

'Dr. Yeadon Comments on 'Eleven Serious Problems with the New York City Spring 2020 Mass Casualty Event' by Jessica Hockett' (see Hockett's substack below); "Why is this important? No pandemic in NYC,
no worldwide scary event & no justification for the extraordinary measures imposed, echoes of which continue today." Eleven Serious Problems with the New York City Spring 2020 Mass Casualty Event

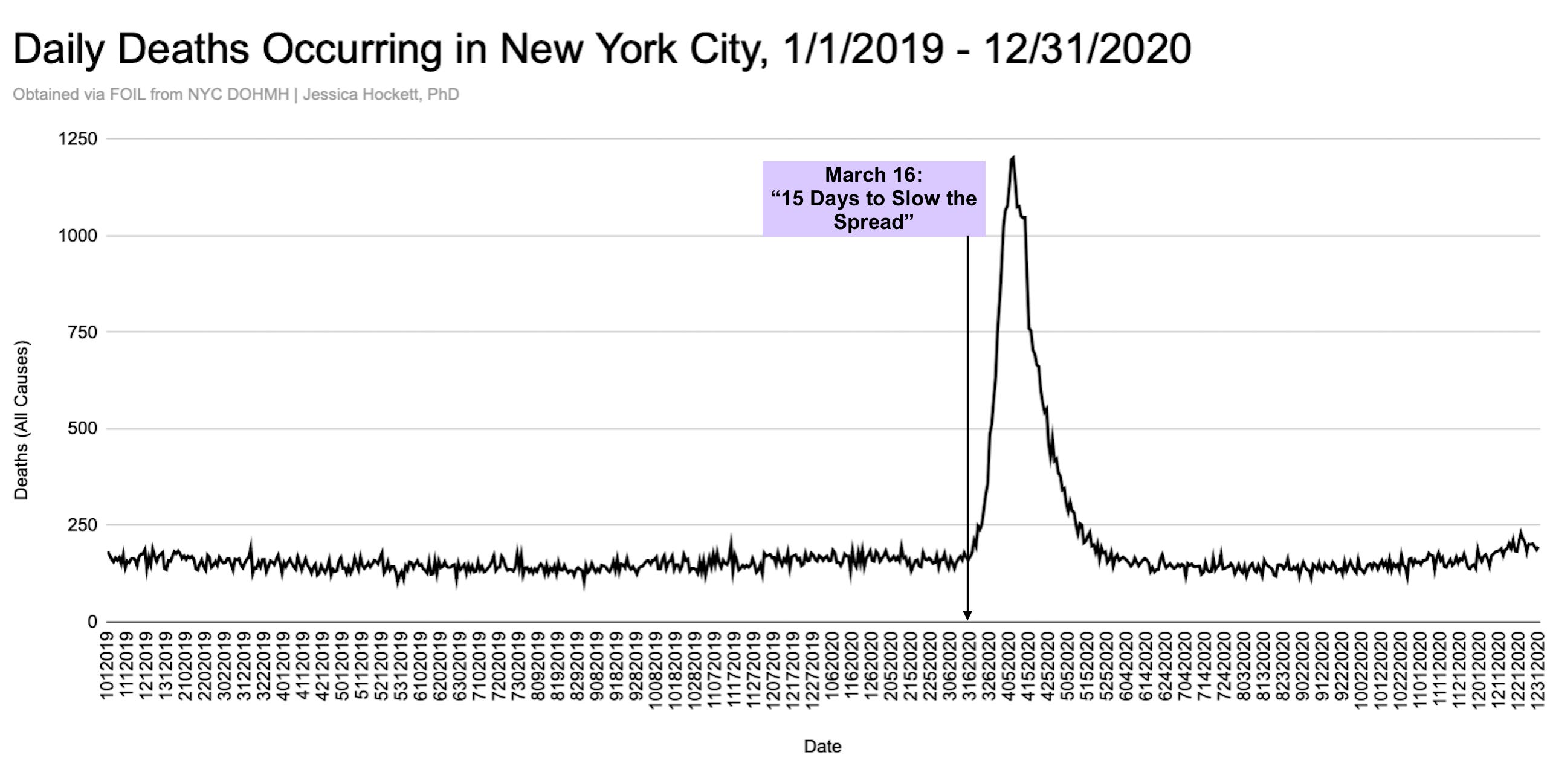
Notice that the spike in deaths only happened when we shut down…March 16th 2020…not before…and so, why?
We continue to argue that deaths occurred, most due to the devastating medical management, response…near 100%. Collateral effects of lockdowns, denial of treatment due to locked off ‘COVID’ beds, the Malone et al. mRNA vaccine, and mostly, the medical system death protocol response (isolation, DNR orders, no antibiotics, sedatives e.g. ketamine, propofol, midazolam etc., Remdesivir (kidney liver toxic), ventilator.
By Dr. Mike Yeadon September 29, 2024
No one can read this excellent summary from Jessica Hockett on the huge pulse in deaths reported to have occurred in NYC during the early stages of the faked “pandemic” and not easily recognize that there are major problems with the narrative and the claims.
Why is this important? No pandemic in NYC, no worldwide scary event & no justification for the extraordinary measures imposed, echoes of which continue today.
I haven’t studied this event, and my knowledge is limited to what Jessica has published over the years.
Her persistence and organization are admirable and appropriate & much appreciated by me and many others.
Read her 11 major problems with the data summary. Some are so ridiculous that you immediately know that they’re flat lies. Like 40% of all USA-wide home deaths associated with 91-divoc are reported to have occurred in NYC, which holds just 3% of the total population of USA. This is impossible.
There are many more such anomalies.
It’s certain that the event described on the nightly news & syndicated around the world 24/7 simply didn’t happen the way we’ve been told.
From separate work, in which I’ve had some involvement (eg from knowledge of pulmonology and pharmacotherapy of acute respiratory illnesses), we know for sure that large numbers of people were killed as a direct result of inappropriate medical “care”, during spring 2020. Furthermore, there were radically different medical procedures imposed in some countries than in others. In those countries in which aberrant changes in medical management of acute respiratory illnesses were not made, there were not excess deaths over expected until the intentionally toxic injections were rolled out.
Nowhere was there an increase in all causes mortality prior to the fraudulent declaration by WHO of a pandemic.
We’re only lied to. If there’s a major news story that is repeatedly reported & widely so, it’s a safe assumption that you’re being lied to in order to create a narrative in your mind, that is anticipated to “soften you up” to the next outrage and stripping of freedoms.
Once mass media got into the habit of lying completely, I think t unlikely to they tell the truth about anything.
For these reasons, I no longer consume any mainstream news media at all. I don’t systematically follow “news” excerpted by freedom activists, either.
There isn’t any true news. Perhaps there never had been.
Question everything you’re told, read & see.
Best wishes,
Mike
Hockett (support this seminal stack):
START HERE:
‘In the meantime, I categorically present some of the most serious data-related problems with the 27,000-death increase in eleven weeks. This event has not been reasonably explained or substantiated by the federal government and demands immediate attention from authorities and citizens.1
Each set of “problems” is framed as a question to allow for the possibility that I am wrong (or at least not 100% right).
1. No Signals?
There was no sign or signal of a spreading pathogen adding risk of severe illness or death in New York until the federal government announced “15 Days to Slow the Spread” and mass testing commenced. Why such a prevalent virus wasn’t manifesting itself in New York City mortality prior to national declarations remains unexplained. Raw data and a number of studies make clear that whatever was being identified via tests was widespread (and harmlessly so) before the purported emergency.2 The idea that officials had the prescience to time their emergency decrees with virus arrival is preposterous.
In theory, a spreading respiratory disease like “COVID” should first impact elderly infirm in settings where the most-vulnerable populations are present, and do so more gradually, but that’s not what we see in the New York data.3 Instead, there are simultaneous jumps in deaths across age groups and places of death, which makes little sense with infection fatality ratios for the disease.4
Not only testing and deaths, but nearly every time-series dataset of any kind I’ve reviewed in depth is unremarkable or within normal variation until mid-March. After that point, we see very sharp spikes or drops occur, as though someone pulled a trigger or commenced a drill.
It is extremely unlikely that natural and/or man-made incidents could generate the synchronicity and shapes observed across data of different kinds. The fact that no analysts or academics have been able to substantively and reasonably explain these and similar anomalies as the work of a novel coronavirus — and that few have even tried — is a testament to the implausible nature of the proposition.
2. (Almost) No Peers?
The speed and magnitude of the New York City event is almost peerless and is exceeded only by smaller and less population-dense provinces in Northern Italy, including Bergamo. Madrid, London, and Manuas, Brazil, also reported suspiciously high and fast death events that should be audited, but none holds a candle to New York.5
New York’s performance was also unparalleled domestically. The city (and surrounding counties) comprised an incredibly disproportionate/outsize contribution to U.S. excess death in the weeks after the pandemic declaration. Compared to other metropolitan areas, excess mortality was up to 14 times higher.6 Simply put, nothing remarkable happened in most U.S. cities and counties, and without New York, the illusion of a pandemic would have been impossible.
When it comes to “pandemics” in New York history, the reported all-cause death rate, peak, and duration of the spring 2020 event somehow exceeded that of the autumn 1918 event. Notably, both events occurred “off-season” from normal winter respiratory illness peaks in northern latitudes, which raises questions about how the accused pathogens know to strike when their sudden appearance can’t be hidden and just before or after colder-weather factors are in the mix.
The NYC health department’s Summary of Vital Statistics 2020 report observed 2020’s excess compared to 1918, as did media, uncritically and with few questions.7 No explicit comparison to the springtime “Russian flu” event of 1890 was made, despite that “outbreak” having been later blamed on a coronavirus. Still, the 2020 event exceeded that of 1890, implying a deadlier pathogen and/or worse “treatments.”
3. No Precedent?
Even were the tall tales about foreign-born flus true, no “silent” biological or epidemiological mechanism can possibly account for a coronavirus suddenly creating (or helping create) nearly ten times the number of deaths as the World Trade Center disaster. Outside of Hollywood, there is no reason to believe such a huge loss of life could occur from a pathogen believed to transmit from person to person, regardless of “origin”.
The sixteen days of consecutive increases in daily deaths seen in the incredibly steep spring 2020 curve may be a previously unobserved phenomenon in modern death-recording and is by itself grounds for an audit. On the rise especially, the curve lacks the stochastic properties of expected and observed death patterns, including seasonal waves influenced by respiratory illness and other phenomena or incidents known to impact the number of deaths over more than one day in a specific location (e.g., earthquakes, hurricanes, heat waves, power outages). 8
The compressed timeframe of the event likewise defies credulity and is incongruent with the duration and nature of policies implemented. Like Bergamo, the increase is simply too fast, the peak too high, the return to normal too abrupt, and the failure to rise again for the rest of the year too absurd to be believed. The fact that the New York and Bergamo curves look so similar is not evidence of the same viral pathogen attacking both locations with the same fervor but of implementing the same iatrogenic measures and (in my opinion) data engineering feats.
Such “outlier” status should make the New York “COVID” event the object of intrigue and in-depth study by the most prominent scholars from multiple disciplines, not to mention hundreds of journalists and documentary filmmakers. More than four years later, interest is generally low, which is curious and unsettling, given the scale and impact of the event.
4. No Proof?
There is no basic proof in the form of names or death records substantiating the claim that 38,000 New Yorkers died in two and a half months (27,000 more than in 2019).9
State and local laws do not permit death certificates or a death registry to be obtained via freedom of information request, nor are medical examiner’s determinations subject to public disclosure or scrutiny, like they are in other states. Names published by The New York Times, The City, and HartIsland.net comprise less than 10% of the 11-week total.
Given that basic death records for city burials on Hart Island are public (including decedent names), there is no reason the same information cannot be released for every decedent. The dead do not have the same right to privacy as the living, and basic facts about a death are a matter of public interest and accountability for proper stewardship of vital records. The failure to allow the public to verify the toll is itself reason enough for all statistics related to the event to be treated as potentially manipulated and/or partially fabricated.
It must be shown that the number of people who are claimed to have died on each day actually died on those days, irrespective of whether COVID-19 is blamed. Numbers and unverified images from New York were used to extend shutdowns and sell the world on a new “vaccine.” Illegal decrees and COVID-shot coercion aside, it is indefensible for one of the biggest mass casualty events in a U.S. city’s history to be simply proclaimed as a matter of irrefutable fact by way of digits on a screen. The onus is on state and federal authorities to back up their claim with actual records.
5. No Corroboration of Hospital Event?
Not only did New York City report what has to be the most cataclysmic death event in a city hospital system anywhere ever, they did so during a period of decreased hospital activity and patient volume. More than ~22,000 hospital deaths reportedly occurred in a period that saw 5,800 in the previous year (+280%). Emergency department visits dropped in half simultaneous to a 700% increase (baseline to peak) in patient deaths systemwide and decreased admissions. This makes no sense without a significant number of existing patients having been killed.
Both the state and city health departments told me they do not have daily admission data, which is unacceptable and probably false. I’ve been unable to find records that show when the patients who died during the spike were admitted to hospitals, but fewer patients coming in with record numbers of patients dying inside is grounds for a federal inquiry. The fact that virtually no one has called for such an inquiry is deeply disturbing, especially when hospitals were financially incentivized to test for and code hospitalizations & deaths as due to COVID-19.
Instead, the main focus has been on nursing homes, which reported fewer COVID deaths and lower proportion of death than hospitals did. Nursing homes have been an emphasis of a U.S. congressional committee, which seems to be directing attention away from any federal role or responsibility for what happened in New York and toward state and local officials in charge at the time.
Also concerning: The state’s “HERDS” dataset is incomplete and starts the day after the CARES Act was passed, with no earlier available data.10 The audacity of a state agency to hide or pretend it is impossible to get baseline hospitalization data is reason enough to believe the New York City *overwhelmed hospitals* fervor was nothing less than a hyperreality TV show.
Occupancy data for the *star* of that show - “epicenter of the epicenter” Elmhurst Hospital in Queens - contradicts reports from media and elected officials about the facility being overwhelmed by sick patients.11 Moreover, a comparison of the Elmhurst bed occupancy data reported in the HERDS file and data provided via FOI requests shows a severe discrepancy between the number beds occupied. Both datasets are sourced from the same agency but cannot both be “true.”12 The difference is a premier example of why daily occupancy, admissions, emergency department, and deaths for every NYC hospital going back to 1999 should be released immediately, so that the public can see how busy and full the city’s hospitals really were (or weren’t), in proper historical context.
Finally, despite much attention on ventilators as a “weapon” in a “war” against a “silent killer” - and various reports on the use/misuse of the devices - no public dataset shows how many people were placed on ventilators total or how many of those patients died. There is no excuse for withholding such numbers when the entire nation was subjected to press conferences & headlines about New York’s crisis-level “need” for the devices, which played an outsize role in scaring the world into submitting to a shutdown.
6. No Bodies?
The total number of bodies needing to be managed during the 11-week timeframe of the NYC event is (frankly) hard to believe.13 A ranking of the most deaths per day going back to 1999 makes clear the city had no prior experience in recent decades (if ever) handling the number of bodies it claimed to have handled in late March and April 2020. While “pandemic influenza” mass fatality planning guides anticipated handling 27,000-85,000 deaths in such an event, the estimates appear aggrandized and “flu” could easily be an excuse for preparedness for any highly-unlikely, worst-case-scenario event (e.g., asteroid assault).
From a practical standpoint, the movement of 5-6 million pounds of bodies (3-4 million more pounds than normal) would be hard to hide from public view. Many New Yorkers have cameras on their phones, yet no pictures & videos on social, mainstream, or independent media depict anything that corroborates the existence of a mass fatality emergency or scale of the death toll. Instead, images and footage of unremarkable incidents (moving a body or two), “props” (refrigerated trailers), and unverified “scenes” (drones flying over burial trenches) were used as propaganda to show “something” was happening.
The body management task in hospitals defies credulity, especially because documentation is scant or confusing. Total morgue capacity in NYC hospitals is reportedly 800 decedents.14 This would make the normal daily death rate 10%-12% of capacity, with increases to 25-85% for 45 consecutive days during the spring spike. That kind of escalation without corresponding testimonies from doctors and nurses is suspicious.
The total number of bodies placed into storage units sent to hospitals by city agencies is undisclosed, but FEMA refrigerator trucks were underutilized as morgue storage and account for only 5% of the total number hospital deaths. Even with additional storage, a monumental hospital casualty event was reported and must be publicly audited, not only for accountability purposes but so hospital systems around world can verify and learn from what New York’s facilities claim to have experienced.
Oddly, there is no single detailed report showing exactly how (and how many) decedents were managed and transported by medical examiner staff and National Guard & U.S. Army units sent to assist the city. Data obtained from the city medical examiner’s office shows a three-day 11,000-death processing event at the end of April, with no explanation of why or how that magnitude of processing occurred.15 The New York City medical examiner’s office appears to be entirely unaccountable with regard to the spring 2020 event and/or operating under federal direction. Either way, it’s a problem and is obstructing the truth being disclosed.
7. No Explanation for Young Deaths?
There was an astounding ~200% increase in deaths among younger, working-age adults (25-54 YO), most of which attributed COVID-19 as underlying cause and occurred in hospitals.16 This is especially troubling because
a) a full 25% of all COVID deaths in the U.S. at that time were in New York City (!),
b) the incidence of COVID deaths in adults under age 69 is known to be very low, and
c) no other city in the world experienced a similar magnitude of younger-adult deaths in the timeframe or thereafter (as far as I can tell).
Lest we forget, the young deaths in NYC - and the myth of ‘asymptomatic transmission’ - were used as propaganda to sell Americans on the threat posed by a spreading pathogen. It is highly unlikely that any generation under age 65 would have obeyed “stay home” orders for an illness affecting only the elderly.
The fact that no study or separate investigation has been conducted on why the city reported so many young deaths is bizarre. A doctor who was in a New York hospital, then testified to a U.S. Senate committee and has risen to celebrity status, said he saw younger adults suffering from COVID-19 but does not think an investigation of city hospitals is warranted on that basis alone. Such an attitude is perplexing and another sign (one of many) that something very unusual occurred and a full review of patient records desperately needed.
8. No Nursing Home Resident Total?
Multiple investigations and hearings around the Cuomo administration’s so-called nursing home policy have come and gone without reporting the total number of facility residents that died during the NYC event, irrespective of place or cause of death.
The much-repeated “9,000” admissions/readmissions from hospitals to nursing homes cited by AP News in February 2021 is a statewide aggregate number divorced from a baseline. It makes for a good soundbite or headline but means very little without context or a sense of what’s normal, and does not itself establish a casual link between those admissions and the number of nursing home residents who died. Without a daily time-series (or county-specific time-series) it is impossible to see the “mechanics” of what occurred.
Because NYC hospital discharges to skilled nursing facilities dropped 20% in 2020, and the raw-number decrease is curiously close to the increase hospital inpatient deaths during the spring death spike, it suggests many nursing home residents who went into hospitals didn’t make it out alive or that an incredible number of hospitalized people who would have normally been sent to a nursing home afterward died. Why officials are continuing to ignore or hide how many nursing home residents perished in the city’s spring death spike (and who all died in hospitals) is unclear and inexcusable.17
9. No In-Depth Study of Home Death Event?
There was a shocking six-week, 250% increase in deaths occurring at Home, driven by an unprecedented, under-investigated, and largely unexplained cardiac arrest event.18 Media and officials reported people were staying away from hospitals and did not seek medical care, yet 9-1-1 call and ambulance dispatch data show a 25% increase in calls for medical help during the first weeks of the emergency period (exception: Manhattan).
While the data could be manipulated, some calls simulated, and a portion of dispatches sent out merely to blare sirens and scare people, the rise contradicts the claim that people were afraid to go to the hospital, since those calling 9-1-1 want medical help. “Worried well” calling for paramedics doesn’t explain the cardiac event nor does the catch-all “panic,” especially when
there was a 183% increase in dead on ambulance arrival cardiac calls,
the cardiac arrests manifested characteristics not necessarily associated with basic anxiety,
the spike happened alongside changes to calls directed to the Fire Department of New York (FDNY) & deadly protocols issued to emergency medical services.19
The Home event is partly blamed on COVID-19, with the “new disease” being the second leading cause of NYC Home deaths. As if people suddenly dying at Home of a respiratory virus weren’t ridiculous enough, a full 40 percent of Home deaths in the entire U.S. that attributed COVID-19 as underlying cause in April 2020 were in New York City, where less than 3% of the country’s population lives!
The trajectory and shape of the home COVID death curve mirrors that of the home heart-related death curve, which raises the possibility that COVID deaths are deaths from other causes but for which there was record of a positive SARS-CoV-2 test result, qualifying the death as a “COVID death” per WHO and CDC coding guidance.
Because deaths at Home are normally the most-autopsied, associated autopsy records are a potential source for verifying the idea of a coronavirus contributing to the Home death event. Unfortunately federal data show that autopsies conducted on NYC home deaths fell 67% during the spike. It’s hard to blame the decrease on staff shortages when records show OCME hired additional positions and received assistance from the U.S. Army and National Guard. If nothing else, a failure to perform a normal number of autopsies has the appearance of trying to cover up undisclosed factors involved in a highly unusual Home death surge.
It is possible the Home death data reflects an altered or expanded definition of where people died. “Home” refers to a decedent’s personal, private residence'; undisclosed guidelines could have been applied during or ex post facto of the spring event. For example, deaths in congregate settings for younger adults, or care facilities that are not skilled nursing homes per se. If that’s the case, the presentation of the Home death event is not entirely genuine and death records need to be reviewed and corrected.20
10. No Accountability for Ambulance Activity & Protocols?
What happened with ambulances during the first 6-8 weeks of the New York death spike is probably the most under-discussed aspect of the entire event. Space prevents a full treatment of issues and questions; suffice to say, ambulance activity shows disturbing patterns that don’t fit media reports and studies about what happened with emergency calls and medical services, and why.
In addition to those mentioned in the previous section on Home deaths, I see these troubling trends during the emergency period:
Dispatches transporting patients (e.g., to the hospital) did not rise with the jump in calls. They were initially normal and then went down, not up. Orders given to EMTs show responders were urging to keep patients away from "overwhelmed" hospitals.21
Unlike the other four boroughs, dispatches in Manhattan did not increase (and dropped slightly) with the federal “15 Days to Slow the Spread” announcement. Reasonable explanations include an estimated 450,000 Manhattan residents departing the city for other places during the shutdown and the drop in workday commuters & tourists. Arguably, if ambulance dispatches in Manhattan are normally driven by those populations, the absence of those groups should have resulted in a more significant drop than the one observed.
There was a 300% increase (base to peak) in dispatches ending in refused medical aid (RMA). Analysis of calls by type & severity level suggests some RMAs were people were sick enough to go to the hospital; however, nearly 20,000 of the RMA calls were coded as severe in nature (severity code 1 or 2). It makes little sense that New Yorkers with severe medical issues - or their loved ones or bystanders - called 9-1-1 and then refused treatment & transportation to a hospital.
Refusals in RMAs are usually on the part of the patient, but orders issued during the timeframe show that the person doing to the refusing and the medical aid being offered could have been involved in the RMA spike. For instance, if a patient refused a breath-actuated nebulizer (March 6) or surgical mask (March 17), or resisted use of an alternative airway (March 20), it may have been grounds to code the dispatch as RMA. A March 27 bulletin from FDNY loosened oversight for RMAs, including in instances where the patient had received medication or was at high risk of severe outcome. Such an allowance being made for patients in need of a hospital during an emergency is troubling. Some anecdotal evidence raises the question of whether - in some cases - it was first responders who refused medical aid when it should have been given. Not far from the city, in northern New Jersey, paramedics reportedly refused to take a man with liver condition to the hospital and relented under pressure from the man’s wife when they came back a second time. Similar instances were documented nearby.
Thousands of New Yorkers, including those I’ve spoken to directly, testify to the incessant sound of sirens in the first weeks of the shutdown. The overall increase in dispatches corroborates their memories, as does the city simply being more quiet and residents perhaps more attuned to the sound amidst the relative silence. Some have said ambulances were driving around the city empty, on purpose, sirens & lights on, to make people afraid and/or convey the “emergency” situation.22 Though they are a small raw-number of the total rise in dispatches, the sudden and brief increase in uncoded ambulance dispatches (null value) may help support the “Empty Ambulance hypothesis”.
The ambulance dispatch datasets are extremely complex and warrant forensic investigation by qualified auditors and computer scientists. Ideally, this would involve multiple credentialed parties who have no political, professional, or personal ties to any New York or federal agency, workers’ union, or official conducting analysis independently.23 In addition, all call recordings, transcripts, and dispatch reports should be analyzed and verified as authentic and having occurred on the date claimed.
11. No Records, No Response?
Public agencies and researchers have resisted, refused, or exercised reticence toward releasing or providing taxpayer-funded data in response to requests and, in some cases, have done so in a manner suggestive of fear or secrecy. Examples follow:
Request to New York City Health + Hospitals Corporation (HHC) for daily death and blood culture data between 2017-2020: Delayed six months with a final response granting records for 2020 only; appeal denied.
Inquiry to HHC COVID Research Committee regarding discrepancy between data supplied to researchers and data reported to HDNY: Ignored. (Inquiries to the researchers also unanswered.)
Requests to HHC employees for data in two studies that report taxpayer-funded data were ignored after authors initially said they would supply it.
Current requests to HHC for medication & intubation data and emergency department visits are each 1-3 months overdue.
Request to the Office of the Medical Examiner for records related to anomalous processing event: Submitted in December 2023 and delayed til October 2024 (still outstanding)
Request to FDNY Chief Medical Officer for 911 call data in study: Denied (“At this time, we cannot provide this.”)
FDNY suddenly closed a request for ambulance transfer data, following a 14-month saga. Appeal submitted; no response to appeal to date.
Request to NYPD for daily dead on arrival (DOA) calls: Submitted March 2024, delayed til August 2024; no response to recent email asking for status update.
In my advocacy efforts and policy work, I’ve submitted records requests to entities in nearly every state in the U.S., including to many big-city and federal agencies. Public employees in a large city ignoring or circumventing records requests is, in some ways, par for the course.
However, the pattern of recalcitrance I’ve experienced in the past two+ years actively investigating the New York event involves data most critical to verifying official and media claims about the event itself — and points to a culture of, or preference for, self-protection rather than transparency around what did or did not happen. I’m left with the impression that conceal, don’t reveal is a guiding principle for some entities and individuals when it comes to the spring 2020 spike.
What to Do
New York residents and legislators with an interest in holding leaders accountable for the “pandemic response” are well-positioned to
demand a full and public release of death certificates with names, dates of death, places of death, and attributed causes as a first step to substantiating the mortality curve,
pressure public agencies to stop withholding data and delaying requests for public records,
contact members of the U.S. House Select Subcommittee on the Coronavirus Pandemic and urge them understand what data regarding nursing homes has been suppressed and to open a separate inquiry into the New York City death spike. (This is also something any American can do.)
send this article - or this one - to elected officials, activists, and other New Yorkers and let them know “Cuomo sending COVID-positive people into nursing homes” does NOT sufficiently explain the city’s spring 2020 death event.
The specter of death & doom in New York City was used to substantiate a pandemic declaration, upend life as We the People knew it, and usher in months & years of harms against children and adults around the world.
For that reason, demanding the truth about the event is not only the responsibility of the 8 million people who live in the five boroughs, but of all Americans who want the truth about what occurred, why, and how.
Article is subject to revisions/updates, typo corrections, etc. Any errors in analysis, content, or interpretation will be formally noted. All Substack posts related to the NYC event here.
I and/or associates have reported many of these findings previously; this list puts some of that work in one place. I have not yet fully addressed the troubling addition of “probable” COVID deaths in April/May 2020. When I do, I will likely add it to this list under the heading “No Transparency about the Probables” or similar.
Even researchers from Northwell Health system said, “Our [testing] data reveal that SARS-CoV-2 incidence emerged rapidly and almost simultaneously across a broad demographic population in the region. These findings support the premise that SARS-CoV-2 infection was widely distributed prior to virus testing availability.” [emphasis added] Likewise, viral genomic sequencing and antibody studies concluded SARS-CoV-2 was widespread in early February 2020, if not much sooner.
I say “spreading respiratory disease like ‘COVID’” but have made clear elsewhere that I do not believe there was a new cause of death or a spreading respiratory disease in 2020 adding risk of severe illness or death.
See figures 2-5 in Does New York City Make Any Sense? and graph in this post.
The counter-examples are informative as well: Berlin, Tokyo, Sydney saw no substantive increase in deaths during spring 2020. Domestically, New Orleans and Detroit did; Houston and Atlanta did not.
“The COVID-19 pandemic resulted in a mortality rate of 241.3 deaths per 100,000 population in 2020, its impact exceeding the 1918 influenza pandemic in New York City, which had a mortality rate of 228.9 deaths per 100,000 population.” (p. 8)
I am happy to review data from anywhere in the world recorded since 1900 that shows 15+ days of consecutive increases in all-cause deaths in a single city, county, or small region. Parts of France during a summer 2003 “heat wave” event may come close.
FEMA COVID-19 Funeral Assistance data for New York City resident deaths fails to substantiate the toll. Less than 50% of COVID deaths in the spring are connected to an application and just over a third received funds. These figures are suspiciously low for a high-profile disaster and disaster relief program.
For example, the state shows 510 beds were occupied on April 2, 2020, but HHC says 299 beds were filled with patients. Which one was it? We effectively see two different stories about Elmhurst in the two occupancy datasets. The state’s story shouts “DISASTER!!” - which was simulation specialist Colleen Smith’s vibe about what was happening. HHC’s story says, “Everything’s fine here. Situation normal/below normal” - which is consistent with Elmhurst’s ED visit and admissions. The state’s data appears “pushed” from the left and gives the impression the hospital was much fuller than the data obtained directly from HHC. My attempts to reconcile the difference with the state (which I reported here) were unsuccessful.
“No Bodies” is somewhat tongue-in-cheek and used as a rhetorical device. The subtext is “Not Enough Bodies” and “No Real Evidence of the Volume of Bodies Suggested by the Data”.
The number is reported in this GNYHA document (p. 8) and needs to be verified.
Ten months have passed since I submitted a FOIL for related records and I’ve yet to receive the documents I asked for.
See also graphs illustrative of the disproportionality between NYC and the rest of NY state.
The demographically-comparable Chicago did not experience this magnitude of deaths at home or an onslaught calls to 911. Significant OHCA events in London, Paris, Lombardy, and Detroit in spring 2020 were also reported and should be investigated.
I’ve reported previously that an NYPD detective I’ve spoken with about his experience said his DOA unit did not see a dramatic increase in calls during the spring 2020 event. I hope he will go on-record in the future about what he experienced. File of orders to FDNY & EMS below.
All Ems Orders
5.58MB ∙ PDF file
Reports about the National Guard picking up decedents at “homes and nursing homes” hint at this possibility, as does Andrew Cuomo’s infamous rhetorical question, “Who cares [if they] died in the hospital, died in a nursing home? They died!”
The American Rescue Plan Act, passed in March 2021, retroactively reimbursed providers for all events relating to a COVID patient, even if the patient was not transported anywhere.
The role of sound (or absence thereof) during the event is worth further exploration. Studies on how ambulance sirens, the “songs” of cicada broods, or other kinds of wave-like patterns manifesting a certain tone or frequency induce anxiety in some people may be relevant. The extent to which military and intelligence agencies have studied and employed sound in experiments or during emergencies and other operations is also of interest.
Downloads of the data over the past few years show signs of tampering. I am not in the position to prove such adulteration has occurred but would be happy to speak to anyone acting in an official capacity about some of the changes I have seen.’
___
You must not wait for another catastrophic crisis (at times manufactured but we are prevented from making our own basic personal decisions or accessing needed drugs and response tools) to catch you off-guard. We must take charge and be prepared today so that we can enjoy peace of mind tomorrow.
Enter the Wellness Company as a solution and a willing participant in the health care conversation. From telemedicine, prescriptions, memberships, and supplements, TWC is leading America with alternative choices to the traditional health care model.
If you wish to give a donation to help me, you can at:
Zelle:
sr7283@gmail.com
Or Ko-Fi
Ko-fi.com/drpauleliasalexander
Or to my address at:
150 South 8th Street
Unit 170
Lewiston, New York
14092
Alternatively, please consider going from an UNPAID subscriber or follower to a PAID at $5 per month or $30 per year. This can provide me help. If this is not possible at this time, this is ok, please remain a subscriber for FREE and there is no difference between FREE and PAID. No restrictions.
Please consider support of a good company Drs. McCullough, Risch, Thorp, myself support (they are our sponsors), The Wellness Company; see the emergency preparation kit (key component being antibiotics you were denied by doctors, pharmacists, governments during the fraud COVID), first aid kit, travel emergency kit, contagion control kit etc. Please consider the SPIKE SUPPORT (spike protein DETOX dissolving spike from mRNA vaccine, this is critical to remove spike form the mRNA vaccine/and DNA viral vector) formula with NATTOKINASE as well as the triple formula (SPIKE SUPPORT, BROMELAIN, CIRCUMIN)
Great sharing. I've been following Jessica Hockett in her relentless efforts to uncover the truth behind the anomaly of the Spring 2020 "spike in covid deaths" in NYC.
Good to see her receive well-deserved attention and acclaim for her dogged determination to get to the bottom of this matter.
Something very evil and dark and wrong has been happening for the past 4 and a 1/2 years. Thank you.