Did Kedl show us that there is a risk (not only theoretical but real) of aerosol transmission of COVID mRNA vaccine antibodies between vaccinated parents & children? Yes! 100%; thus spike, mRNA, LNPs!
Be warned, this is a 'real' risk (paging Makary, Bhattacharya et al.); children can receive all the parents get via vaccine via placental, breast milk, aerosolize, skin, saliva etc., LNPs to spike

What did Kedl show?
Kedl et al. showed us evidence for Aerosol Transfer of COVID-specific Humoral Immunity (antibodies); we are left to then ask, can lipid-nano particles (LPN), spike protein & mRNA also be aerosolized? As such, shed?
Yes, yes, yes, and yes a 4th time! see my prior stack on this; see Keld et al. below. Finding antibodies on the inside of the masks in vaccinated persons indicates transmission
‘The data…from human nasal swabs provides evidence for the aerosol transfer of antibodies (Abs) between immune and nonimmune hosts.’
So, can unvaccinated children in close juxtaposition to their vaccinated parents go on to manifest and develop an immune response to spike protein, unlike those children with unvaccinated parents? Is there shedding then? What is your view?
Human serum, saliva, and nasal swabs were obtained (Institutional Review Board approval no. 20-1279). Surgical masks were anonymously donated by laboratory workers at the end of one work day.’
identified anti-SARS-CoV-2–specific Abs eluted from surgical face masks that were worn for 1 work day by vaccinated laboratory members. Consistent with the results reported by others, we identified both IgG and IgA in saliva from vaccinated individuals (Fig. 1C, 1D). It was therefore not surprising to detect both IgG and IgA following elution from face masks (Fig. 1C, 1D).’
‘comparison of nasal swabs acquired from children living in vaccinated households revealed readily detectable SARS-CoV-2–specific IgG (Fig. 1E), especially when compared with the complete deficit of SARS-CoV-2–specific Ab detected in the few nasal swabs we obtained from children in nonvaccinated households.’
Evaluation of samples in this fashion revealed that high intranasal IgG in vaccinated parents was significantly associated (p = 0.01) with a 0.38 increase in the log-transformed intranasal IgG gMFIs within a child from the same household (Fig. 1F). This significant positive relationship was observed using either parametric or nonparametric analysis, and adjustments for the correlation within household did not alter the conclusion.’
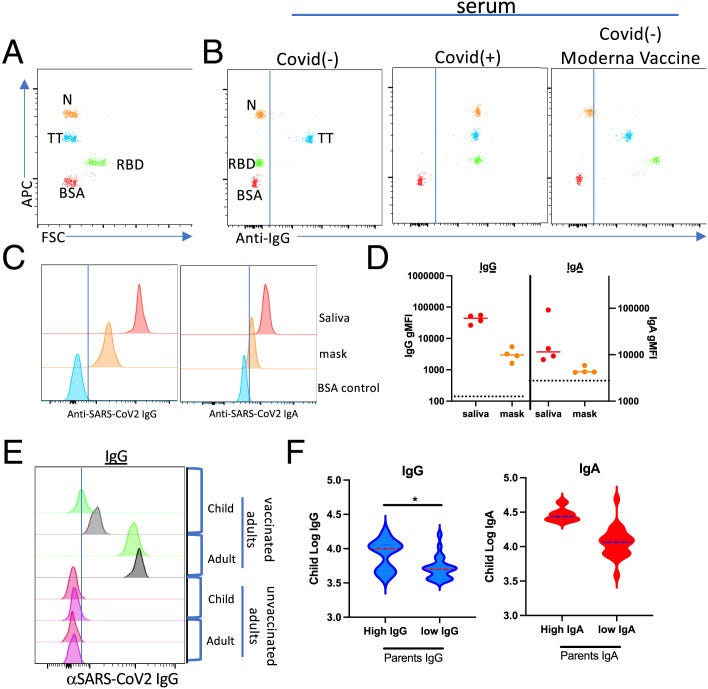
Evidence for aerosol transfer of SARS-CoV-2–specific immunity.
In short, the findings revealed elevated IgG in the nostrils (intranasal) of vaccinated parents that was “significantly associated” with an increase in intranasal IgG in the children who were unvaccinated and living in the same household; how do you think this happened? they also found no COVID antibodies in the nasal swabs taken from children residing in the nonvaccinated family homes. Same for IgA. IMO, this is clear aerosol transfer transmission of antibodies and I mean from virus or vaccine-induced. Parent to child. This means same for the intact spike protein (vaccine-induced), spike fragments, mRNA, micro mRNA, mRNA fragments, antibodies, lipid-nano particles (LNPs) etc.
All of it and parents must understand that vaccinating you, while child is in utero or even older children, infants, children, teens etc. is akin to vaccinating them. This is ‘passive immunization’ potentially via respiratory droplets. Like droplet infection. I am not talking about if the antibodies can confer any protection for we know from all the science today that the mRNA vaccine failed and were ineffective, into negative efficacy and effectiveness territory rapidly, with waning immunity near instantly and we know that it is devastatingly harmful, up to including causing death.
https://brownstone.org/articles/16-studies-on-vaccine-efficacy/
See Figures in Kedl et al.:

Legend for above figures:
Evidence for aerosol transfer of SARS-CoV-2–specific immunity.
‘(A and B) Representative flow cytometric results from the use of a multiplex microsphere immunoassay (MMI) (A) evaluating serum samples from a COVID-19–negative (B, left), COVID-19–positive (B, middle), and Moderna mRNA vaccinee (B, right). N, nucleocapsid protein; RBD, receptor-binding domain; TT, tetanus toxoid. Note that the TT reactivity serves as a positive control for validating sample quality in the assay. (C and D) Histograms showing the MFIs for Wuhan-RBD–specific IgG (left) and IgA (right) from saliva or eluted from a surgical mask worn for 1 work day. (D) Quantification of IgG and IgA gMFI eluted from masks obtained from four individuals. Dotted lines indicate gMFI obtained for COVID-19/vaccine− sample. (E) Histograms showing the MFIs for Wuhan-RBD–specific IgG eluted from nasal swabs from unvaccinated children living in households in which parents or family members were either vaccinated (top) or unvaccinated (bottom). Gray and green histograms represent histograms from two separate children in whom high (gray) versus low (green) RBD Abs were identified. (F) Log transformation of the gMFI for Wuhan-RBD–specific IgG (left) or IgA (right) from 34 adult/child pairs using Ab cutoffs for high versus low parental intranasal Ab levels. Cutoff between adult high and low samples was determined as described in Materials and Methods.’
SOURCE:
___
You must not wait for another catastrophic crisis (at times manufactured but we are prevented from making our own basic personal decisions or accessing needed drugs and response tools) to catch you off-guard. We must take charge and be prepared today so that we can enjoy peace of mind tomorrow.
Enter the Wellness Company as a solution and a willing participant in the health care conversation. From telemedicine, prescriptions, memberships, and supplements, TWC is leading America with alternative choices to the traditional health care model.
If you wish to give a donation to help me, you can at:
Zelle:
sr7283@gmail.com
Or Ko-Fi
Ko-fi.com/drpauleliasalexander
Or to my address at:
150 South 8th Street
Unit 170
Lewiston, New York
14092
Alternatively, please consider going from an UNPAID subscriber or follower to a PAID at $5 per month or $30 per year. This can provide me help. If this is not possible at this time, this is ok, please remain a subscriber for FREE and there is no difference between FREE and PAID. No restrictions.
Please consider support of a good PATRIOT company (in this PATRIOT economy) Drs. McCullough, Risch, Thorp, myself support (they are our sponsors), The Wellness Company; see the emergency preparation kit (key component being antibiotics you were denied by doctors, pharmacists, governments during the fraud COVID), first aid kit, travel emergency kit, contagion control kit etc. Please consider the SPIKE SUPPORT (spike protein DETOX dissolving spike from mRNA vaccine, this is critical to remove spike form the mRNA vaccine/and DNA viral vector) formula with NATTOKINASE as well as the triple formula (SPIKE SUPPORT, BROMELAIN, CIRCUMIN)
So, if a child has not been vaccinated and the parents have not been vaccinated, and the child attends school with children who have not been vaccinated, but those children have parents who have been vaccinated, is the child who attends school with other children of vaccinated parents at risk for mRNA transfer?
I became concerned - and remain so to this day - when years ago I first heard that the *jabbed* could potentially be dangerous (shedding and all that). As time went on, that 'potential' became confirmed with study after study. And now it's in the food, air and water. Good grief!!!
We are all literally surrounded by the "vaccinated" - there's no realistic way of getting away from them (short of moving to an isolated cave on some Himalayan mountain).
The mRNA jabs -- the gift that keeps on giving!! Ah, but Fauci is fully pardoned.