

Dr. Joe Ladapo's letter from CDC & FDA (March 10th 2023) show us why CDC & FDA are led by incompetent (Drs. Walensky & Califf), academically sloppy, vapid, specious, & intellectually lazy technocrats
Sheer absurdity; they showed in a March 10th 2023 reply to Dr. Ladapo just how incompetent & inept they are as they defended VAERS COVID vaccine data & why CDC & FDA (NIH) must be stripped to studs

First, LIABILITY PROTECTION.
Drs. Walensky and Califf, if you both stand by the COVID gene injections, the mRNA platform especially, for you said in your letter to Dr. Ladapo it is ‘safe and effective’, why don’t you put liability protection on the table? Put it on the table, let us see how brave you are and then remove it. Be a man and woman about it, stand by your gene injection and remove the protections you enjoy. Allow an equal playing field so parents can take you into a court for compensation as their children have died and more will die from it. Remove liability protection! There is literally no sound basis, no rational argument or scientific or medical data that can justify and underpin giving any health child or young person any of these vaccines.
The reality is that CDC, NIH, FDA, NIAID must be taken down to the very studs, fumigated, striped down, with 100 officials top down across all alphabet health agencies including HHS, fired. Fired! In fact, if the Fire Marshall where these buildings are located can evacuate the buildings completely, and they think they could be razed safely, I say raze them. All of them! They, these alphabet health agencies collectively functioned in 2020 (and the three years prior) to hurt and subvert an elected President with false, incomplete, deliberately inaccurate, reckless COVID data and policies that hurt the POTUS but catastrophically, devastated the American people. Catastrophic mistakes were made yet it has become increasingly clear that these alphabet agencies operate with some level of ineptness, yet malfeasance. I have to think so. I do not want to, yet have to.
Truth is, CDC, NIH, FDA etc. as once premier health agencies in the US, are the purveyors of false, fraudulent, inaccurate misinformation and have lost most of their credibility among the public. They are now political agencies and it was clear the public health response during the pandemic became a political one by them.
The public simply does not believe what you the CDC and FDA says, nor NIH or NIAID, nor HHS. All corrupted. You earned that by your corruptibility, politicization, and deceit across the last 3 years but I argue this is how you always operated. COVID revealed the underbelly of you, your ‘always’ role. COVID ‘crystalized’ you. COVID peeled back the onion for us. What we the public have seen is horrendous and not just for these health agencies, but human behavior such as the leeches who used COVID to enrich themselves on the backs of suffering people! Took their miserable inconsequential lives and became ‘COVID experts’. We have leeches using the public and donors using their money for their own aims, in all of this, the public hurts. The public was always the loser.
What can I say after reading the inane and vacuous March 10th 2023 reply by Drs. Walensky and Califf to Dr. Ladapo? It is a simple question you must answer to scientists and doctors like Ladapo and McCullough, Risch, Oskoui, Brinkley, Littell etc. and me, which is what is the data and science you are basing, and have based your COVID policies on? Where is the randomized trial data (RCT)? Where is it? Where is the RCT data for children? What? Where? We cannot seem to find it so please point us to it. What data Drs. Walensky and Califf? What different data do you have, that you based your COVID and vaccine policy decisions on for it is very different from the core mainstream data? For we cannot find it and we are exhausted looking for it. Can you show the science to us so that we can make sense of your policies as well as the letter you wrote (March 10th, 2023) to Dr. Ladapo for the letter says a tremendous lot yet really says absolutely nothing. It, to me, is complete utter nonsense and absurdity. It really is nonsensical and no serious scientist can read it without a chuckle or two.
You out of the box cited studies that are not optimal comparative effectiveness research designs, not trustworthy, not of high quality, grossly methodologically flawed, deficient in statistical analyses, and largely confounded (residual confounding) and plagued with selection bias, without control for key confounders such as early treatment effects, natural immunity effects, healthy vaccinee effects since persons who seek vaccines and treatment tend to take better care and are healthier to begin with, differential in health care as well as improved health care across study period, co-morbidities etc. These factors can have staggering effects on the resulting estimates of effect. You use and cite studies with small sample sizes, small outcome event numbers, short duration of follow-up, selective reporting, heavily conflicted by industry sponsorship, and write-ups that omit key important information for the reader to understand the methods.
You CDC and FDA use antibody titer levels as the primary patient outcome which is not patient important. How could you use antibody levels for decision making? You know it is not a proxy for immunity. You use corrupted methods such as ‘immuno-bridging’ that makes no sense. So how could a reader like me with steep evidence-based methods and epidemiology training, or Dr. Harvey Risch, Dr. Ramin Oskoui, Dr. Peter McCullough, Dr. Howard Tenenbaum etc. ever take you seriously. In large part what you say is ludicrous to us and certainly to Dr. Joe Ladapo. We laugh when we read your reports and letters such as this one which is the subject of my substack. I even argue it smacks of discrimination. You dismiss his letter out of hand, ex cathedra, yet you both can not stand in his shoes technically, intellectually or otherwise, even with 95% of his brain left at home. Yet you write so very dismissively. Typical.
I am defending Dr. Joe Ladapo and his reach out to you. You CDC and FDA failed in your response.
Let me start by saying nothing about these mRNA technology gene injection vaccines have been safe and effective, nothing! IMO should have never been brought in the first place.
You CDC and FDA slam Dr. Ladapo’s letter and incredibly, even try to relegate and quasi-question your own VAERS database (that is the subject) that has always served as a red-flag ‘signal’. No doubt it is not perfect or optimal especially since it captures at most 10% of the vaccine harms and deaths, yet it is very useful and you cannot simply disregard it NOW out of convenience given Dr. Ladapo’s focus on it. How could you now discount your own vaccine adverse reporting VAERS database? This is why the CDC has credibility of zero (0). You and FDA cannot be taken seriously. You are a joke to the public.
Your motive is clear Drs. Walensky and Califf as per your response letter to Dr. Ladapo, in that you are continuing to push the failed and deadly COVID mRNA technology gene injection. You continue to deny the dangers of the fraud gene shot while Americans continue to fall victim to it. A recent survey (Rasmussen Reports) showed that more than 25% of Americans know of someone harmed by the vaccines. Did you know that or are you even interested to know this? This statistic to me, should be very worrying.
There is no credible basis as to why this COVID gene injection has not been pulled from the market. This IMO has to do with greed, corruption, ineptness, malfeasance, intended harm. Has to be. If I were to step back and ask then, are you deliberately at CDC and FDA, trying to harm Americans? Did you and do you continue to by advocating for these dangerous shots? Is this your intent? To harm people? I am inclined to say ‘yes’.
With all of the ‘died suddenly’ in the media and clearly credible cases? You pretend and still push the shots? With all the ‘dying at dawn in your sleep’? You still push the shot? Does this not bother you Drs. Walensky and Califf? All of the ‘deaths unknown’? What do you think of that? Have you ever seen anything like that before Drs/ Walensky and Califf? I have not. All of the reports of mRNA and fragments, spike protein, and spike sub-units circulating for way too long (some say maybe life-time?) and beyond what you the CDC stated on your websites that the mRNA/vaccine content stays at the injection site and dissolves rapidly. Why did you CDC deceive the public in that way for it drove people to take the shot and many have died. What do you say about that, given we know clearly that it leaves the injection site and can be found throughout the body? Why did you FDA not mandate and demand that the vaccine maker study the long-term effect of spike and mRNA staying in the body? So much evidence of myocarditis in young persons and athletes, thrombosis, and neurological harms. Does this not concern you Drs. Walensky and Califf?
To be honest, this is the only thing that makes sense to me, incredible as it sounds, that there must be some level of malfeasance. Something other than science seems at play here and we have to figure this out to get proper justice and accountability.
You Drs. Walensky and Califf, IMO, continue to act in reckless and dangerous ways for you could not be that inept to not grasp the science as well as observe around you how extensively the vaccine has failed. How much harm it is doing. You yourself Dr. Walensky got five shots yet got re-infected. Did you not?
You Drs. Walensky and Califf know full well that these COVID gene injections are non-sterilizing and do not stop infection, replication, or transmission. Do not confer immunity and unless we cut the chain of transmission, one could never get to herd immunity. You knew these shots could not get us to herd immunity yet you pushed it out. You know full well that these COVID gene injections (mRNA technology) are driving viral immune escape and the emergence of infectious variants (immune tolerance, viral immune escape, original antigenic sin (immune fixation, immune priming, immune hypnotism on the initial prime or exposure), and paradoxical priming and auto-immune disease.
You know full well these sub-optimal non-neutralizing vaccine-induced antibodies (rolled out into the teeth of a pandemic and thus high infectious pressure/circulating virus) induced while there is mounting sub-optimal immune pressure (vaccinal antibodies not yet arrived at its full ‘binding affinity’ and so are non-neutralizing) are driving infectious variants and giving the virus properties it prior did not have e.g. increased infectiousness, and to the vaccinated. The vaccinated are becoming infected, re-infected, severely ill and some are dying. You know full well it was never a pandemic of the ‘unvaccinated’, but rather a pandemic of the ‘vaccinated’ and that you lied and created a false narrative by re-defining what being ‘vaccinated’ meant.
You know full well that this dangerous mRNA technology injection is implicated in blood clots, bleeding, myocarditis, pericarditis, strokes, heart attacks, subversion of the immune system (innate and acquired-adaptive), neurological illness etc. Yet with all of the devastation and risk linked to the COVID gene shots, you wrote that negative letter to Dr. Ladapo when he sought urgently to signal you of the startling adverse event and death data in VAERS and due to the COVID gene injection. You at CDC continue to write (via your pseudoscientific MMWR) and invoke studies that you know are deeply flawed and which lack the methodological rigor to stand up to proper scientific scrutiny. You ‘select’ studies for inclusion and apply methods that are often incorrect and your statistical analyses are grossly misplaced and wrong. Do you at CDC, Dr. Walensky, ever proof-read the drivel that you publish? Yet you at CDC just do not care for you have your deeply flawed MMWR to publish in.
Really, what is there to say for I am embarrassed by these two public health and regulatory leader dolts and I take umbrage by their inane and specious letter, itself devoid of proper scientific depth and breadth coming from leaders of the CDC and FDA. It is shameful. These two health officials by the letter’s content exhibit a level of cognitive dissonance matched only by Fauci and Francis Collins. This letter shown below by CDC and FDA reveals why they are two of the dumbest public health figures heading our alphabet health agencies in America. It is clear that Walensky and Califf simply cannot read data or evidence, cannot understand the science, are blinded to it, do not ‘get’ it, are biased and politicized to it, and are just plain inept and malfeasant. I argue there must be some level of malfeasance for they cannot be that incompetent. To make sense of their actions, one must only conclude that something other than science is at play. What then??
Dr. Rochell Walensky and Dr. Robert Califf as well as the head of NIH and HHS with their polices, with the obvious inability to read and understand the COVID and vaccine science and data (as I would show below), is a great disservice to both individuals and public health. It is devastating, the harms visited upon America by the leaders of these alphabet health agencies in America and I mean in both the Trump and Biden Administrations. Their leadership has been catastrophic for they have been 100% flat wrong on everything and they costed lives, hundreds of thousands of lives. People died because of them. Their decisions. The CDC, NIH, FDA, NIAID, and HHS have made statements and implemented policies throughout the 3 years of the COVID ‘so-called’ pandemic that have been incorrect, misleading and very harmful to the American public. I argue they have been and have caused far reaching harms and many deaths.
So from my vantage, when someone like Dr. Joe Ladapo comes along, they are unsettled by him, his sheer academic depth and breadth, his reach, his leadership, his compassion for the American suffering, and I dare say they are rankled and rattled by him. They are unable to match wits and technical competence with him and so dismiss him out of hand. They clearly did not re-read the tripe and drivel that they wrote on March 10th 2023 for it was devoid of any scientific merit. Drs. Walensky and Califf seemed to not understand basic and long-established scientific principles. It is rather shocking that these two corruptible dimwits lead these two esteemed health agencies, one being the nation’s regulator.
Let me explain why by simply stating ‘first’ Dr. Ladapo’s core argument that set off the fire-storm, followed by the CDC and FDA’s response, and then why they are so very incredibly inept and wrong by laying out my response immediately after. I will deal with this by sharing the studies and science that refute and call into serious questions the contention of CDC and FDA, and urge Walensky and Califf to please read the contained science, abreast themselves fully, and then to re-write their response to Dr. Ladapo beginning with an apology. They may also be well served by inviting Dr. Ladapo to their campuses to see how they can benefit by his steep grasp of the devastation at hand due to the COVID injections (and policies in general).
Let me set the table by reminding Drs. Walensky and Califf of a recent report in Rasmussen Reports whereby massive numbers of Americans reported their views on the adverse effects and deaths from the COVID vaccine.
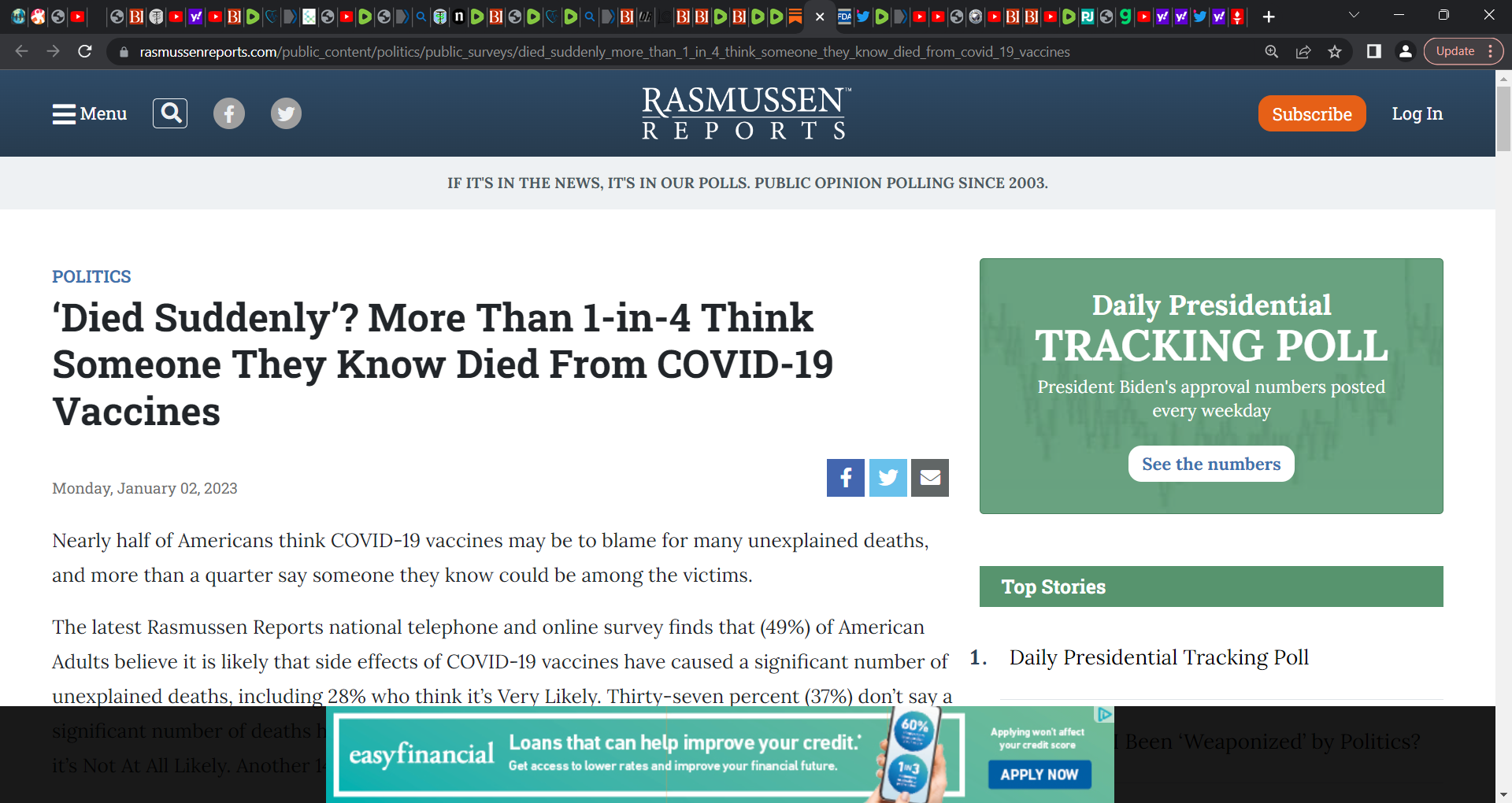
Rasmussen national and online survey reported that ‘Nearly half of Americans think COVID-19 vaccines may be to blame for many unexplained deaths, and more than a quarter say someone they know could be among the victims.’ The report stated that ‘(49%) of American Adults believe it is likely that side effects of COVID-19 vaccines have caused a significant number of unexplained deaths, including 28% who think it’s Very Likely.’ The Report shockingly indicates 28% of Americans know someone who has died after the vaccine. You have to let this data sink in a bit.
It is not ‘misinformation’ about COVID vaccine safety that has caused Americans to avoid getting the vaccines they need to be up to date. Not misinformation, it is the actual data and evidence that has accumulated across nations and actual persons sharing the reality (using IT media) that the vaccine is harmful and kills. They have been harmed and know of loved ones and colleagues who have died, often on the same day as the shot or one day post COVID gene shot or soon after (next few days). Where are the respective reports from CDC etc. on cause of death so that people can be optimally informed for their own decision-making? Yet really, how could people be informed when from day one, you denied them being informed of both the benefits and harms of the gene injection?
Fact is most all of Americans know someone in their family, friends, acquaintances, as well as work colleagues who have been hurt by the COVID gene injections or may have died.
Statements by Dr. Ladapo to CDC and FDA (key):
‘In Florida alone, we saw a 1,700% increase in reports after the release of the COVID-I9 vaccine, compared to an increase of 400% in vaccine administration for the same period. The reporting of life-threatening conditions increased 4,400%.’
‘According to a recent study, mRNA COVID-1 9 vaccines were associated with an excess risk of serious adverse events, including coagulation disorders, acute cardiac injuries, Bell's palsy, and encephalitis, to name a few. This risk was I in 550, much higher than other vaccines. To claim these vaccines are "safe and effective" while minimizing and disregarding the adverse events is unconscionable.’
Statements by CDC and FDA to Dr. Ladapo in bolded italics and quotations and my response immediately after:
CDC & FDA’s statement to Dr. Ladapo:
i)“The FDA-approved and FDA-authorized COVID-19 vaccines have met FDA’s rigorous scientific and regulatory standards for safety and effectiveness and these vaccines continue to be recommended for use by CDC for all people six months of age and older. Both FDA and CDC have continued to collect outcome data from multiple sources that demonstrate the clear benefit of COVID-19 vaccines in preventing death, serious illness, and hospitalization from SARS-CoV-2 infection, along with indicating a modest benefit in the prevention of infection and transmission that wanes over time, even as new variants have emerged. Additional benefits include a reduced risk of known complications from SARS-CoV-2 infection, including post-COVID conditions, COVID-19- associated stroke and heart disease, and COVID-19-induced venous thromboembolism.”
My response:
Before I begin Drs. Walensky and Califf, are you by any chance aware of the recent systematic review and meta-analysis that shredded your credibility on natural immunity’s inferiority relative to vaccinal immunity? I mean, you have made the most incredibly non-sensical illogical and absurd statements and enacted polices that harmed people when you knew all along that no vaccine, none ever and to come, could ever confer immunity that is more complete, robust, rigorous, and bullet-proof than natural exposure immunity. I draw your attention to this paper just published in the LANCET when you get time, really so that you would stop making a fool of yourself when speaking publicly. Fact is that the recent systematic review and meta-analysis found natural immunity is/was “at least as high, if not higher” than that provided by Pfizer and Moderna injections, and “provides strong, lasting protection against the most severe outcomes of the illness.”
SOURCE:
Past SARS-CoV-2 infection protection against re-infection: a systematic review and meta-analysis
I would even draw you to a seminal review I did culminating (iterating) at this time with about 170 pieces of evidence showing that natural immunity is far more superior than vaccinal immunity, more robust, comprehensive, and bullet-proof.
SOURCE:
https://brownstone.org/articles/research-studies-affirm-naturally-acquired-immunity/
I even share some choice studies immediately below with you in case you want some focus and again, please share with your staff so that they can for once, understand the power of natural immunity.
Immunology and virology 101 taught us over a century that natural immunity confers potent protection against a respiratory virus’s outer coat proteins, and not just one, e.g. the SARS-CoV-2 spike glycoprotein. There is even strong evidence for the persistence of antibodies. Even your own CDC recognizes natural immunity for chicken-pox and measles, mumps, and rubella, yet stunningly, not for COVID-19.
We saw very early on post vaccine roll-out that the vaccinated were showing viral loads (very high) similar to the unvaccinated (Acharya et al. and Riemersma et al.), and the vaccinated were as infectious. Riemersma et al. also reported Wisconsin data that corroborated how the vaccinated individuals who get infected with the then Delta variant were potentially (and were) transmit(ting) SARS-CoV-2 to others (potentially to the vaccinated and unvaccinated). It became clear that the vaccinated and unvaccinated were at similar risk of infection and that the vaccinated were transmitting virus.
This troubling situation of the vaccinated being infectious and transmitting the virus emerged early on in seminal nosocomial outbreak papers by Chau et al. (HCWs in Vietnam), the Finland hospital outbreak (spread among HCWs and patients), and the Israel hospital outbreak (spread among HCWs and patients). These studies also revealed that the PPE and masks were essentially ineffective in the healthcare setting. Again, the Marek’s disease in chickens and the vaccination situation explains what we are potentially facing with these leaky vaccines (increased transmission, faster transmission, and more ‘hotter’ variants).
Several studies that should always be on your radar and I know by your prior polices you either did not read these or did not understand the science, including this potent study showing that natural immunity to the Spanish flu lasted 100 years:
Researchers find long-lived immunity to 1918 pandemic virus, CIDRAP, 2008 and the actual 2008 NATURE journal publication by Yu
“A study of the blood of older people who survived the 1918 influenza pandemic reveals that antibodies to the strain have lasted a lifetime and can perhaps be engineered to protect future generations against similar strains…the group collected blood samples from 32 pandemic survivors aged 91 to 101..the people recruited for the study were 2 to 12 years old in 1918 and many recalled sick family members in their households, which suggests they were directly exposed to the virus, the authors report. The group found that 100% of the subjects had serum-neutralizing activity against the 1918 virus and 94% showed serologic reactivity to the 1918 hemagglutinin. The investigators generated B lymphoblastic cell lines from the peripheral blood mononuclear cells of eight subjects. Transformed cells from the blood of 7 of the 8 donors yielded secreting antibodies that bound the 1918 hemagglutinin.” Yu: “here we show that of the 32 individuals tested that were born in or before 1915, each showed sero-reactivity with the 1918 virus, nearly 90 years after the pandemic. Seven of the eight donor samples tested had circulating B cells that secreted antibodies that bound the 1918 HA. We isolated B cells from subjects and generated five monoclonal antibodies that showed potent neutralizing activity against 1918 virus from three separate donors. These antibodies also cross-reacted with the genetically similar HA of a 1930 swine H1N1 influenza strain.”
There are also these:
Comparing SARS-CoV-2 natural immunity to vaccine-induced immunity: reinfections versus breakthrough infections, Gazit, 2021
“A retrospective observational study comparing three groups: (1) SARS-CoV-2-naïve individuals who received a two-dose regimen of the BioNTech/Pfizer mRNA BNT162b2 vaccine, (2) previously infected individuals who have not been vaccinated, and (3) previously infected and single dose vaccinated individuals found para a 13 fold increased risk of breakthrough Delta infections in double vaccinated persons, and a 27 fold increased risk for symptomatic breakthrough infection in the double vaccinated relative to the natural immunity recovered persons…the risk of hospitalization was 8 times higher in the double vaccinated (para)…this analysis demonstrated that natural immunity affords longer lasting and stronger protection against infection, symptomatic disease and hospitalization due to the Delta variant of SARS-CoV-2, compared to the BNT162b2 two-dose vaccine-induced immunity.”
Highly functional virus-specific cellular immune response in asymptomatic SARS-CoV-2 infection, Le Bert, 2021
“Studied SARS-CoV-2–specific T cells in a cohort of asymptomatic (n = 85) and symptomatic (n = 75) COVID-19 patients after seroconversion…thus, asymptomatic SARS-CoV-2–infected individuals are not characterized by weak antiviral immunity; on the contrary, they mount a highly functional virus-specific cellular immune response.”
Large-scale study of antibody titer decay following BNT162b2 mRNA vaccine or SARS-CoV-2 infection, Israel, 2021
“A total of 2,653 individuals fully vaccinated by two doses of vaccine during the study period and 4,361 convalescent patients were included. Higher SARS-CoV-2 IgG antibody titers were observed in vaccinated individuals (median 1581 AU/mL IQR [533.8-5644.6]) after the second vaccination, than in convalescent individuals (median 355.3 AU/mL IQR [141.2-998.7]; p<0.001). In vaccinated subjects, antibody titers decreased by up to 40% each subsequent month while in convalescents they decreased by less than 5% per month…this study demonstrates individuals who received the Pfizer-BioNTech mRNA vaccine have different kinetics of antibody levels compared to patients who had been infected with the SARS-CoV-2 virus, with higher initial levels but a much faster exponential decrease in the first group”.
“Researchers used vaccination records as well as clinical outcomes for 1,368,721 North Carolina residents 11 years of age or younger from October 29, 2021 to January 6, 2023.
Statistical methods used were ‘Cox regression to estimate the time-varying effects of primary and booster vaccination and previous infection on the risks of omicron infection, hospitalization, and death.’
‘For children 5–11 years of age, the effectiveness of primary vaccination against infection was 59.9% (95% confidence interval [CI], 58.5 to 61.2), 33.7% (95% CI, 32.6 to 34.8), and 14.9% (95% CI, 12.3 to 17.5) at 1, 4 and 10 months after the first dose;
the effectiveness of a monovalent or bivalent booster dose after 1 month was 24.4% (95% CI, 14.4 to 33.2) or 76.7% (95% CI, 45.7 to 90.0); and the effectiveness of omicron infection against reinfection was 79.9% (95% CI, 78.8 to 80.9) and 53.9% (95% CI, 52.3 to 55.5) after 3 and 6 months, respectively.
For children 0–4 years of age, the effectiveness of primary vaccination against infection was 63.8% (95% CI, 57.0 to 69.5) and 58.1% (95% CI, 48.3 to 66.1) at 2 and 5 months after the first dose, and the effectiveness of omicron infection against reinfection was 77.3% (95% CI, 75.9 to 78.6) and 64.7% (95% CI, 63.3 to 66.1) after 3 and 6 months, respectively.”
Researchers sought to ‘evaluate dynamics of antibody levels following exposure to SARS-CoV-2 during 12 months in Dutch non-vaccinated hairdressers and hospitality staff.’ A prospective cohort study design, ‘blood samples were collected every three months for one year, and analyzed using a qualitative total antibody ELISA and a quantitative IgG antibody ELISA. Researchers found that 95 of 497 participants (19.1%) ‘had ≥1 seropositive measurement before their last visit using the qualitative ELISA. Only 2.1% (2/95) seroreverted during follow-up. Of the 95 participants, 82 (86.3%) tested IgG seropositive in the quantitative ELISA too. IgG antibody levels significantly decreased in the first months (p<0.01), but remained detectable up to 12 months in all participants. Higher age (B, 10-years increment: 24.6, 95%CI: 5.7-43.5) and higher BMI (B, 5kg/m² increment: 40.0, 95%CI: 2.9-77.2) were significantly associated with a higher peak of antibody levels.’ These results indicate that ‘SARS-CoV-2 antibodies persisted for up to one year after initial seropositivity, suggesting long-term natural immunity.’
Protection against Omicron from Vaccination and Previous Infection in a Prison System, Chin, 2022
evaluated the protection conferred by mRNA vaccines and previous infection against infection with the omicron variant in two high-risk populations”; See Table S4 in supplementary for the important findings, there are zero (0) deaths in the unvaccinated (prior infected) and zero (0) deaths in the vaccinated; the study attempts to champion the vaccine yet the real finding is that there were no deaths on those unvaccinated in a closed high-risk prison population; these prisoners withstood death with their own immunity (natural immunity) and needed no vaccine.
Risk of BA.5 Infection among Persons Exposed to Previous SARS-CoV-2 Variants, Graca, 2022
These researchers applied a registry-based study design that indeed lacks the level of precision of a test-negative design. Yet as they rightly argue, the very large number of cases studied that covered all the residents of Portugal over 12 years old, allowed confidence in a derived risk estimate for individuals with prior BA.1/BA.2 infection that was robust and trustworthy enough and located close to an estimate from Qatar based on a test-negative design.
Background and findings:
“Portugal was one of the first countries affected by a BA.5 predominance. We used the national coronavirus disease 2019 (Covid-19) registry (SINAVE) to calculate the risk of BA.5 infection among persons with documented infection with past variants, including BA.1 and BA.2. The registry includes all reported cases in the country, regardless of clinical presentation.”
“We found that previous SARS-CoV-2 infection had a protective effect against BA.5 infection, and this protection was maximal for previous infection with BA.1 or BA.2. These data should be considered in the context of breakthrough infections in a highly vaccinated population, given that in Portugal more than 98% of the study population completed the primary vaccination series before 2022.”
“Overall, we found that breakthrough infections with the BA.5 subvariant were less likely among persons with a previous SARS-CoV-2 infection history in a highly vaccinated population, especially for previous BA.1 or BA.2 infection, than among uninfected persons.”
Elevated risk of infection with SARS-CoV-2 Beta, Gamma, and Delta variant compared to Alpha variant in vaccinated individuals, ANDEWEG, 2022
“We analyzed 28,578 sequenced SARS-CoV-2 samples from individuals with known immune status obtained through national community testing in the Netherlands from March to August 2021. We found evidence of an increased risk of infection by the Beta (B.1.351), Gamma (P.1), or Delta (B.1.617.2) variants compared to the Alpha (B.1.1.7) variant after vaccination. No clear differences were found between vaccines. However, the effect was larger in the first 14-59 days after complete vaccination compared to ≥60 days. In contrast to vaccine-induced immunity, there was no increased risk for re-infection with Beta, Gamma or Delta variants relative to Alpha variant in individuals with infection-induced immunity.”
“We found no association between previous infection and a new infection with Beta, Gamma, or Delta versus Alpha, suggesting that there is no difference in protection from a previous infection between Beta, Gamma, or Delta variants compared to the Alpha variant. This is in line with the similar relative risk reductions for re-infection found for the Alpha and Delta variant (9). Early studies showed that previous infection conferred better protection than vaccination without previous infection during the Delta period.”
Neutralization Escape by SARS-CoV-2 Omicron Subvariants BA.2.12.1, BA.4, and BA.5, Hachmann, 2022
“Six months after the initial two BNT162b2 immunizations, the median neutralizing antibody pseudovirus titer was 124 against WA1/2020 but less than 20 against all the tested omicron subvariants. Two weeks after administration of the booster dose, the median neutralizing antibody titer increased substantially, to 5783 against the WA1/2020 isolate, 900 against the BA.1 subvariant, 829 against the BA.2 subvariant, 410 against the BA.2.12.1 subvariant, and 275 against the BA.4 or BA.5 subvariant.
Among the participants with a history of Covid-19, the median neutralizing antibody titer was 11,050 against the WA1/2020 isolate, 1740 against the BA.1 subvariant, 1910 against the BA.2 subvariant, 1150 against the BA.2.12.1 subvariant, and 590 against the BA.4 or BA.5 subvariant.”
Duration of immune protection of SARS-CoV-2 natural infection against reinfection in Qatar, Chemaitelly, 2022
Researchers studied the duration of protection afforded by natural infection, the effect of viral immune evasion on duration of protection, and protection against severe reinfection, in Qatar, between February 28, 2020 and June 5, 2022. They conducted and included three national, matched, retrospective cohort studies so as to compare incidence of SARS-CoV-2 infection and COVID-19 severity among unvaccinated persons with a documented SARS-CoV-2 primary infection, to incidence among those infection-naive and unvaccinated.
They found that “effectiveness of pre-Omicron primary infection against pre-Omicron reinfection was 85.5% (95% CI: 84.8-86.2%). Effectiveness peaked at 90.5% (95% CI: 88.4-92.3%) in the 7th month after the primary infection, but waned to ~70% by the 16th month. Extrapolating this waning trend using a Gompertz curve suggested an effectiveness of 50% in the 22nd month and <10% by the 32nd month. Effectiveness of pre-Omicron primary infection against Omicron reinfection was 38.1% (95% CI: 36.3-39.8%) and declined with time since primary infection. A Gompertz curve suggested an effectiveness of <10% by the 15th month. Effectiveness of primary infection against severe, critical, or fatal COVID-19 reinfection was 97.3% (95% CI: 94.9-98.6%), irrespective of the variant of primary infection or reinfection, and with no evidence for waning. Similar results were found in sub-group analyses for those ≥50 years of age.”
Key is that protection of natural infection against reinfection wanes and may diminish within a few years. Viral immune evasion accelerates this waning. However, and very tantalizing is that protection against severe reinfection “remains very strong, with no evidence for waning, irrespective of variant.”
Naturally-acquired Immunity Dynamics against SARS-CoV-2 in Children and Adolescents, Patalon, 2022
Setting: Nationally centralized database of Maccabi Healthcare Services, an Israeli national health fund that covers 2.5 million people.
Participants: The study population included between 293,743 and 458,959 individuals (depending on the model), 5-18 years of age, who were unvaccinated SARS-CoV-2 naive persons or unvaccinated convalescent patients.
Evaluated three SARS-CoV-2-related outcomes: (1) documented PCR confirmed infection or reinfection, (2) COVID-19 and (3) severe COVID-19.
Results: Overall, children and adolescents who were previously infected acquired durable protection against reinfection (symptomatic or not) with SARS-CoV-2 for at least 18 months. Importantly, no COVID-19 related deaths were recorded in either the SARS-CoV-2 naive group or the previously infected group. Effectiveness of naturally-acquired immunity against a recurrent infection reached 89.2% (95% CI: 84.7%-92.4%) three to six months after first infection, mildly declining to 82.5% (95% CI, 79.1%-85.3%) nine months to one year after infection, then remaining rather steady for children and adolescents for up to 18 months, with a slight non-significant waning trend. Found that ages 5-11 exhibited no significant waning of naturally acquired protection throughout the outcome period, whereas waning protection in the 12-18 age group was more prominent, but still mild.
Conclusions: Children and adolescents who were previously infected with SARS-CoV-2 remain protected against reinfection to a high degree and policy decision makers should consider when and if convalescent children and adolescents should be vaccinated.’
Anti-nucleocapsid antibodies following SARS-CoV-2 infection in the blinded phase of the mRNA-1273 Covid-19 vaccine efficacy clinical trial, Follmann, 2022
“Evaluate anti-nucleocapsid antibody (anti-N Ab) seropositivity in mRNA-1273 vaccine efficacy trial participants after SARS-CoV-2 infection during the trial’s blinded phase…nested analysis in a Phase 3 randomized, placebo-controlled vaccine efficacy trial…at 99 sites in the US…trial participants were ≥ 18 years old with no known history of SARS-CoV-2 infection and at appreciable risk of SARS-CoV-2 infection and/or high risk of severe Covid-19…among participants with PCR-confirmed Covid-19 illness, seroconversion to anti-N Abs at a median follow up of 53 days post diagnosis occurred in 21/52 (40%) of the mRNA-1273 vaccine recipients vs. 605/648 (93%) of the placebo recipients (p < 0.001).” Substantially less N Ab (nucleocapsid antibodies are highly conserved and stable, unlike the mutable spike protein) emerged in the vaccinated than those who were unvaccinated. Prior mRNA-1273 vaccination influenced/impacted anti-nucleocapsid antibody seroconversion relative to those unvaccinated. This is a major concern if the mRNA vaccine is impacting N Ab inducement, for then the unvaccinated who are naturally exposed and infected and mount an immune response, will show a far superior and broad immune response that includes Ab to not only the mutable spike but also to other viral proteins such as the interior nucleocapsid protein (evidence of long-term acquired-adaptive natural immunity).
Effect of prior infection, vaccination, and hybrid immunity against symptomatic BA.1 and BA.2 Omicron infections and severe COVID-19 in Qatar, Altarawneh, March 2022
Qatar researchers investigated SARS-CoV-2 Omicron symptomatic BA.1 infection, symptomatic BA.2 infection, BA.1 hospitalization and death, and BA.2 hospitalization and death, between December 23, 2021 and February 21, 2022. The researchers conducted 6 national, matched, test-negative case-control studies were conducted to examine effectiveness of BNT162b2 (Pfizer-BioNTech) vaccine, mRNA-1273 (Moderna) vaccine, natural immunity due to prior infection with pre-Omicron variants, and hybrid immunity from prior infection and vaccination. They found that “Effectiveness of only prior infection against symptomatic BA.2 infection was 46.1% (95% CI: 39.5-51.9%). Effectiveness of only two-dose BNT162b2 vaccination was negligible at -1.1% (95% CI: -7.1-4.6), but nearly all individuals had received their second dose several months earlier. Effectiveness of only three-dose BNT162b2 vaccination was 52.2% (95% CI: 48.1-55.9%). Effectiveness of hybrid immunity of prior infection and two-dose BNT162b2 vaccination was 55.1% (95% CI: 50.9-58.9%).” The key finding was “There are no discernable differences in the effects of prior infection, vaccination, and hybrid immunity against BA.1 versus BA.2.”
“Evaluate 254 COVID-19 patients longitudinally up to 8 months and find durable broad-based immune responses. SARS-CoV-2 spike binding and neutralizing antibodies exhibit a bi-phasic decay with an extended half-life of >200 days suggesting the generation of longer-lived plasma cells… most recovered COVID-19 patients mount broad, durable immunity after infection, spike IgG+ memory B cells increase and persist post-infection, durable polyfunctional CD4 and CD8 T cells recognize distinct viral epitope regions.”
Now to the matter at hand in responding to CDC and FDA’s letter to Ladapo.
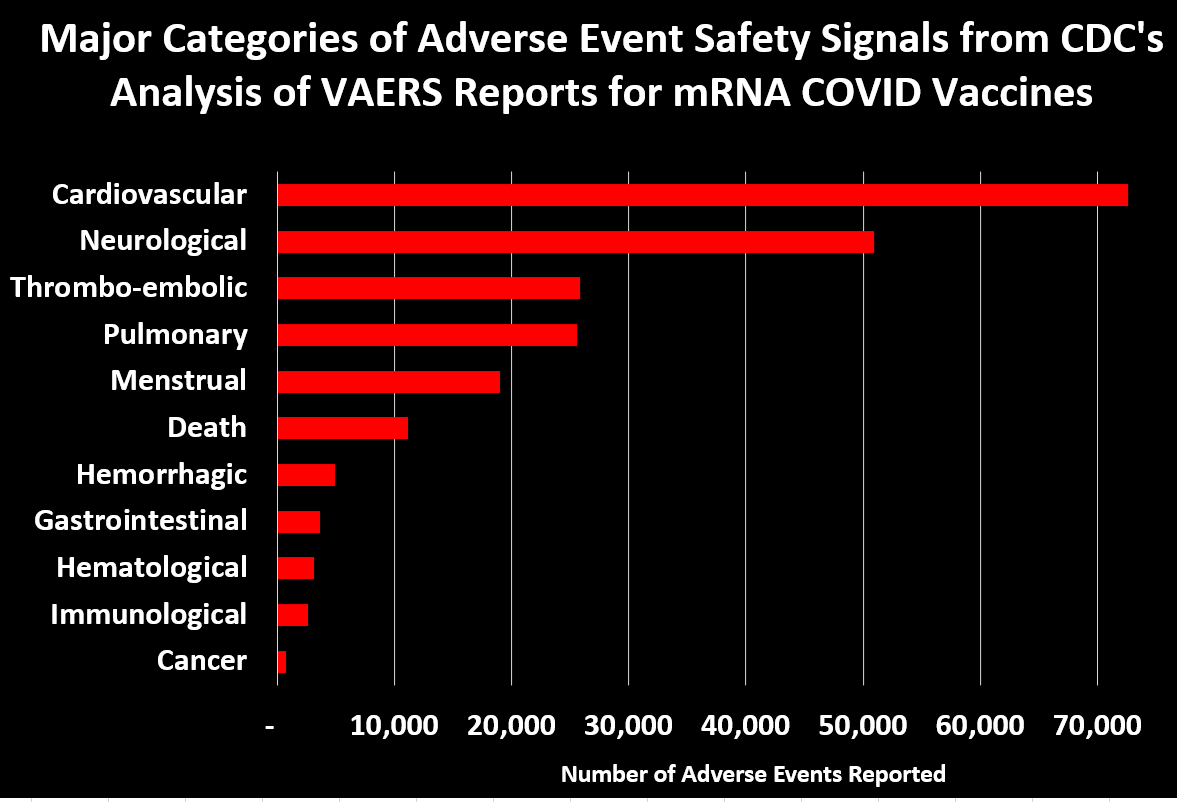
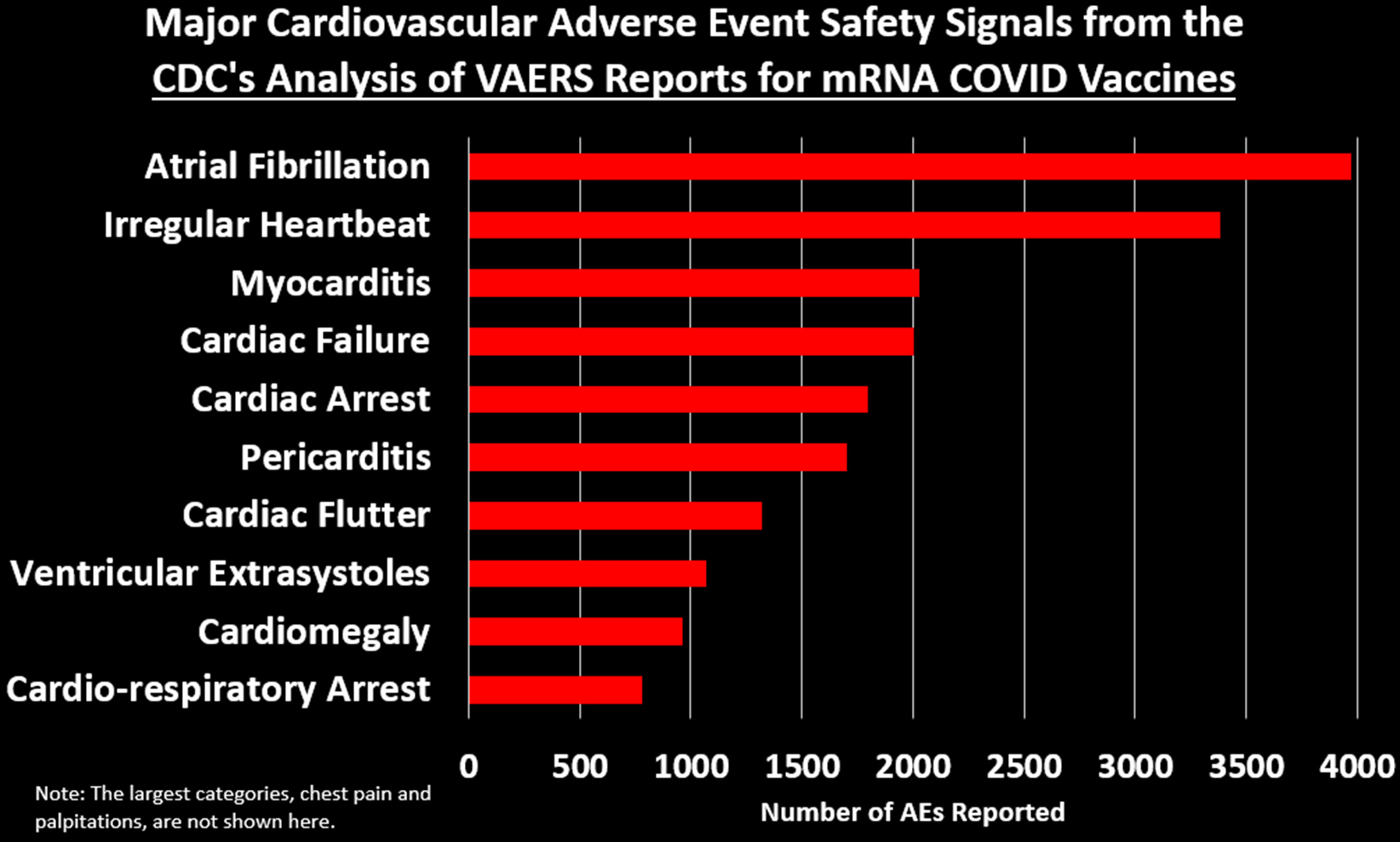
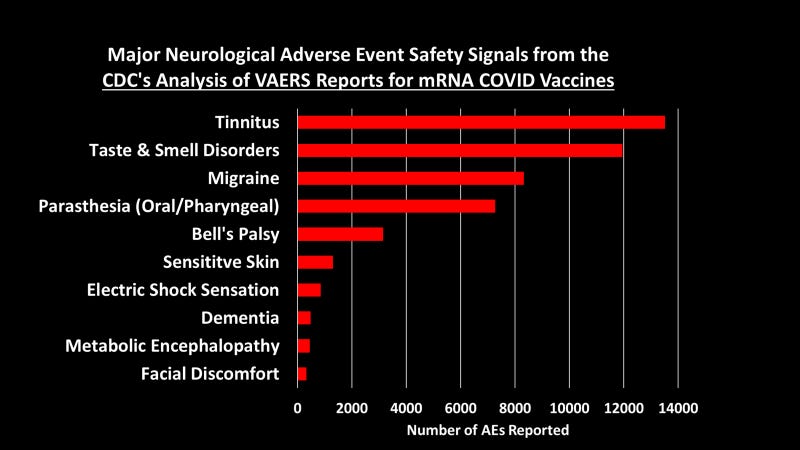
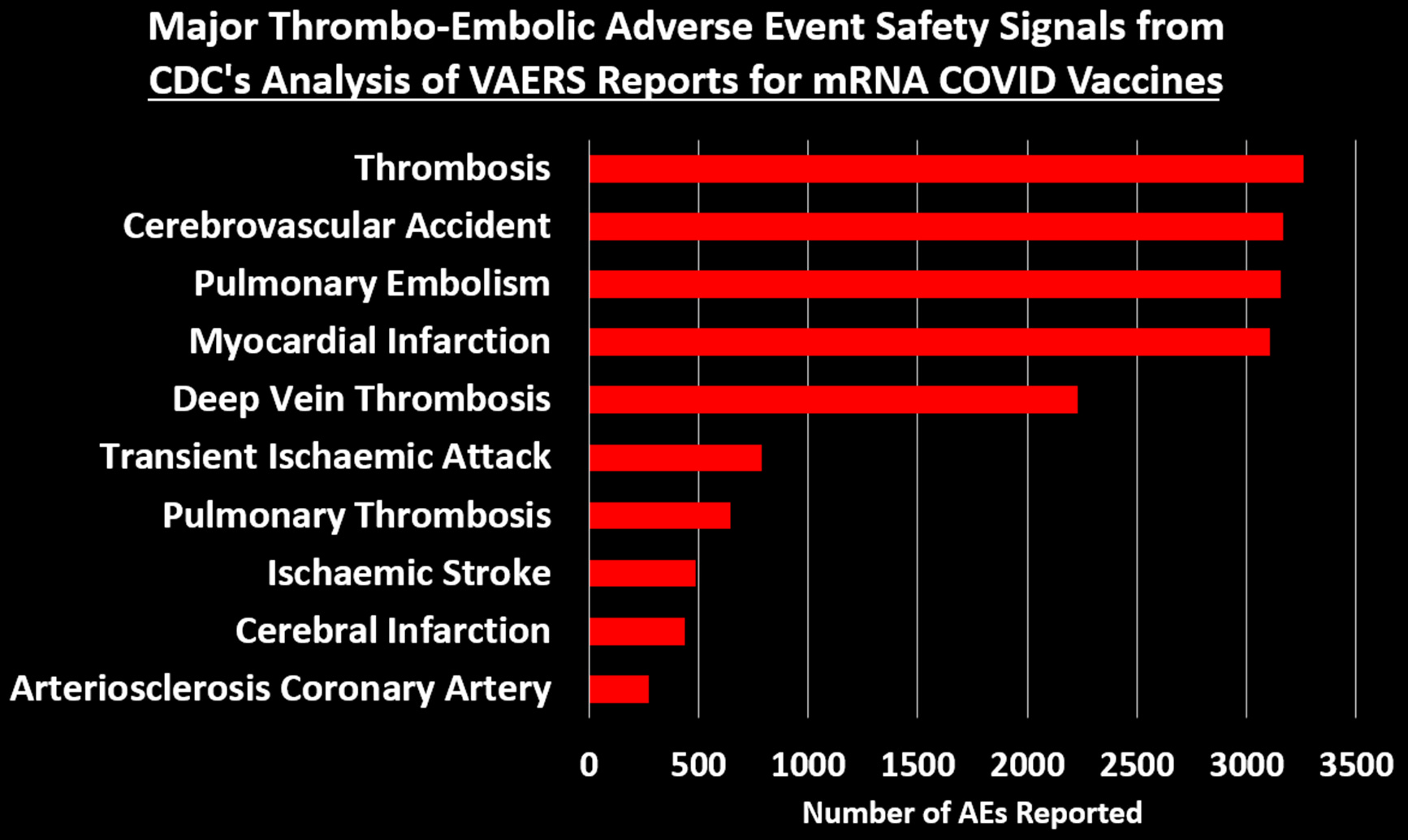
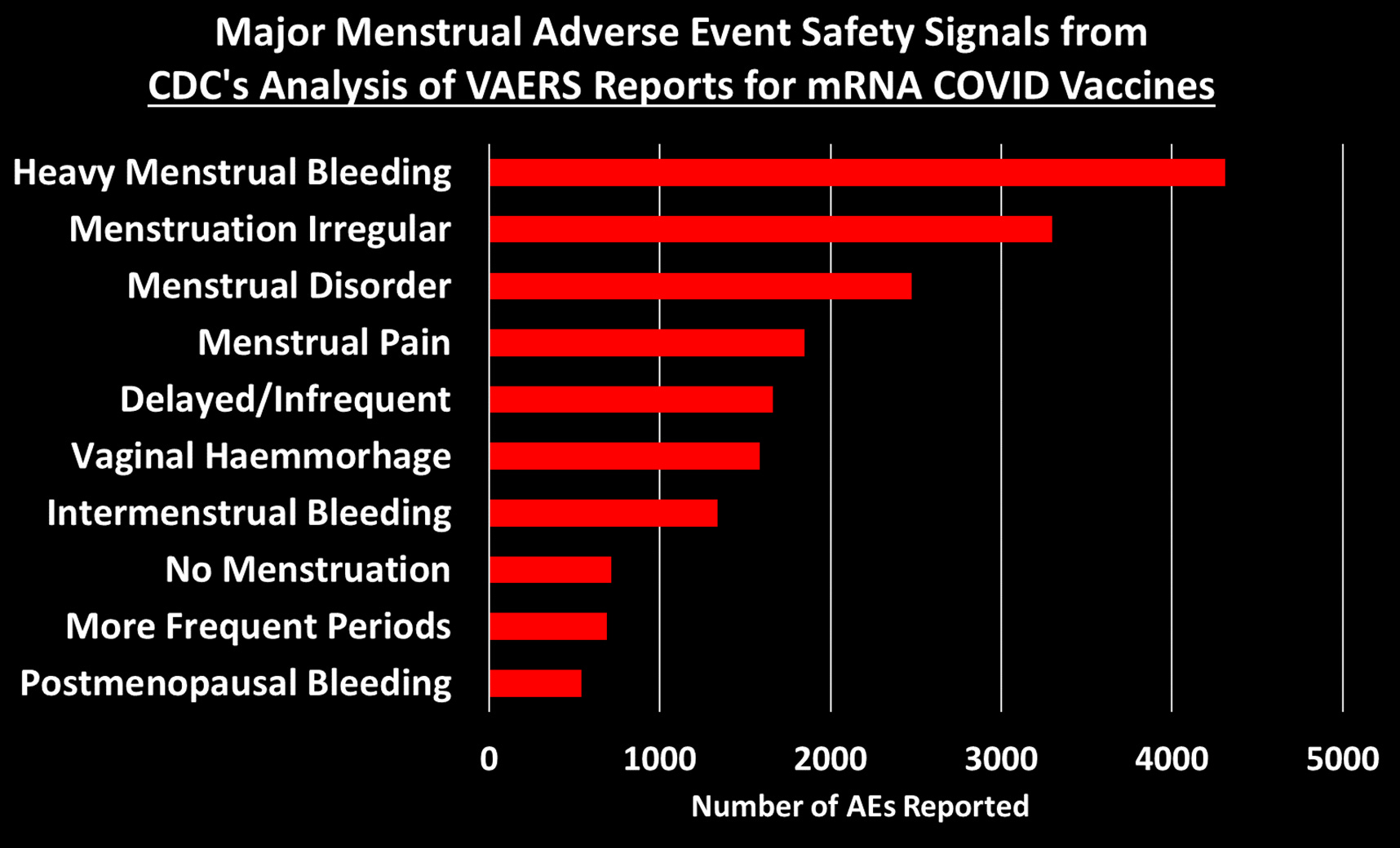
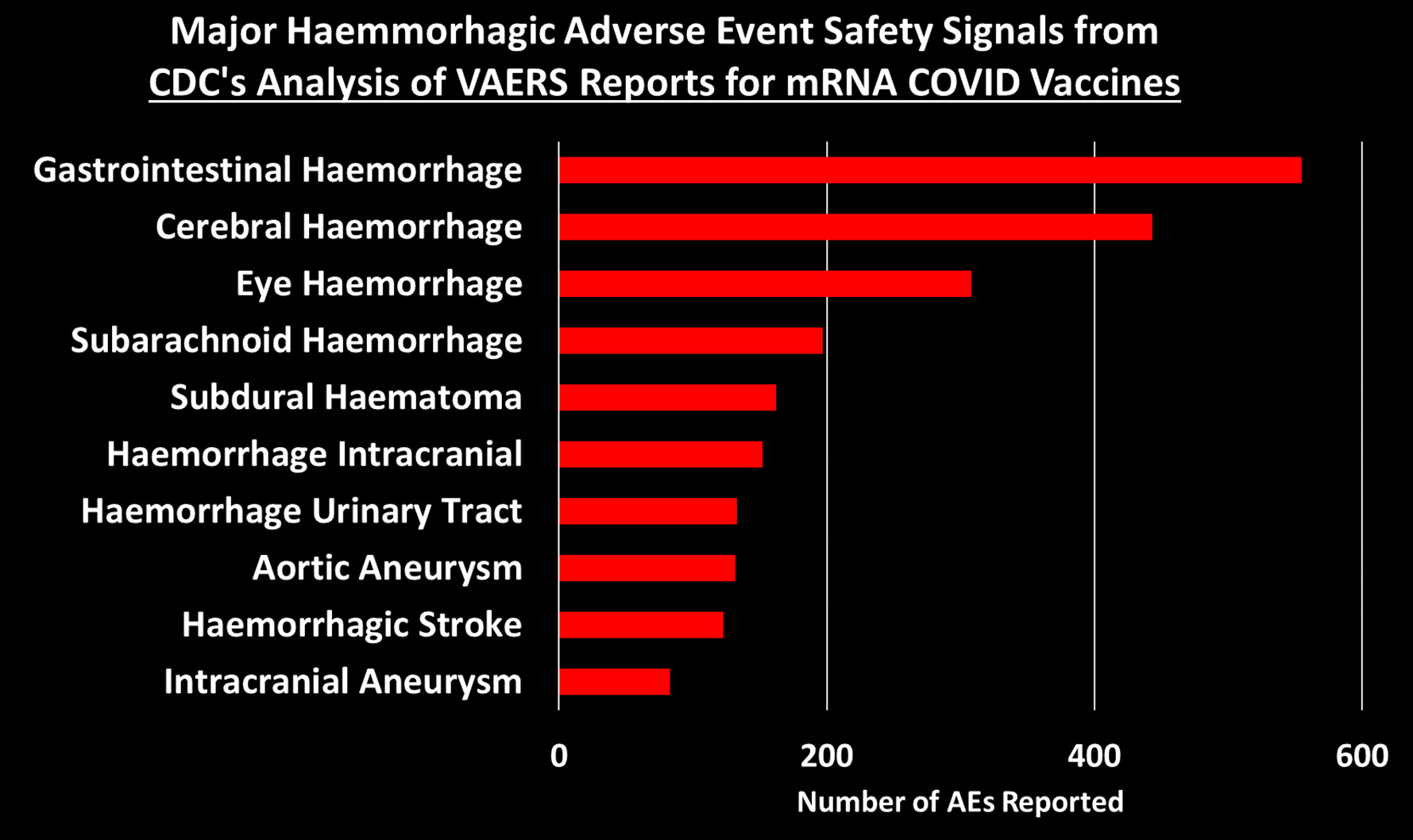
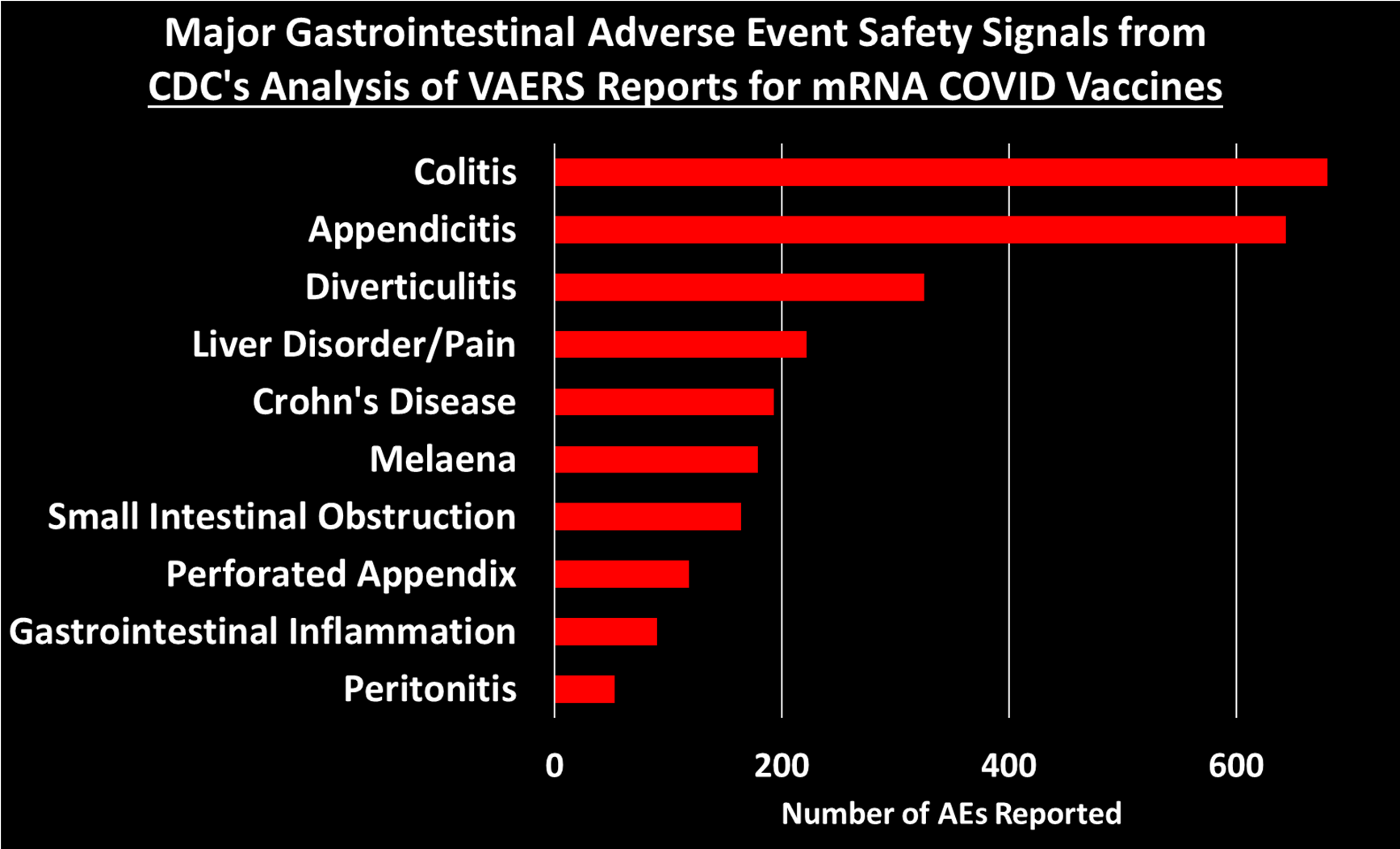
Before I begin, let me share a snapshot of the current 758 safety signals emerging from an analysis of the VAERS database, post COVID gene injection (this serious scholarship was done by Josh Guetzkow, Jackanapes Junction stack):
Deeper analysis into the cardiovascular signals:
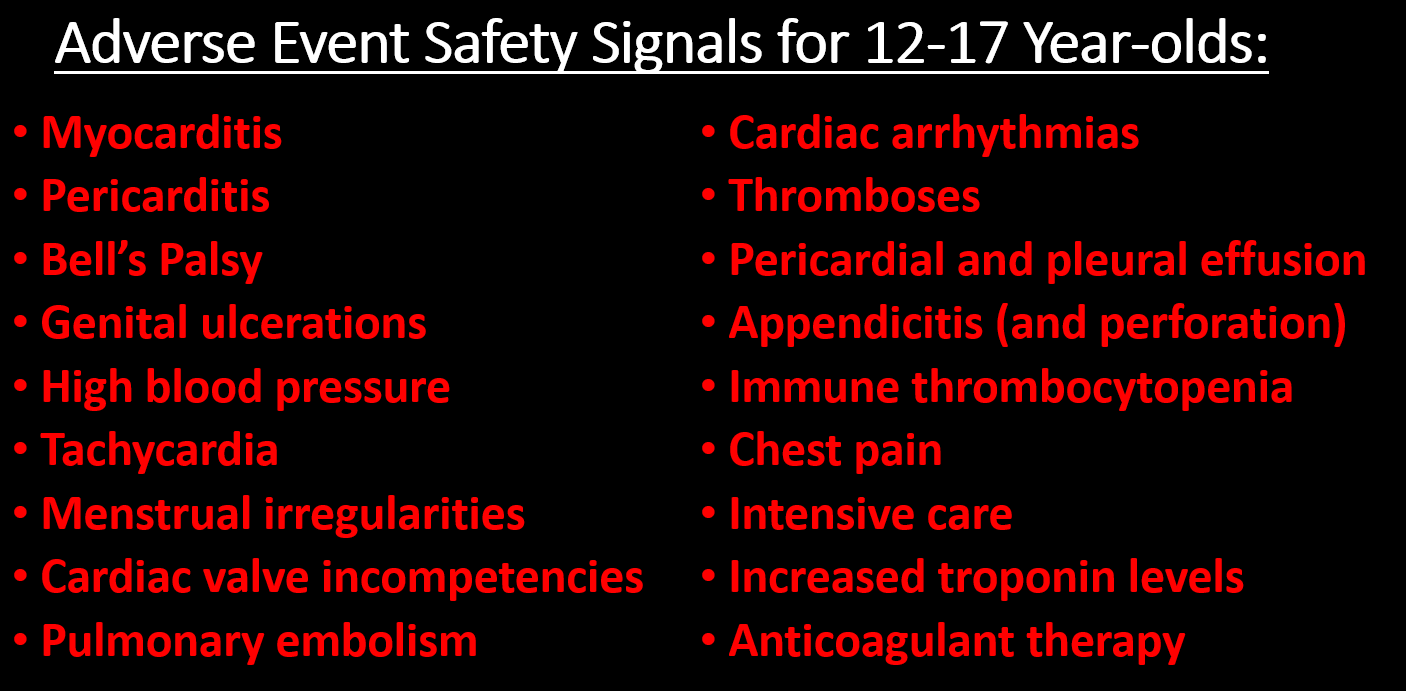
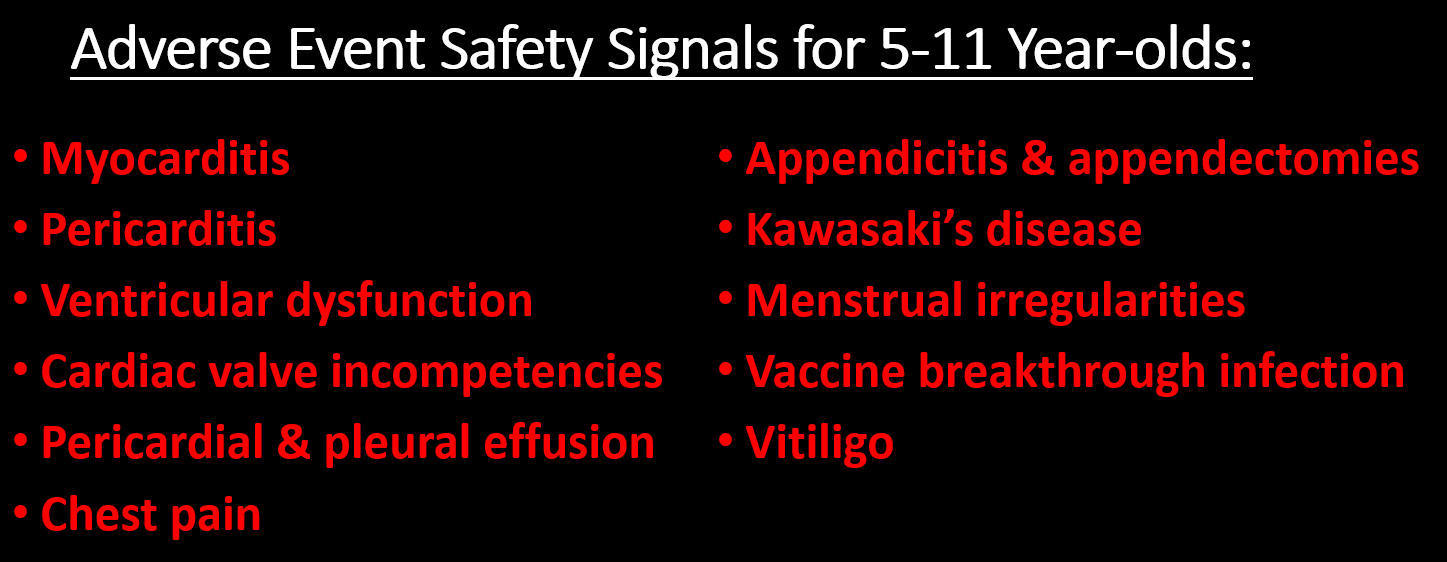
Jackanapes Junction even gives us good data on adverse events in children as compiled in the VAERS database:
‘There are 92 safety signals for 12-17 year-olds and 65 for 5-11 year-olds. Here are the most alarming ones:
Drs. Walensky and Califf, what about this recent NATURE study by Kwan et al. showing elevated 'Postural orthostatic tachycardia syndrome' (POTS) risk after COVID mRNA technology gene injection vaccine? Researchers found that in a cohort of near 300,000 COVID-vaccinated individuals, the odds of POTS are higher 3 months after vaccine exposure than 90 days before exposure; a possible association between COVID-19 vax & POTS. Myocarditis: OR 2.57, POTS: OR 1.52, UTI: OR 1.32, Hypertension: OR 1.23
SOURCE:
https://www.nature.com/articles/s44161-022-00177-8?utm_source=substack&utm_medium=email

Have you Drs. Walensky and Califf had time to read the shocking study report by Dr. James Thorp et al. whereby he found that the COVID-19 gene-based inoculations produce a 57-fold increase in miscarriages, a 38-fold increase in still birth rates, and a 1200-fold increase in menstrual abnormalities?
Key conclusion is that: ‘Pregnancy complications and menstrual abnormalities are significantly more frequent following COVID-19 vaccinations than Influenza vaccinations. A worldwide moratorium on the use of COVID-19 vaccines in pregnancy is advised until randomized prospective trials document safety in pregnancy and long-term follow-up in offspring.’
Dr. Thorp found that the COVID gene injections were associated with a significant ‘increase in AE with all proportional reporting ratios of > 2.0: menstrual abnormalities, miscarriage, fetal chromosomal abnormalities, fetal malformation, fetal cystic hygroma, fetal cardiac disorders, fetal arrhythmias, fetal cardiac arrest, fetal vascular mal-perfusion, fetal growth abnormalities, fetal abnormal surveillance, fetal placental thrombosis, low amniotic fluid, preeclampsia, premature delivery, preterm premature rupture of membrane, fetal death/stillbirth, and premature baby death (all p values were much smaller than 0.05).’

SOURCE:
https://www.preprints.org/manuscript/202209.0430/v2
What about this recent publication by structural biologist Panagis Polykretis and board-certified internist and cardiologist Dr. Peter McCullough, finding that over 270 athletes & former American athletes have died from cardiac arrests & serious issues from taking 'mRNA technology' based COVID-19 gene vaccines? Did you read this report, Drs. Walensky and Califf?

The global data also showed that between 2021 to 2022, former and current American athletes made up 279 of the mortalities.
SOURCE:
https://onlinelibrary.wiley.com/doi/full/10.1111/sji.13242
I have another study to interest you both in. Have you read this study in CIRCULATION by Yonker et al. where researchers found free spike antigen in the blood of adolescents and young adults who developed post-mRNA vaccine myocarditis? Did you spend any time thinking about the implications of the free spike protein and what these researchers found as to myocarditis?
SOURCE:
https://www.ahajournals.org/doi/10.1161/CIRCULATIONAHA.122.061025
How about this study Drs. Walensky and Califf? The lead author was Øystein Karlstad and they looked at 23 million population in the 4 Nordic nations of Denmark, Finland, Norway, and Sweden. Did you happen to read these findings? Allow me to also include them here:
SOURCE:
https://jamanetwork.com/journals/jamacardiology/fullarticle/2791253
‘Among 23, 122, 522 Nordic residents (81% vaccinated by study end; 50.2% female), 1077 incident myocarditis events and 1149 incident pericarditis events were identified. Within the 28-day period, for males and females 12 years or older combined who received a homologous schedule, the second dose was associated with higher risk of myocarditis, with adjusted IRRs of 1.75 (95% CI, 1.43-2.14) for BNT162b2 and 6.57 (95% CI, 4.64-9.28) for mRNA-1273. Among males 16 to 24 years of age, adjusted IRRs were 5.31 (95% CI, 3.68-7.68) for a second dose of BNT162b2 and 13.83 (95% CI, 8.08-23.68) for a second dose of mRNA-1273, and numbers of excess events were 5.55 (95% CI, 3.70-7.39) events per 100 000 vaccinees after the second dose of BNT162b2 and 18.39 (9.05-27.72) events per 100 000 vaccinees after the second dose of mRNA-1273.’ Estimates for pericarditis were similar.
I bold the conclusion for you:
Results of this large cohort study indicated that both first and second doses of mRNA vaccines were associated with increased risk of myocarditis and pericarditis. For individuals receiving 2 doses of the same vaccine, risk of myocarditis was highest among young males (aged 16-24 years) after the second dose.’
The hard reality is that these COVID mRNA technology gene injections have never ever been proven safe and effective. Never. Stating it does not make it so. Moreover, in your capacity at CDC and FDA, you Drs. Walensky and Califf are constrained from making a statement on safety and effectiveness (efficacy) given no such study exists and has proven this, and also these studies remain investigational and the COVID gene injections remain under EUA. You are not allowed to make that claim if I recall correctly, even as per FDA’s own rules.
Again, as I wrote this response, there exists no study, no clinical study, no randomized controlled trial, none, that shows these vaccine are safe or effective. The legacy trials by Pfizer and Moderna were fraudulent, the methodology was poor and sub-optimal with many questions that suggest fraud in the data provided and analysis, and were stopped early for benefit which is a clear flag for high risk of biased estimates of effect. Giving the vaccine to the placebo group essentially doomed the studies and stopped them as there no longer was a comparative effectiveness research group. None. The studies were over.
As an example, there is no proper accounting of 3,000 subjects that were removed from the study/analysis (1,500 per arm in Pfizer as an example) and when we back calculate and re-impute, the relative risk reduction of 95% drops to 20% and does not meet the 50% threshold. There is substantial baseline imbalance and the use of the relative risk reduction was an attempt to defraud the public for the absolute risk benefit was 0.7% and 1.1% respectively. When you consider the toxicity, the burden, the costs and harms, then a well-informed potential vaccinee may well have rejected the shot given the very modest near non-existent 0.7% absolute risk reduction relative to the harms. Persons would have likely chosen to place more value on avoiding the harms in lieu of a modest benefit for a vaccine that was not studied for the proper duration to conclusively ‘exclude’ harms. It is not that it was ‘not completely safe’. It is that it is not and was never safe and no amount of further follow up would have made an unsafe vaccine then become ‘safe’. The mRNA technology and the lipid-nano particle platform were unsafe to begin wit hand known to be unsafe and should have never ever been given to the public. This IMO was criminal by all involved.
To this day, we have not had the proper robust comparative effectiveness research using large randomized controlled trials (placebo) (RCTs) that run to sample size, that are not stopped for benefit, that have trustworthy randomization sequence generation, allocation concealment, blinging, trial arm/group baseline balance, limited attrition and balanced attrition, clear of rampant conflicts of interest, and which utilize the proper patient important outcomes for informed decision-making. Antibody (humoral) titer levels (and elevated titers) are not a measure of immunity (given we are more concerned about infections, hospitalizations, ICU, and deaths as well as cellular memory T and B-cell immunity) along with the corrupted methods of immuno-bridging etc.
This is corrupted ‘made-up’ voodoo science that the vaccine makers are engaging in and the FDA is approving. Instead, we are barraged by very sub-optimal corrupted short duration (often a few weeks) observational studies using antibody titers as the primary outcome measure and these are often of short duration (unable to detect safety signals) and plagued by selection bias and confounding (distorting the interpretation) with very shoddy statistical adjustment techniques without the control for key known and unknown factors, and particularly co-morbidities, natural exposure immunity, early treatment, and health vaccinee effect bias, as well as improvements in healthcare across the pandemic etc. The observational studies within this vaccine research era have been plagued with residual confounding bias that would even persist after adjusting for several individual-level and community-level risk factors.
Where is the proper research studies? Where are the RCTs in children? The CDC and FDA continue to claim there is ‘the clear benefit of COVID-19 vaccines in preventing death, serious illness, and hospitalization from SARS-CoV-2 infection’. So I ask, please Drs. Walensky and Califf, can you point us to the studies and evidence you are referring to for we could not find it?
I now point Drs. Walensky and Califf to the most recent research publication from Dr. John Ioannidis of Stanford who has after near 3 years, produced the same estimates he did early in 2020, basically showing the very near zero risk of severe outcome or death in the population, save for the elderly (often with underlying medical conditions). Did Drs. Walensky and Califf know of this research?
‘In people younger than 70 years, infection fatality rates ranged from 0.00% to 0.31% with crude and corrected medians of 0.05%. The infection fatality rate of COVID-19 can vary substantially across different locations and this may reflect differences in population age structure and case-mix of infected and deceased patients and other factors. The inferred infection fatality rates tended to be much lower than estimates made earlier in the pandemic.’
SOURCE:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7947934/pdf/BLT.20.265892.pdf/
What about this new publication (updated) by Dr. Ioannidis? Did you take the time to visit these IFR estimates, Drs. Walensky and Califf? He focused on the age-stratified infection fatality rate of COVID in the non-elderly, informed from pre-vaccination national seroprevalence studies. He showed the following:
‘For 29 countries (24 high-income, 5 others), publicly available age-stratified COVID-19 death data and age-stratified seroprevalence information were available and were included in the primary analysis. The IFRs had a median of 0.035% (interquartile range (IQR) 0.013 - 0.056%) for the 0-59 years old population, and 0.095% (IQR 0.036 - 0.125%,) for the 0-69 years old. The median IFR was 0.0003% at 0-19 years, 0.003% at 20-29 years, 0.011% at 30-39 years, 0.035% at 40-49 years, 0.129% at 50-59 years, and 0.501% at 60-69 years. Including data from another 9 countries with imputed age distribution of COVID-19 deaths yielded median IFR of 0.025-0.032% for 0-59 years and 0.063-0.082% for 0-69 years. Meta-regression analyses also suggested global IFR of 0.03% and 0.07%, respectively in these age groups.’
SOURCE:
https://www.medrxiv.org/content/10.1101/2022.10.11.22280963v1
Drs. Walensky and Califf also mentioned the waning of vaccine immunity. Can they point to any study, just one, showing that the COVID mRNA gene injections stop infection or transmission. They cannot. I could find none and we know that most all persons who are vaccinated have gotten re-infected. I think even you Dr. Walensky with your 22 shots. So you are being disingenuous and misleading the public as you tried to discredit Dr. Ladapo’s urgent letter to you. You know full well these COVID injections are non-neutralizing and do not sterilize the virus. They do not stop infection, replication, or transmission. You know they place the target antigen (spike and it’s epitope binding sites) under sub-optimal selective pressure that is driving infectious variant after infectious variant to emerge (with a potentially virulent one). Yet you seem to pretend for in my estimation, if you continue these gene shots, then the infectious variants (increasingly more infectious) will never stop emerging. There is a risk now that this can go on for years even and the vaccinated person is now on a booster treadmill they cannot get off of for their immune systems are now subverted. The vaccinated person is getting re-infected and becoming severely ill and there are reported deaths.
May I Drs. Walensky and Califf, provide you with some study examples that I hoped you would have read but alas, I realize you simply do not read the science or cannot understand it. I will embed the links for you and you have a go at it and if you do not understand, please reach out to me and I will surely school you on what these studies show. En toto though, Writ Large, these shared studies show that the COVID gene injections did fail, have fail, will fail and never worked and there is sheer negative effectiveness and harms. You are free to ensure your respective staffs know of these so that they too can stop making themselves look so idiotic in public:
Key link here to a major review I wrote:
https://brownstone.org/articles/16-studies-on-vaccine-efficacy/
Some selected individual studies for you to enjoy:
Rate of SARS-CoV-2 Reinfection During an Omicron Wave in Iceland, Eythorsson, 2022“11 536 PCR-positive persons were included. The mean (SD) age was 34 (19) years (median, 31 years; range, 0-102 years), 5888 (51%) were male, 2942 (25.5%) had received at least 1 dose of vaccine, and the mean (SD) time from initial infection was 287 (191) days (median, 227 days; range, 60-642 days); The probability of reinfection increased with time from the initial infection (odds ratio of 18 months vs 3 months, 1.56; 95% CI, 1.18-2.08) (Figure) and was higher among persons who had received 2 or more doses compared with 1 dose or less of vaccine (odds ratio, 1.42; 95% CI, 1.13-1.78)”
Effectiveness of mRNA-1273 against infection and COVID-19 hospitalization with SARSCoV-2 Omicron subvariants: BA.1, BA.2, BA.2.12.1, BA.4, and BA.5, Tseng, 2022“While 3-dose VE against BA.1 infection was high and waned slowly, VE against BA.2, BA.2.12.1, BA.4, and BA.5 infection was initially moderate to high (61.0%-90.6% 14-30 days post third dose) and waned rapidly. The 4-dose VE against infection with BA.2, BA.2.12.1, and BA.4 ranged between 64.3%-75.7%, and was low (30.8%) against BA.5 14-30 days post fourth dose, disappearing beyond 90 days for all subvariants.”
Effectiveness of COVID-19 Vaccines Over 13 Months Covering the Period of the Emergence of the Omicron Variant in the Swedish Population, Yu, 2022“Two vaccine doses showed long-lasting good protection against infection before Omicron (VE were above 85% for all time intervals), but less protection against Omicron infection (dropped to 43% by week four and no protection by week 14). Similarly, VE against hospitalization was high and stable before Omicron, but showed clear waning during the Omicron period, although VE estimates were substantially higher (above 80% to week 25, dropping to 40% by week 40) than against infection.”
Long-term COVID-19 booster effectiveness by infection history and clinical vulnerability and immune imprinting, Chemaitelly, 2022“Booster effectiveness relative to primary series was 41.1% (95% CI: 40.0-42.1%) against infection and 80.5% (95% CI: 55.7-91.4%) against severe, critical, or fatal COVID-19, over one-year follow-up after the booster. Among persons clinically vulnerable to severe COVID-19, effectiveness was 49.7% (95% CI: 47.8-51.6%) against infection and 84.2% (95% CI: 58.8-93.9%) against severe, critical, or fatal COVID-19. Effectiveness against infection was highest at 57.1% (95% CI: 55.9-58.3%) in the first month after the booster but waned thereafter and was modest at only 14.4% (95% CI: 7.3-20.9%) by the sixth month. In the seventh month and thereafter, coincident with BA.4/BA.5 and BA.2.75* subvariant incidence, effectiveness was progressively negative reaching -20.3% (95% CI: -55.0-29.0%) after one year of follow-up. Similar levels and patterns of protection were observed irrespective of prior infection status, clinical vulnerability, or type of vaccine (BNT162b2 versus mRNA-1273).”
Alarming antibody evasion properties of rising SARS-CoV-2 BQ and XBB subvariants, Wang, 2022“BQ.1, BQ.1.1, XBB, and XBB.1 are the most resistant SARS-CoV-2 variants to date;
Serum neutralization was markedly reduced, including with the bivalent booster;
All clinical monoclonal antibodies were rendered inactive against these variants;
The ACE2 affinity of these variants were similar to their parental strains;
The BQ and XBB subvariants of SARS-CoV-2 Omicron are now rapidly expanding, possibly due to altered antibody evasion properties deriving from their additional spike mutations. Here, we report that neutralization of BQ.1, BQ.1.1, XBB, and XBB.1 by sera from vaccinees and infected persons was markedly impaired, including sera from individuals boosted with a WA1/BA.5 bivalent mRNA vaccine. Titers against BQ and XBB subvariants were lower by 13-81-fold and 66-155-fold, respectively, far beyond what had been observed to date. Monoclonal antibodies capable of neutralizing the original Omicron variant were largely inactive against these new subvariants, and the responsible individual spike mutations were identified. These subvariants were found to have similar ACE2-binding affinities as their predecessors. Together, our findings indicate that BQ and XBB subvariants present serious threats to current COVID-19 vaccines, render inactive all authorized antibodies, and may have gained dominance in the population because of their advantage in evading antibodies.”
Low neutralization of SARS-CoV-2 Omicron BA.2.75.2, BQ.1.1, and XBB.1 by parental mRNA vaccine or a BA.5-bivalent booster, Kurhade, 2022“The newly emerged SARS-CoV-2 Omicron sublineages, including the BA.2-derived BA.2.75.2 and the BA.5-derived BQ.1.1 and XBB.1, have accumulated additional spike mutations that may affect vaccine effectiveness. Here we report neutralizing activities of three human serum panels collected from individuals 23–94 days after dose 4 of a parental mRNA vaccine, 14–32 days after a BA.5-bivalent-booster from individuals with 2–4 previous doses of parental mRNA vaccine, or 15–32 days after a BA.5-bivalent-booster from individuals with previous SARS-CoV-2 infection and 2–4 doses of parental mRNA vaccine. The results showed that a BA.5-bivalent-booster elicited a high neutralizing titer against BA.4/5 measured at 14- to 32-day post-boost; however, the BA.5-bivalent-booster did not produce robust neutralization against the newly emerged BA.2.75.2, BQ.1.1, or XBB.1. Previous infection significantly enhanced the magnitude and breadth of BA.5-bivalent-booster-elicited neutralization. Our data support a vaccine update strategy that future boosters should match newly emerged circulating SARS-CoV-2 variants.”
Effectiveness of the Coronavirus Disease 2019 (COVID-19) Bivalent Vaccine, Shrestha, 2022 “A retrospective cohort study conducted at the Cleveland Clinic Health System (CCHS) in the United States.
Researchers included employees on the very day that the bivalent COVID-19 vaccine was first available.
‘Protection provided by vaccination (analyzed as a time-dependent covariate) was evaluated using Cox proportional hazards regression.’
Findings focused on 51,011 employees of which 20,689 (41%) had a prior documented COVID-19 infection (episode), and whereby 42,064 (83%) received at least two doses of the vaccine.
‘The majority of infections in Ohio were caused by the BA.4 or BA.5 lineages of the Omicron variant during the first 10 weeks of the study, based on SARS-CoV-2 variant monitoring data available from the Ohio Department of Health. By December, the BQ.1, BQ.1.1, and BF.7 lineages accounted for a substantial proportion of the infections.’
‘By the end of the study, 10804 (21%) were bivalent vaccine boosted. The bivalent vaccine was the Pfizer vaccine in 9595 (89%) and the Moderna vaccine in the remaining 1178. Altogether, 2452 employees (5%) acquired COVID-19 during the 13 weeks of the study.’
‘The calculated overall vaccine effectiveness from the model was 30% (95% C.I., 20% – 39%)…when the Omicron BA.4/BA.5 lineages were the predominant circulating strains.’
‘The multivariable analyses also found that, the more recent the last prior COVID-19 episode was the lower the risk of COVID-19, and that the greater the number of vaccine doses previously received the higher the risk of COVID-19.”
Effectiveness of second booster compared to first booster and protection conferred by previous SARS CoV-2 infection against symptomatic Omicron BA.2 and BA.4/5 in France, Tamandjou, 2023“We included symptomatic ≥60 years old individuals tested for SARSCoV-2 in March 21-October 30, 2022. Compared to a 181-210 days old first booster, a second booster restored protection with an effectiveness of 39% [95%CI: 38% – 41%], 7-30 days postvaccination This gain in protection was lower than the one observed with the first booster, at equal time points since vaccination.”
Extended SARS-CoV-2 RBD booster vaccination induces humoral and cellular immune tolerance in mice, Gao, 2023i) Our findings demonstrate potential risks with the continuous use of SARS-CoV-2 vaccine boosters, providing immediate implications for the global COVID-19 vaccination enhancement strategies.
ii) Whether such re-establishment of vaccine-induced immune response could be repeated by continued application of boosters is being questioned, yet largely unknown at present. Here, we compared the effects of repeated RBD vaccine boosters with a conventional immunization course to those with an extended vaccination strategy, in a Balb/c mice model.
iii) We found that the protective effects from the humoral immunity and cellular immunity established by the conventional immunization were both profoundly impaired during the extended vaccination course. Specifically, extended vaccination not only fully impaired the amount and the neutralizing efficacy of serum RBD-specific antibodies, but also shortened the long-term humoral memory.
iv) This is associated with immune tolerance in germinal center response, along with decreased numbers of spleen germinal center B and Tfh cells. Moreover, we demonstrated that extended immunization reduced the functional responses of CD4+ and CD8+T cells, restrained the population of memory T cells, and up-regulated the expression of PD-1 and LAG-3 in Te sub-type cells.
v) An increased percentile of Treg cells was also observed, accompanied by significant elevation of IL-10 production. Together, we provided crucial evidence that repetitive administration of RBD booster vaccines may negatively impact the immune response established by a conventional vaccination course and promote adaptive immune tolerance.’
vi) Continued vaccination promoted the formation of a prominent adaptive immune tolerance and profoundly impaired the established immune response with the conventional course, evidenced by significant reductions in antigen specific antibody and T cell response, a loss of immune memory and form of immunosuppression micro-environment.
Effect of prior infection, vaccination, and hybrid immunity against symptomatic BA.1 and BA.2 Omicron infections and severe COVID-19 in Qatar, Altarawneh, March 2022“Qatar researchers investigated SARS-CoV-2 Omicron symptomatic BA.1 infection, symptomatic BA.2 infection, BA.1 hospitalization and death, and BA.2 hospitalization and death, between December 23, 2021 and February 21, 2022. The researchers conducted 6 national, matched, test-negative case-control studies were conducted to examine effectiveness of BNT162b2 (Pfizer-BioNTech) vaccine, mRNA-1273 (Moderna) vaccine, natural immunity due to prior infection with pre-Omicron variants, and hybrid immunity from prior infection and vaccination. They found that “Effectiveness of only prior infection against symptomatic BA.2 infection was 46.1% (95% CI: 39.5-51.9%). Effectiveness of only two-dose BNT162b2 vaccination was negligible at -1.1% (95% CI: -7.1-4.6), but nearly all individuals had received their second dose several months earlier. Effectiveness of only three-dose BNT162b2 vaccination was 52.2% (95% CI: 48.1-55.9%). Effectiveness of hybrid immunity of prior infection and two-dose BNT162b2 vaccination was 55.1% (95% CI: 50.9-58.9%).” The key finding was “There are no discernable differences in the effects of prior infection, vaccination, and hybrid immunity against BA.1 versus BA.2.”
Effectiveness of a fourth dose of mRNA COVID-19 vaccine against all-cause mortality in long-term care facility residents and in the oldest old: A nationwide, retrospective cohort study in Sweden, Nordström, 2022“From 7 days after baseline and onwards, there were 1119 deaths in the LTCF cohort during a median follow-up of 77 days and a maximum follow-up of 126 days. During days 7 to 60, the VE of the fourth dose was 39% (95% CI, 29-48), which declined to 27% (95% CI, -2-48) during days 61 to 126. In the cohort of all individuals aged ≥80 years, there were 5753 deaths during a median follow-up of 73 days and a maximum follow-up of 143 days. During days 7 to 60, the VE of the fourth dose was 71% (95% CI, 69-72), which declined to 54% (95% CI, 48-60) during days 61 to 143.”
Risk of infection, hospitalisation, and death up to 9 months after a second dose of COVID-19 vaccine: a retrospective, total population cohort study in Sweden, Nordström, 2022“For the outcome SARS-CoV-2 infection of any severity, the vaccine effectiveness of BNT162b2 waned progressively over time, from 92% (95% CI 92 to 93; p<0·001) at 15-30 days, to 47% (39 to 55; p<0·001) at 121-180 days, and to 23% (-2 to 41; p=0·07) from day 211 onwards. Waning was slightly slower for mRNA-1273, with a vaccine effectiveness of 96% (94 to 97; p<0·001) at 15-30 days and 59% (18 to 79; p=0·012) from day 181 onwards. Waning was also slightly slower for heterologous ChAdOx1 nCoV-19 plus an mRNA vaccine, for which vaccine effectiveness was 89% (79 to 94; p<0·001) at 15-30 days and 66% (41 to 80; p<0·001) from day 121 onwards. By contrast, vaccine effectiveness for homologous ChAdOx1 nCoV-19 vaccine was 68% (52 to 79; p<0·001) at 15-30 days, with no detectable effectiveness from day 121 onwards (-19% [-98 to 28]; p=0·49). For the outcome of severe COVID-19, vaccine effectiveness waned from 89% (82 to 93; p<0·001) at 15-30 days to 64% (44 to 77; p<0·001) from day 121 onwards. Overall, there was some evidence for lower vaccine effectiveness in men than in women and in older individuals than in younger individuals.”
Neutralization against BA.2.75.2, BQ.1.1, and XBB from mRNA Bivalent Booster, Davis-Gardner, 2023“Used the FRNT in a VeroE6/TMPRSS2 cell line1 to compare the neutralizing activity in serum samples obtained from participants in three cohorts: the first cohort comprised 12 participants 7 to 28 days after one monovalent booster; the second, 11 participants 6 to 57 days after a second monovalent booster; and the third, 12 participants 16 to 42 days after a bivalent booster.
In all three cohorts, neutralization activity was lower against all omicron subvariants than against the WA1/2020 strain; neutralizing activity was lowest against the XBB subvariant (Figure 1 and Fig. S2). In the cohort that received one monovalent booster, the FRNT50 GMTs were 857 against WA1/2020, 60 against BA.1, 50 against BA.5, 23 against BA.2.75.2, 19 against BQ.1.1, and below the limit of detection against XBB. In the cohort that received two monovalent boosters, the FRNT50 GMTs were 2352 against WA1/2020, 408 against BA.1, 250 against BA.5, 98 against BA.2.75.2, 73 against BQ.1.1, and 37 against XBB. The results in both of these cohorts correspond with neutralization titers against BA.1 and BA.5 that were 5 to 9 times as low as that against WA1/2020 and neutralization titers against BA.2.75.2, BQ.1.1, and XBB that were 23 to 63 times as low as that against WA1/2020.”
Neutralization Escape by SARS-CoV-2 Omicron Subvariants BA.2.12.1, BA.4, and BA.5, Hachmann, 2022“Six months after the initial two BNT162b2 immunizations, the median neutralizing antibody pseudovirus titer was 124 against WA1/2020 but less than 20 against all the tested omicron subvariants. Two weeks after administration of the booster dose, the median neutralizing antibody titer increased substantially, to 5783 against the WA1/2020 isolate, 900 against the BA.1 subvariant, 829 against the BA.2 subvariant, 410 against the BA.2.12.1 subvariant, and 275 against the BA.4 or BA.5 subvariant.
Among the participants with a history of Covid-19, the median neutralizing antibody titer was 11,050 against the WA1/2020 isolate, 1740 against the BA.1 subvariant, 1910 against the BA.2 subvariant, 1150 against the BA.2.12.1 subvariant, and 590 against the BA.4 or BA.5 subvariant.”
I wanted to show you Drs. Walensky and Califf, this very interesting graph emerging out of the recently published by Shrestha et al.:
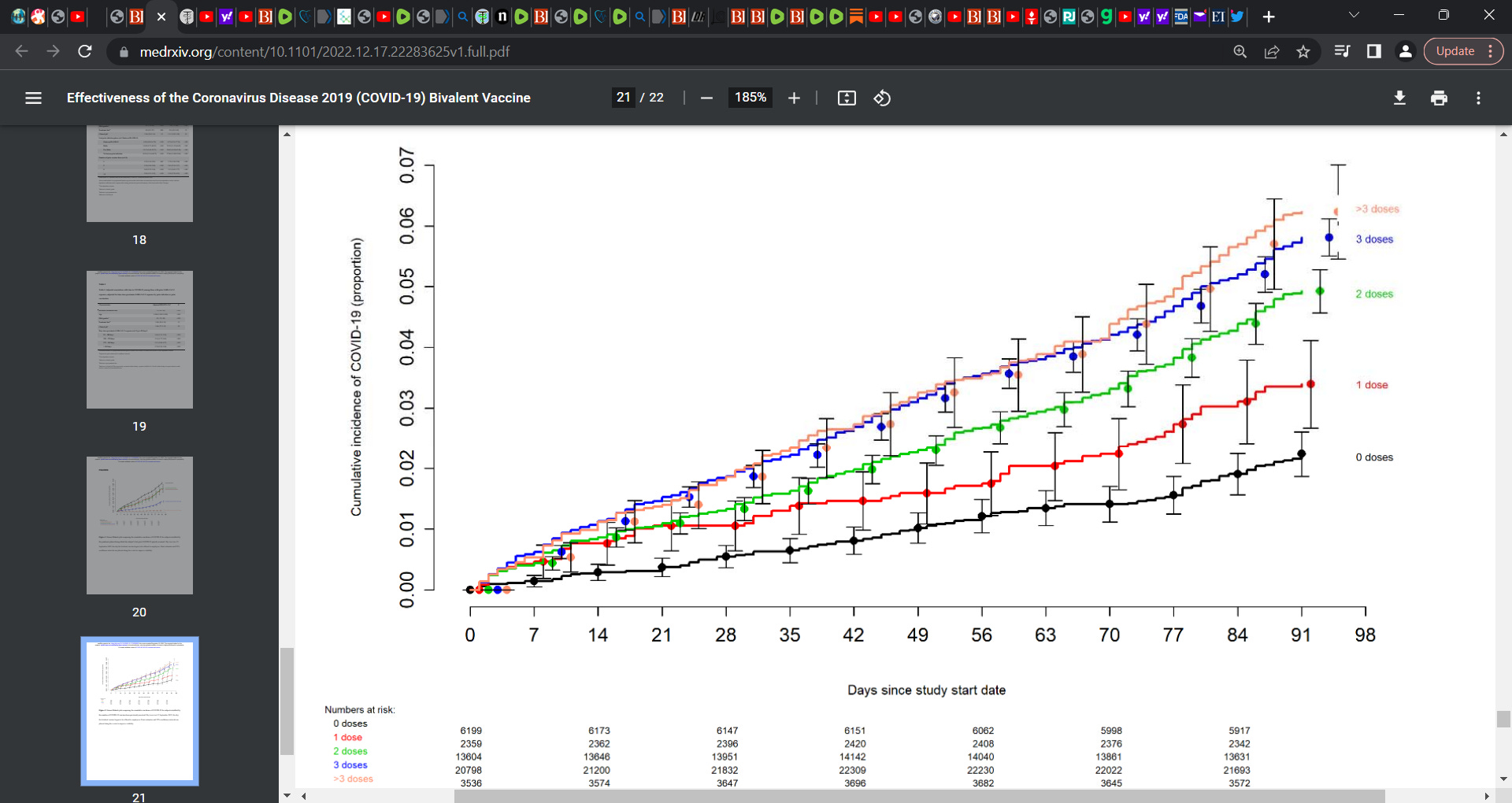
What do you see? Could you see the dose-response? That the more jabs you take, the more you are at risk of infection? Did you see that persons who remained unvaccinated had the lowest risk of COVID-19? That is, zero shots. When you get some time away form pulling fuzz balls from your navels, please take a look at this graph.
I also wanted to interest you in this important study by Constantin Schwab (German study) in case you may have missed it distracted by your navels; it is titled: Autopsy-based histopathological characterization of myocarditis after anti-SARS-CoV-2-vaccination
What is important to you two from this study, since you clearly have no grasp of the prevailing science is:
1)35 persons who died within 20 days post COVID gene injection (Germany)
2)autopsy findings and common characteristics of myocarditis in untreated persons who received COVID vaccination is presented with a focus on 25 persons who had died unexpectedly and within 20 days after COVID vaccination (mRNA platform).
3)All 25 (71%) had evidence of vaccine-induced sequelae e.g. cardiac arrest etc.
4)in four patients (16%), researchers identified acute (epi-)myocarditis without detection of another significant disease or health constellation that may have caused an unexpected death.
5)Histology showed patchy interstitial myocardial T-lymphocytic infiltration, predominantly of the CD4 positive subset, associated with mild myocyte damage. Overall, autopsy findings indicated death due to acute arrhythmogenic cardiac failure.
6)Conclusion by researchers: myocarditis can be a potentially lethal complication following mRNA-based COVID vaccination.
In the same light, I wanted to also interest you in this study by Mansanguan et al. titled: Cardiovascular Manifestation of the BNT162b2 (Pfizer) mRNA COVID-19 Vaccine in Adolescents, which looked at the sequelae in Thai adolescents post vaccine.
SOURCE:
https://pubmed.ncbi.nlm.nih.gov/36006288/
This prospective cohort study enrolled students aged 13-18 years from two schools, who received the second dose of the Pfizer mRNA COVID-19 vaccine. Researchers enrolled 314 participants; of these, 13 participants were lost to follow-up, leaving 301 participants for analysis. Researchers found that the most common cardiovascular signs and symptoms were tachycardia (7.64%), shortness of breath (6.64%), palpitation (4.32%), chest pain (4.32%), and hypertension (3.99%). One participant could have more than one sign and/or symptom. Seven participants (2.33%) exhibited at least one elevated cardiac biomarker or positive lab assessments.
It is important Drs. Welensky and Califf to understand that cardiovascular manifestations were found in 29.24% of patients, ranging from tachycardia or palpitation to myopericarditis. ‘Myopericarditis was confirmed in one patient after vaccination. Two patients had suspected pericarditis and four patients had suspected subclinical myocarditis.’
CDC & FDA’s statement to Dr. Ladapo:
ii)“Reports of adverse events to VAERS following vaccination do not mean that a vaccine caused the event. Since December 2020, almost 270 million people have received more than 670 million doses of COVID-19 vaccines in the U.S., with over 50 million people having received the updated bivalent vaccine.”
My response:
Firstly, CDC recommends everyone ages 6 months and older get vaccinated as soon as possible to protect against COVID-19 and its potentially severe complications. Yet, reports are that in October 2022, based on CDC’s own data, that as of August, 86% of children between 6 months and 17 years have had at least one COVID-19 infection, which is up from 75% in April of 2022. Estimates are that this is closer to 100% now. Then why would CDC at the same time be recommending everyone from 6 months and older to be vaccinated. This when CDC knows that healthy children bring a statistical zero risk of becoming severely ill or dying from COVID. So what is the scientific or medical basis?
This response above ii) is a non-sensical and outright specious and unscientific response by Drs. Walensky and Califf. These two know full well that CDC’s VAERS database is limited by the completeness of reporting and that the best estimate is that it captures 10% of morbidity and mortality. Many argue just 1%. Thus we are at present potentially looking at hundreds of thousands of deaths due to the COVID gene injection if only 10% is currently captured and millions of averse effects and many very serious at that.
Moreover, I do appreciate that an association does not mean ‘causation’ and that other factors may be the causative factor. Yet if we went just by the Sir Austin Bradford Hill’s criteria moving from observation to causation (strength, consistency, specificity, temporality, biological gradient, plausibility, coherence, experiment, and analogy), we find that the criteria are met that would more closely link the adverse events in VAERS to the COVID gene injection. It is clear that causality has been met and moreover, I have embedded a study above by Schwab et al. titled Autopsy-based histopathological characterization of myocarditis after anti-SARS-CoV-2-vaccination whereby researchers show that 71% of the deaths (in the initial cohort of 35) have some form of vaccine involvement.
CDC & FDA’s statement to Dr. Ladapo:
iii)“The Emergency Use Authorizations (EUAs) for the COVID-19 Vaccines require sponsors and vaccine providers to report certain adverse events through VAERS, so more reports should be expected. Recent concerns about increased reports of cardiovascular events provide an instructive example of the need to do further analysis when increased reporting of an event occurs. Despite increased reports of these events, when the concern was examined in detail by cardiovascular experts, the risk of stroke and heart attack was actually lower in people who had been vaccinated, not higher.”
My response:
Firstly the CDC referred to a non-randomized study by Jiang et al. plagued by unmeasured confounding variables and selection bias.
The CDC knows that the VAERS system captures only a very small fraction of the adverse events and deaths post vaccine. It is their system and they know how limited and corrupted it is. It has been useful as a sentinel system but something is not making sense for when we as outside scientists query the database and do our own analyses, we get numbers orders of magnitude greater than what the CDC is reporting. The key questions is who is doing the analysis for CDC? It is very easy for a biased and conflicted career technocrat doctor doing the review on behalf of the CDC that controls their salary and career, to provide misleading and actually false reviews. Are doctors doing these reviews and assessment being bought off? Their technocrat career and academic/research jobs dangled in front of them if they told the truth? I have no problem saying this and I am convinced this is what occurs.
Importantly, the CDC and FDA etc. have not implemented the proper and needed testing to assess if the vaccine is linked to the deaths, a robust adverse event surveillance given the sub-optimal performance of VAERS, data safety monitoring boards, adverse event monitoring boards etc. for these COVID gene injections. Where are the safety reports? Where are the adverse event reports for the public and oversight people to look at for independent assessment, especially on what was the actual cause of death. We need autopsies to be done and they are not being done. Denied. Why? Thus as of this writing, the data and situation analysis as to the true adverse event and death number indicates that is is false. Not accurate and the public is being misled.
Letters of interest that are the background for this substack (Ladapo, Walensky and Califf):
i)Dr. Ladapo’s letter dated February 15th 2023 to Drs. Walensky & Califf:
SOURCE:
ii) CDC & FDA’s letter to Dr. Joe Ladapo dated March 10th 2023:
SOURCE:
https://www.fda.gov/media/166159/download?utm_source=substack&utm_medium=email
One of your more comprehensive and forceful pieces. Thanks!
This is a very good stack Dr. Alexander. Unfortunately, Walensky and her ilk are impervious to reason and there's a reason for that.
Most of them have Hitler's personality disorder, Obsessive Compulsive Personality Disorder (OCPD; Anakastic Personality Disorder), and in particular the OCPD subtype that Theodore Millon, originator of the American Psychiatric Association's Diagnostic and Statistical Manual of Mental Disorders' personality disorders classification termed "bureaucratic compulsive with narcissistic features." This is the disorder that has driven the bureaucratic incompetence. Understanding it is key to defeating it.
I noted about it previously as follows:
What I think we are up against is OCPD. It's a big part of the reason for the bureaupathology of the vaccine advocates: Obsessive Compulsive Personality Disorder (OCPD), which is common in the military, where those with the condition tend to be rapidly promoted (e.g., Colonel Russell Williams, convicted serial killer and former Commanding Officer of Canada's largest airforce base), law enforcement (e. g., murderer of George Floyd, Derek Chauvin, Idaho killings suspect Bryan Kohberger), academia and serial killers appears also to be common in public health bureaucrats.
OCPD is a disorder of overcontrol. When dialled up, it's similar to psychopathy, with which it is often comorbid. It's characterised by, among other things, self-righteousness, tyrannical or dictatorial tendencies, perfectionism (especially WRT expectations of others), neatness ("serial killer neat"), punctuality, the ability to dial down or turn off empathy, perspective shifting deficits, rigidity, overconscientious and enjoyment of creating fear in subordinates. It has links to sadism, especially "enforcing sadism with compulsive features," "tyrannical sadism" mooand "spineless sadism."
People with the condition are functionally rigid, stubborn and tend to think they are "always right" and that there is only one correct way of doing things, which is their way. Hitler and Ghandi are good examples. They are angered when they don't get their own way and are overconcerned with ethics and morality. (Hitler was vegetarian and Bryan Kohberger is vegan.)
OCPD individuals are annoyed when proven to be wrong and they double down on their mistakes. Because of their perspective shifting deficits they have trouble with alternative hypothesis generation and are unsuited to be scientists. They are also unsuited for management roles and unsuited to be public health bureaucrats although, due to attention to detail, can make good accountants. A big part of their problem is their perspective taking deficits and cognitive distortions and fallacies in their reasoning. They can do well on tasks requiring attention to detail but they can't readily adjust their perspective to identify and correct for weaknesses in theory or methodology.
They tend to rise to the top in ethics councils, professional associations, regulatory bodies and the military as well as, it appears, the public health bureaucracy. Present them with evidence of vaccine harms and individuals with OCPD can't adjust their perspective or admit their mistakes and instead they just double down, and then seek revenge. Because it's an egosyntonic disorder they have no idea of how fucked up they are and how much harm they cause.
To further understand OCPD, consider the following description of Anthony Fauci by Scott Sturman M.D:
"The mindset of Field Marshal Douglas Haig, World War I’s worst general, springs to mind, when drawing a comparison to Anthony Fauci. By some historical accounts Field Marshal Sir Douglas Haig bears the distinction of WWI’s worst general. He rose to Commander of British Expeditionary Forces and led Allied armies during the slaughter and futility at the battles of the Somme and Passchendaele.
Known for his self confidence and inflexibility, he repeatedly ordered soldiers over the top to “no man’s land” and into the path of German machine guns. No number of casualties or unachieved objectives could dissuade him from his singular approach to combat. Nigel Davies, historian and educator, points out that General Haig was emblematic of the chateau general - dictating and directing but far removed from the battlefield: They were Chateau Generals in approach and in attitude.
They drew lines on maps without adequately considering the terrain, issued impossible instructions without looking at the state of the ground, and ran completely inadequate communications that were far from capable of keeping track of, or controlling, a modern battlefield.
In a similar respect, despite his academic and professional accomplishments, Dr. Anthony Fauci has no background or experience in clinical medicine and is ill equipped to lead the SARS-CoV-2 response. His purview is that of a research scientist and entrenched bureaucrat, who is far removed from patient contact. His career is enmeshed with the pharmaceutical industry, whose financial ties with federal medical regulatory institutions are well described.
Throughout his career he has denied patients easily accessible, inexpensive, and effective treatments in lieu of patented medications with high risk profiles and of dubious efficacy. In 1987 despite overwhelming clinical evidence, he told AIDS activists that the prophylactic use of the common antibiotic Bactrim to treat pneumocystis carnii pneumonia was ineffective and possibly dangerous. Through private donations the company Lymphomed circumvented the NIAID and conducted successful clinical trials.
The delay cost the lives of nearly 17,000 immunocompromised patients.