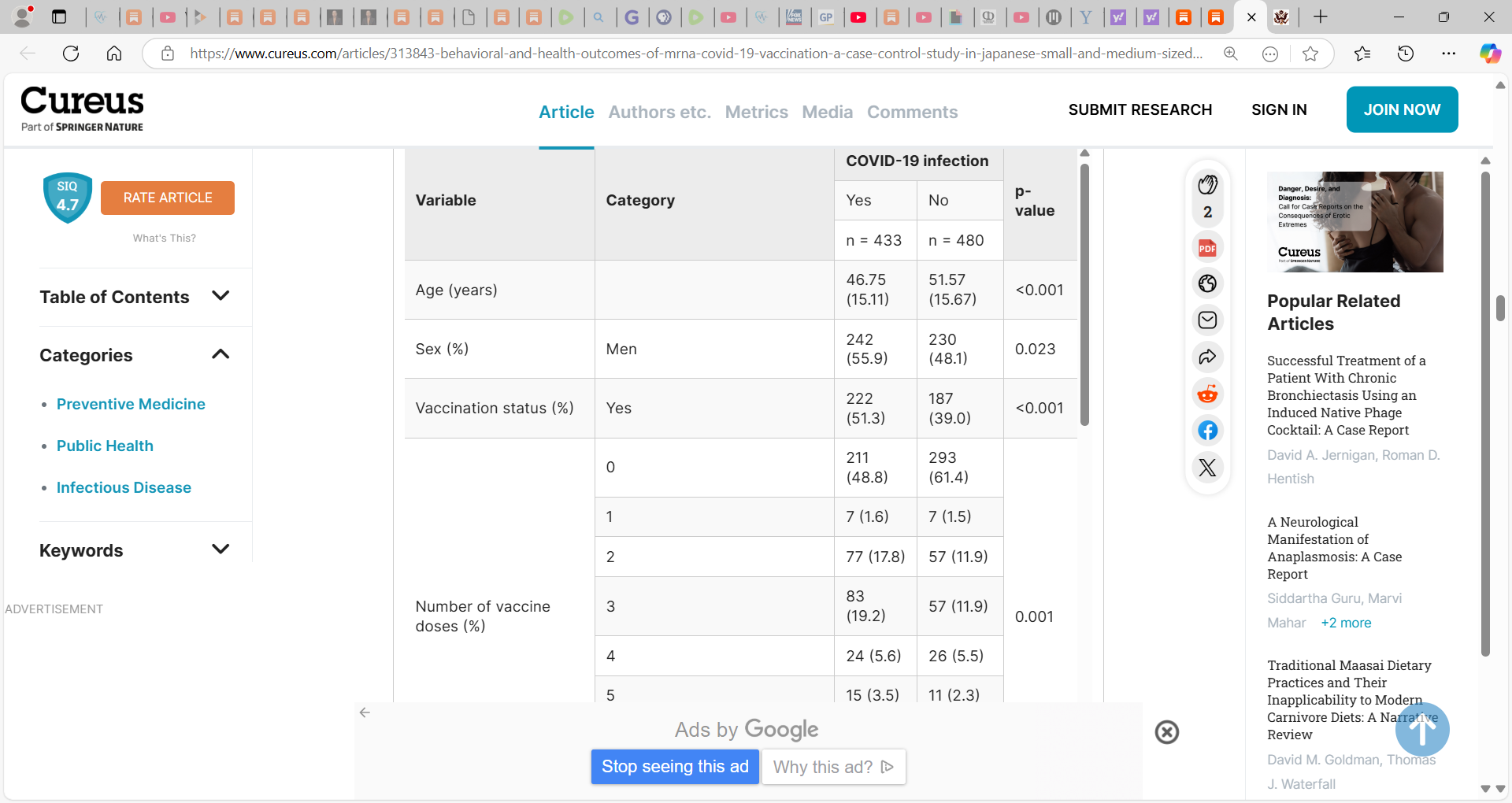
A total of 913 participants were included in the final analysis. The adjusted ORs for COVID-19 infection among vaccinated individuals compared to unvaccinated individuals were 1.85 (95% CI: 1.33-2.57, p < 0.001). The odds of contracting COVID-19 increased with the number of vaccine doses: one to two doses (OR: 1.63, 95% CI: 1.08-2.46, p = 0.020), three to four doses (OR: 2.04, 95% CI: 1.35-3.08, p = 0.001), and five to seven doses (OR: 2.21, 95% CI: 1.07-4.56, p = 0.033). Behavioral analysis indicated that a reduced frequency of bathing and exercising was significantly associated with higher COVID-19 infection rates (p < 0.05).
Conclusions
The study observed a higher reported incidence of COVID-19 infection among vaccinated individuals during the pandemic period, which increased with the number of vaccine doses received.’
This study observed a higher incidence of COVID-19 infection among vaccinated individuals, escalating with the number of vaccine doses received.’
Important issues when considering the findings of this study and I raise issues with the methodology and analysis, but on balance, the findings add to the evidence and raise important questions:
‘The paper entitled, ‘Behavioral and Health Outcomes of mRNA COVID-19 Vaccination: A Case-Control Study in Japanese Small and Medium-Sized Enterprises’ written by Dr. Nakatani et al. concludes higher reported incidence of COVID-19 infection among vaccinated individuals than unvaccinated individuals. However, this study raises several concerns that cannot be overlooked.
First, although the title of the study contains “Case-Control Study,” this is not a case-control study. ‘The case-control study starts with a group of cases, which are the individuals who have the outcome of interest. The researcher then tries to construct a second group of individuals called the controls, who are similar to the case individuals but do not have the outcome of interest’ [1]. In this study, however, the researcher first collects whole study subjects and then divides them into two groups: one with outcome and one without outcome. In this respect, the retrospective cohort approach, which divides the entire subject population by exposure, and examines outcome status by exposure group, is more natural and straightforward. Because the authors chose the framework of a case-control study, Table 1 is divided by outcome information, and an important information of the distribution of potential confounders by exposure status is not known.
Second, the primary outcome of this study was the presence or absence of self-reported COVID-19 infection. However, the time frame of the outcome was not questioned and a longitudinal analysis could not be performed. If a subject was infected with COVID-19 before the first vaccination and then received six additional vaccinations and prevented the infection, then vaccination cannot be the cause of COVID-19 infection. In the study, however, the association would be observed between the vaccination and the infection. Without knowing the time frame of the outcome, a causal relationship cannot be discussed.
Third, the study is inadequate in describing important information. Most importantly, all of the subjects were Yamato project participants and/or employees of SMEs, whose attributes were not described at all. Moreover, the actual questionnaire used is not shown, and the specifics of the questions are not clear. For example, we do not know what “eating habits” refers to. Throughout this paper, such descriptions are severely lacking. In addition, the data set is not publicly available.
Fourth, the studies were derived from two different populations but were combined without assumption. Here, we would like to point out the possibility of confounding due to the different backgrounds of the two groups, Yamato project participants and employees of SMEs. Confounding could occur if the vaccination or infection status of the two groups differs. Adjustment for the groups or confirmation of the absence of confounding is essential.
Fifth, the study population was described by the authors as “the study team believed that the participants reasonably approximated the broader workforce of SMEs in Japan”. However, 504 of the 913 subjects (55.2%) were unvaccinated. Considering that the proportion of unvaccinated persons aged 20 years or older in Japan is 11.6% [2] (as of April 1, 2023), this is a biased population with approximately five times as many unvaccinated persons and is not representative. In this paramount matter, the “reasonable approximation” is completely false. The authors are accountable for the type of population which they chose, why the unvaccinated rate is so high, and with what intent the “reasonable approximation” statement was made.
And last but not least, the validity of the odds ratios is not fully considered. For the odds ratio to be valid, the accuracy of COVID-19 diagnosis must be constant regardless of vaccination status. However, it is conceivable that vaccination is associated with diagnostic diligence for the disease in question, in which case there would be a difference in diagnostic accuracy, resulting in information bias. This bias increases the odds ratio without causality.’
Some very important input here above by SADAO SUZUKI, MD, PhD and I thank him for this.
___
You must not wait for another catastrophic crisis (at times manufactured but we are prevented from making our own basic personal decisions or accessing needed drugs and response tools) to catch you off-guard. We must take charge and be prepared today so that we can enjoy peace of mind tomorrow.
Enter the Wellness Company as a solution and a willing participant in the health care conversation. From telemedicine, prescriptions, memberships, and supplements, TWC is leading America with alternative choices to the traditional health care model.
If you wish to give a donation to help me, you can at:
Zelle:
sr7283@gmail.com
Or Ko-Fi
Ko-fi.com/drpauleliasalexander
Or to my address at:
150 South 8th Street
Unit 170
Lewiston, New York
14092
Alternatively, please consider going from an UNPAID subscriber or follower to a PAID at $5 per month or $30 per year. This can provide me help. If this is not possible at this time, this is ok, please remain a subscriber for FREE and there is no difference between FREE and PAID. No restrictions.
Please consider support of a good PATRIOT company (in this PATRIOT economy) Drs. McCullough, Risch, Thorp, myself support (they are our sponsors), The Wellness Company; see the emergency preparation kit (key component being antibiotics you were denied by doctors, pharmacists, governments during the fraud COVID), first aid kit, travel emergency kit, contagion control kit etc. Please consider the SPIKE SUPPORT (spike protein DETOX dissolving spike from mRNA vaccine, this is critical to remove spike form the mRNA vaccine/and DNA viral vector) formula with NATTOKINASE as well as the triple formula (SPIKE SUPPORT, BROMELAIN, CIRCUMIN)
I have decided to again share research, poorly done as they were, again, so that Trump, Bobby Jr., Makary, Jay et al. cannot say 'oh we did not know'...oh, btw, my substack is printed and read widely in the orbit...I know for I deal with people there and across the last 2 years it is used to help uncork heavy constipation for it gives them diarrheas...so they need it as to see what I am thinking and it helps them go to the washroom. I AM TOLD THE COMMENTS SECTION HERE IS VERY INFORMATIVE TO THE INTERNAL ORBIT. THEY READ OTHERS TOO BUT MINE IS A STAPLE DIET TO RAISE BLOOD PRESSURES AND GET PULSE UP
Trump was betrayed, along with the entire US, and humanity itself, by Pence who was Trump's "Covid Czar." Trump, like all transformational leaders, is not a micromanager and that enabled Pence to deceive him. Pence must be made to carry the can for the devastating harm caused by the mRNA injections. There is a special place in hell for Pence.