

I wrote these reviews near 3 years now and more (with some sound colleagues) on the harms, ineffectiveness of COVID face masks, including N95; toxicity & harm to pregnant women & children, see below
People like McCullough, Risch, Tenenbaum, Dara, Oskoui etc. were my co-writers! They/we were prescient on the fraud masks that Fauci et al. knew could never work! Tucker at AIER was ahead of the game


This is a public health warning to the US population and elsewhere, as it appears that our public health agencies and television medical experts seem unable to address key health messages that could have a dramatic effect in reducing risk of severe sequelae in higher-risk populations such as the minority and African-American population to the scourge of SARS-CoV-2. This is now clear. They have squandered many an opportunity to inform the public on simple yet very effective messaging that could reduce morbidity and save lives. Not just for Covid-19, but our focus here is on Covid-19.
For example, obesity has emerged as a potent human target for the SARS-CoV-2 in most studies, in addition to being elderly, frail and having comorbid conditions. It would behoove our agencies to address these risks in a large-scale education program for the populace and especially by calling for a reduction in body weight and particularly for the minority sub-groups (African-Americans). In a similar light, studies have shown that vitamin D supplementation for African-Americans has been associated with a lowered risk of severe disease and mortality from the SARS-CoV-2.
Early ambulatory outpatient treatment with successful combination and sequenced antiviral agents, corticosteroids, and anti-clotting therapeutics should be used widely to help the people at risk. The African-American community is aware that, “Covid (is) a killer for the obese: like pouring gasoline on top of a fire.” Unfortunately, more than a year into the pandemic, the manifest issue of public health education and sound policy decisions remain aloof, given the erratic and confusing responses from the health and governing officials. We are calling for an aggressive focus on our minority populations (and all of our population), as they are usually overlooked and disregarded by public health leaders and agencies. We plead for effective and needed public health messaging.
With that clarion call, we pivot and refer here to another looming concern and this is the potential danger of the chlorine, polyester, and microplastic components of the face masks (surgical principally but any of the mass-produced masks) that have become part of our daily lives due to the Covid-19 pandemic. We hope those with persuasive power in the government will listen to this plea. We hope that the necessary decisions will be made to reduce the risk to our populations.
Emergent reports, albeit nascent and anecdotal but nevertheless vitally important (and will be clarified and defined in time) regarding the manufacture of masks, where, “many of them (face masks) are made of polyester, so you have a microplastic problem…many of the face masks would contain polyester with chlorine compounds…if I have the mask in front of my face, then of course I inhale the microplastic directly and these substances are much more toxic than if you swallow them, as they get directly into the nervous system.”
There are also reports of toxic mould, fungi, and bacteria that can pose a significant threat to the immune system by potentially weakening it. Of particular concern to us is the recent report of breathing in synthetic fibers in the face masks. This is of serious concern. “Loose particulate was seen on each type of mask. Also, tight and loose fibers were seen on each type of mask. If every foreign particle and every fiber in every facemask is always secure and not detachable by airflow, then there should be no risk of inhalation of such particles and fibers. However, if even a small portion of mask fibers is detachable by inspiratory airflow, or if there is debris in mask manufacture or packaging or handling, then there is the possibility of not only entry of foreign material to the airways, but also entry to deep lung tissue, and potential pathological consequences of foreign bodies in the lungs.”
Reports are that “Graphene is a strong, very thin material that is used in fabrication, but it can be harmful to lungs when inhaled and can cause long-term health problems.” We argue that there is a risk of potential ‘future’ inflammatory/fibrotic lung diseases because we are inhaling these materials in the masks now for over one year with more duration to come and no end in sight. These substances might also be highly carcinogenic. Not just for us as adults but we must be very concerned about the risks especially to our children since they depend on us as mentors and guides for their decision-making. It is our children that we are very concerned for.
These blue surgical masks pervade our lives. “Health Canada has issued a warning about blue and gray disposable face masks, which contain an asbestos-like substance associated with “early pulmonary toxicity.” The warning is specific to potentially toxic masks distributed within schools and daycares across Quebec. Health Canada (and full praise to them)….“discovered during a preliminary risk assessment that the masks contain microscopic graphene particles that, when inhaled, could cause severe lung damage.”
Reports are that “for a while now, some daycare educators had expressed suspicion about the masks, which were causing children to feel as though they were swallowing cat hair while wearing them. We now know that instead of cat hair, children were inhaling the equivalent of asbestos all day long.”.It appears to be a substance known as graphene. What is indeed alarming is that “the SNN200642 masks that were being used all across Canada in school classrooms had never been tested for safety or effectiveness.” This is indeed a catastrophic failure by the regulators as these surgical face masks are linked to early pulmonary toxicity.
.
.
.
Also:

Summary: Children do not readily acquire SARS-CoV-2 (very low risk), spread it to other children or teachers, or endanger parents or others at home. This is the settled science. In the rare cases where a child contracts Covid virus it is very unusual for the child to get severely ill or die. Masking can do positive harm to children – as it can to some adults. But the cost benefit analysis is entirely different for adults and children – particularly younger children. Whatever arguments there may be for consenting adults – children should not be required to wear masks to prevent the spread of Covid-19. Of course, zero risk is not attainable – with or without masks, vaccines, therapeutics, distancing or anything else medicine may develop or government agencies may impose.
How did this blue surgical mask and white cloth mask come to dominate our daily lives? Well, indeed, the surgical masks and white cloth (often homemade) masks have become the most contentious and quarrelsome symbol and reminder of our battle with SARS-CoV-2 and the disease it causes, Covid-19. The mask has become so politicized that it prevents rational consideration of the evidence (even across political lines) and drives levels of acrimony, invidious actions, disdain, and villainy among wearers to each other who feel threatened by the individual who will not or cannot wear a mask.
But how dangerous is this virus? Based on studies done by Professor John PA Ioannidis of Stanford University, we know that we are dealing with a virus that has an infection fatality rate (IFR) of 0.05 in persons 70 years old and under (range: 0.00% to 0.57% with a median of 0.05% across the different global locations; with a corrected median of 0.04%). This compares quite well to the IFR of most influenza viruses (and even lower), and yet the draconian and massive reactions to SARS- CoV-2 have never been employed during influenza season.
Given this knowledge it is more than perplexing as to why our governments, at the behest of their public health advisors, have accepted as a fait accompli what we refer to as a ‘great deception’ or lie, convincing us of inevitable and severe consequences if anyone is infected with SARS-CoV-2.
Yes, the public was lied to and deceived from day one by governments and their medical advisors and the media medical cabal with its incessant messaging that we were all at equal risk of severe illness or death if infected, young and old. They subverted science. This caused irrational fear and hysteria and it has held on. This type of deception and the resulting unfounded fear has been driven by the media despite “a thousandfold difference in risk between old and young.”
We suggest that this has always been known, and yet this disinformation and related falsehoods were spread seemingly both willfully and knowingly by our leaders and the media. Such conflation of the risks between the young and the elderly population with comorbidities and at risk is wrong-headed and creates unnecessary fear for all. It is well known that there is a distinct stratified risk (strongly associated with increasing age and comorbidities).
Additionally, data now suggests (even though still nascent) that children not only have extremely low risk as mentioned above but also that they naturally have the capability of evading the SARS-CoV-2 virus due to the lack of the ACE-2 receptors in their nostrils. It escapes us as to why this deceit continues to be served to the public and has not been stopped forthwith.
What does the evidence show? Well, evidence is accumulating about the potential harms of mask use (references 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23). For example, the CDC’s own February 2021 double-mask study reported that masking may impede breathing – which can trigger a variety of other problems including acute anxiety attacks in susceptible individuals. These harms are even more likely to occur to children, particularly smaller children.
The scientific evidence in total also suggests masks (surgical and cloth masks) as currently used are ineffective in reducing transmission (references 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25). Even if we tried to tease out ‘minimal help’ and say ‘they may help a little,’ these Covid-19 masks are largely ineffective. In many reports, conclusively so. As an example, a very recent publication stated that face masks become nonconsequential and do not function after 20 minutes due to saturation. “Those masks are only effective so long as they are dry,” said Professor Yvonne Cossart of the Department of Infectious Diseases at the University of Sydney.” As soon as they become saturated with the moisture in your breath, they stop doing their job and pass on the droplets.” In a similar light, there are indications that wearing a mask that has already been used, which is very common, is riskier than if one wore no mask at all. The evidence on mask mandates is also clear in that they are ineffective and do not work (references 1, 2, 3, 4, 5, 6) to prevent the spread of respiratory viruses like SARS-CoV-2.
We don’t have a wealth of scientific evidence on exactly when it is safe or not safe for children to be masked, but here’s a good rule of thumb. If you wouldn’t put a child in the front seat of your Prius without disabling the airbag – think twice before requiring an otherwise healthy child to wear a mask – or even forcing them to social distance in school.
On the dangers of masks generally, a recent mini-review reported “There are insufficient data to quantify all of the adverse effects that might reduce the acceptability, adherence and effectiveness of face masks.” We agree that the adequate primary type comparative effectiveness research is still not available but we do have strong anecdotal, reported, and real-world information as indicated above, along with some primary evidence, which we have judged appropriate to inform the discussion sufficiently.
During April to October 2020 in the US, emergency room visits linked to mental health problems (e.g. anxiety) for children aged 5-11 increased by nearly 25% and increased by 31% for those aged 12-17 years old as compared to the same period in 2019. During the month of June 2020, 25% of persons aged 18 to 24 in the US reported suicidal ideation. While some of this may be related to the pandemic, we suspect that it is largely a function of our response to the pandemic.
One of the most starkly revealing and troubling observations come from Dr. Margarite Griesz-Brisson MD, PhD, who is one of Europe’s leading neurologists and neurophysiologists focused on neurotoxicology, environmental medicine, neuro-regeneration and neuroplasticity. She has gone on record stating: “The rebreathing of our exhaled air will without a doubt create oxygen deficiency and a flooding of carbon dioxide. We know that the human brain is very sensitive to oxygen deprivation.” There are neurons, for example in the hippocampus that cannot survive more than 3 minutes without an adequate supply of oxygen. Given that such cells are so sensitive to oxygen deprivation, their functionality must be affected by low oxygen levels.
Oxygen deprivation can cause metabolic changes and the metabolic changes that happen in neuronal cells are vitally important for cognitive functioning and brain plasticity and it is known that when drastic metabolic shifts occur in the brain, there are consequent changes of oxidative stress (cellular oxidative state) and these have a significant role in managing neuron functioning (we do not claim that masking would produce complete absence of oxygen of course).
The acute warning symptoms are headaches, drowsiness, dizziness, reduced ability to concentrate and reductions in cognitive function. Given that the development of neurodegenerative diseases can take years to develop, then what are the potentially deleterious effects of the use of masks, especially in children, when masks are used over the majority of their day? We and particularly parents, must consider this and weigh the benefits versus the harms. Are there benefits enough to warrant use relative to the potential harms? If the harms outweigh the benefits, then we cannot in good conscience advocate for mask use. Moreover, the continual and stressful impacts of masking (and school closures) will also have a known and deleterious impact on the immune systems in children (and adults).
Other medical harms relate to the notion that children and adolescents have an extremely active and adaptive immune system, a system that must be challenged in order to retain functionality. Yet by severely restricting children’s activities because of lockdowns and masking (physical activity/fitness exercises are almost impossible whilst wearing a mask), we are probably hobbling their immune systems. Evidence indicates that regular physical activity and frequent exercise enhance immune competency and regulation.
A child unexposed to nature has little defense against a minor illness, which can become overwhelming due to the lack of a primed ‘tuned-up’ and ‘taxed’ immune system. A robust immune system shortens an illness as a consequence of the presence of preprogrammed anamnestic immunity. Preventing children from such interactions with nature and germs can and does lead to overwhelming infections and serious consequences to the health and life of a child. We might be setting up our children for future disaster when they emerge from societal restrictions fully and with no masks, to then be at the mercy of normally benign opportunistic infections with a now weakened immune system. This cannot be disregarded as we consider the consequences of our actions today in this pandemic and the questionable lockdowns, school closures, and mask policies.
A German-wide registry (not the optimal highest-quality study) used by 20,353 parents who reported on data from almost 26,000 children, found that the “average wearing time of the mask was 270 minutes per day. Impairments caused by wearing the mask were reported by 68% of the parents. These included irritability (60%), headache (53%), difficulty concentrating (50%), less happiness (49%), reluctance to go to school/kindergarten (44%), malaise (42%) impaired learning (38%) and drowsiness or fatigue (37%).”
Concerns are being raised regarding psychological damage and why a mask is not ‘just a mask.’ There is tremendous psychological damage to infants and children, with potential catastrophic impacts on the cognitive development of children. This is even more critical in relation to children with special needs or those within the autism spectrum who need to be able to recognize facial expressions as part of their ongoing development. The accumulating evidence also suggests that prolonged mask use in children or adults can cause harms, so much so that Dr. Blaylock states “the bottom line is that [if] you are not sick, you should not wear a mask.” Furthermore, Dr. Blaylock writes, “By wearing a mask, the exhaled viruses will not be able to escape and will concentrate in the nasal passages, enter the olfactory nerves and travel into the brain.”
.
.
.
Also:

he question on whether to wear a face mask or not during the Covid-19 pandemic remains emotional and contentious. Why? This question about the utility of face coverings (which has taken on a talisman-like life) is now overwrought with steep politicization regardless of political affiliation (e.g. republican or liberal/democrat).
Importantly, the evidence just is and was not there to support mask use for asymptomatic people to stop viral spread during a pandemic. While the evidence may seem conflicted, the evidence (including the peer-reviewed evidence) actually does not support its use and leans heavily toward masks having no significant impact in stopping spread of the Covid virus.
In fact, it is not unreasonable at this time to conclude that surgical and cloth masks, used as they currently are, have absolutely no impact on controlling the transmission of Covid-19 virus, and current evidence implies that face masks can be actually harmful. All this to say and as so comprehensively documented by Dr. Roger W. Koops in a recent American Institute of Economic Research (AIER) publication, there is no clear scientific evidence that masks (surgical or cloth) work to mitigate risk to the wearer or to those coming into contact with the wearer, as they are currently worn in everyday life and specifically as we refer to Covid-19.
We present the evidence in full below. We also state that should adequate evidence emerge that supports the effectiveness of surgical and cloth masks in this Covid pandemic (or any similar type masks), then we will change our position and conclude otherwise. Our focus is on face masks for Covid but we will touch gently on the issue of school closures and lockdowns, as these three issues remain the key public health policy catastrophes we have faced as global societies.
Back in August 2020, a survey by Pew indicated that 85% of Americans wore masks when in public all or most of the time. So, the public has been using masks extensively. We thus set the table in this review on the effectiveness of masking for Covid by asking, if these surgical and cloth masks are effective, why did incidence of the virus (or actual disease; and they’re not the same thing) escalate so rapidly despite widespread use? Why is there no evidence across US States and global nations showing that when use is mandated (or not mandated given the general uptake of masking by the public), this contributes to reduced viral transmission? Is there any such evidence?
Orofecal transmission?
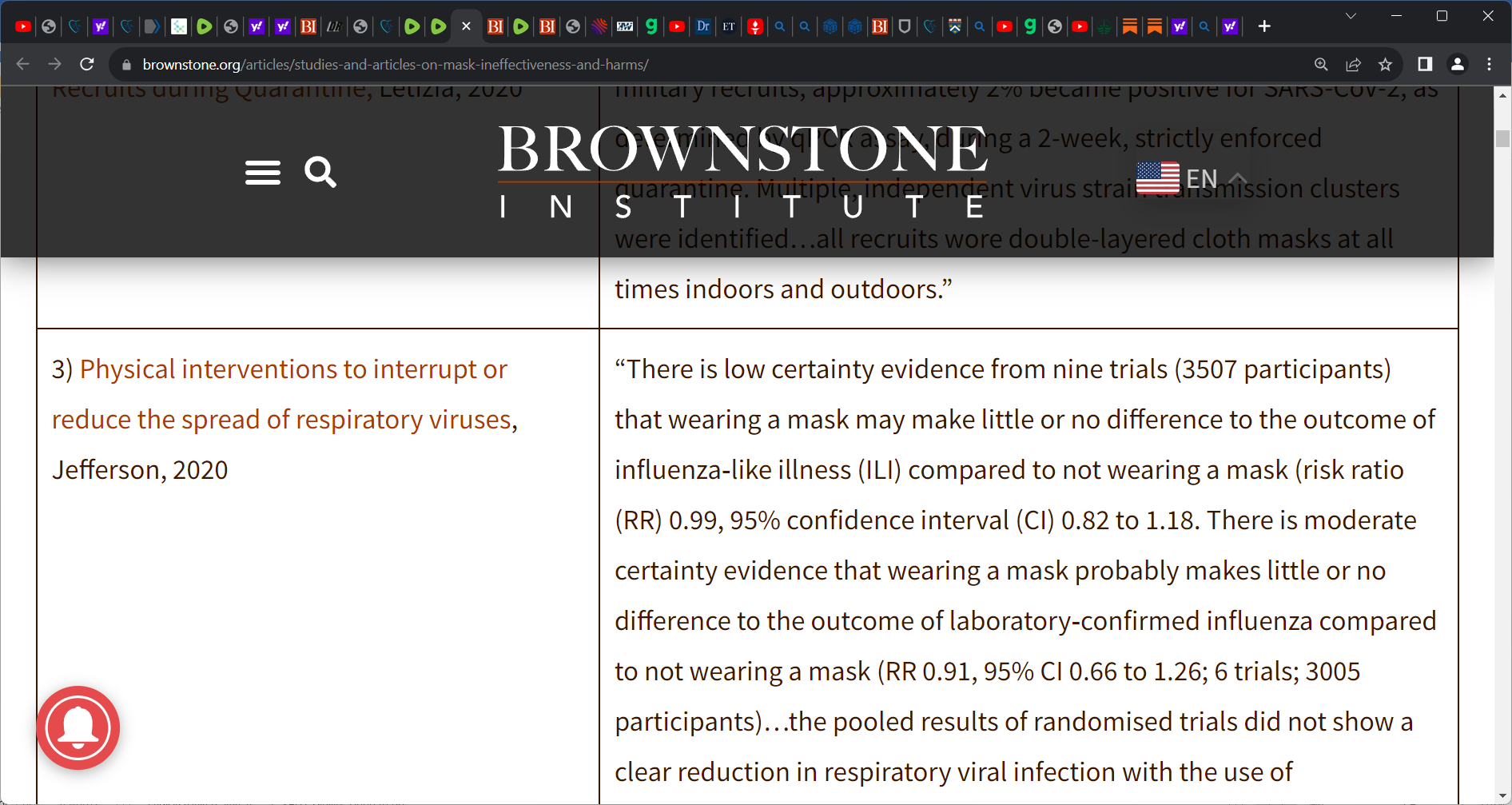
Understanding the transmission of this respiratory SARS-CoV-2 pathogen is also evolving given evidence of orofecal spread as having a potentially larger contributor role in non-respiratory transmission of Covid. As an example, a recent open-evidence review brief by Oxford researchers (Jefferson, Brassey, Heneghan) and its publication in CEBM, reveals the growing recognition that SARS-CoV-2 can infect and be shed from the gastrointestinal (GI) tract of humans. Orofecal spread demands urgent study and if orofecal spread is shown to be definitive and more consequential in Covid transmission, then this could impact mitigation strategies beyond those for respiratory transmission.
Where do we begin on masks? How about infection fatality rate/IFR?
Moreover, we are addressing here highly irrational, punitive, capricious, and groundless societal restrictions for a virus with an infection fatality rate (IFR), based on Stanford University John Ioannidis’s calculations, of 0.05% in persons under 70 years old (across different global nations). Ioannidis’s research was followed up recently by a reported non-institutionalized IFR in the state of Indiana (persons aged > 12 years) of 0.12% (95% CI 0.09 to 0.19) when age 40-59/60 years (reported in the Annals of Internal Medicine), and an IFR when < 40 years old of 0.01% (95% CI 0.01 to 0.02). Persons 60 or older had an IFR of 1.71% (overall IFR was 0.26%).
So why would we continue this way with these unsound and very punitive restrictive policies and for so long once the factual characteristics of this virus became evident and as alluded to above, we finally realized that its infection fatality rate (IFR) which is a more accurate and realistic reflection of mortality than CFR, was really no worse than annual influenza?
How did we get here?
How did we arrive at the confusion and misinformation surrounding mask use which is our focus, yet by extension, the crushing societal lockdowns and harmful school closures? There are serious harms and downsides due to these crushing restrictive policies and we understand that one would think reflexively if there is a pathogen, we should just lock and shut everything down and away. We understand this initial instinct.
However, there are benefits and risks to any action and the harms of these lockdowns and school closures far outweighed the benefits based on what has transpired. We even knew this soon after implementing lockdowns yet we continued catastrophic policies and are still continuing. How did we get here societally? How have our government bureaucratic leaders failed so disastrously?
We lay heavy blame on our government leaders but argue that the so-called ‘medical experts’ who are part of Covid Task Forces and guidance panels have been largely unscientific, illogical, and irrational in their guidance and statements.
Untethered from the reality of things. In many instances just flat out misleading and wrong! The incessant campaign by the media that has worked to drive fear and hysteria in the public is also partly to blame. There appears to be an unholy alliance between the government bureaucrats, the aforementioned ‘medical experts,’ and a willing print and digital media. A vast lot of what these experts say on Covid makes no sense anymore, at times unhinged and lacking of any credibility.
In such incredibly important Covid-related input and guidance, these television medical experts and many government leaders have failed in profound and often unimaginable ways and we are left asking how they got things so very wrong. Is it that these medical experts do not read the science? Or maybe cannot understand the data or science? Which? They talk about following the science but seem blinded to it. They clearly don’t follow the science else we would not be here. They seem to not understand the devastation they have visited upon the lives of so many.
We argue that the messaging by the media and medical experts initially suggested that all persons are of equal risk of severe illness from Covid infection. This is where it all went wrong and where societies were greatly deceived by those who should not have done that. We were never ‘all’ at equal risk. This was deeply flawed and has crippled the US and global nations since day one of this pandemic. This was and remains a flat-out falsehood (untrue) and it has driven irrational fear by the public. This clearly erroneous intimation has stuck in the minds of the public and severely impacted the public’s perception of their risk and how they would move forward.
School closure policy mirrors face mask policy?
What did we know? Let’s address masks by first looking at school closures as it bears mentioning about the disaster the flawed school closure policies directed by our government leaders have caused in our children’s lives. The school closure catastrophe mirrors the masking catastrophe and similar unsound policies. We knew early on in 2020 for example, that the key risk group was elderly persons with medical conditions (though Covid gave way to age due to serious medical conditions or obesity based on existing data). But just look at the complete disaster experts have created with our children in terms of school closures.
Look at what is now known in Ontario, Canada with the union and fees paid to ‘conflicted’ medical experts to drive a school closure message. This is reckless and scandalous! In spite of extremely low transmission rates and very low likelihood of spreading Covid virus among children (or of becoming severely ill from Covid), they have gone on and destroyed a year of the school lives of children due to these nonsensical medical experts and hysterical media and this will carry a huge long-term loss to our children. Who is going to pay for this?
What did CDC and NIH know about risk to children and when did they know it?
Did we have any data or science? Of course we did. Quality research “in the leading journal Nature estimated the Covid-19 survival rate to be approximately 99.995% in children and teens.” We knew this very early on but that did not stop public health agencies and experts from deceiving or failing to inform about the true risk. A recent publication by CDC reported that among in excess of 90,000 students and staff in 11 North Carolina school districts, they found that in-school virus transmission was “very rare.” A similar finding emerged in 17 rural Wisconsin schools.
The Atlantic’s Derek Thompson wrote in January 2021 that “We’ve known for months that young children are less susceptible to serious infection and less likely to transmit the coronavirus. Let’s act like it.” This piece by Thompson was driven by CDC ‘coming’ out in the last week for school reopenings when the data was clear for a very long time that the risk was very low, if at all. Then we are, as is Thompson in his piece, provoked to ask, why did the media, our bureaucratic government leaders, and the medical experts seemingly collude to damage our children with their baseless school closures? Why did they deceive the public for so long? Catastrophic long-term losses for our children’s educational but importantly, their social and emotional/psychological development has accumulated. We know that suicides among children have been escalating. Parents are struggling with the pandemic and homeschooling and children are failing out. This type of unfounded fear has been driven by the media “despite a thousandfold difference in risk between old and young.” They always knew this but continued a bold-faced lie! As a result, this has underpinned an atmosphere of gross distrust of our government officials and medical experts.


It is not unreasonable to conclude that surgical and cloth masks, used as they currently are being used (without other forms of PPE protection), have no impact on controlling the transmission of Covid-19 virus. Current evidence implies that face masks can be actually harmful. The body of evidence indicates that face masks are largely ineffective.
My focus is on COVID face masks and the prevailing science that we have had for nearly 20 months. Yet I wish to address this mask topic at a 50,000-foot level on the lockdown restrictive policies in general. I build on the backs of the fine work done by Gupta, Kulldorff, and Bhattacharya on the Great Barrington Declaration (GBD) and similar impetus by Dr. Scott Atlas (advisor to POTUS Trump) who, like myself, was a strong proponent for a focused type of protection that was based on an age-risk stratified approach.
Because we saw very early on that the lockdowns were the single greatest mistake in public health history. We knew the history and knew they would not work. We also knew very early of COVID’s risk stratification. Sadly, our children will bear the catastrophic consequences and not just educationally, of the deeply flawed school closure policy for decades to come (particularly our minority children who were least able to afford this). Many are still pressured to wear masks and punished for not doing so.
I present the masking ‘body of evidence’ below (n=167 studies and pieces of evidence), comprised of comparative effectiveness research as well as related evidence and high-level reporting. To date, the evidence has been stable and clear that masks do not work to control the virus and they can be harmful and especially to children.
Table 1: The evidence on COVID-19 face masks and mask mandates and harms









The great body of evidence (comparative research studies and high-quality pieces of evidence and reporting judged to be relevant to this analysis) shows that COVID-19 lockdowns, shelter-in-place policies, masks, school closures, and mask mandates have failed in their purpose of curbing transmission or reducing deaths. These restrictive policies were ineffective and devastating failures, causing immense harm especially to the poorer and vulnerable within societies.
Nearly all governments have attempted compulsory measures to control the virus, but no government can claim success. The research indicates that mask mandates, lockdowns, and school closures have had no discernible impact of virus trajectories.
Bendavid reported “in the framework of this analysis, there is no evidence that more restrictive nonpharmaceutical interventions (‘lockdowns’) contributed substantially to bending the curve of new cases in England, France, Germany, Iran, Italy, the Netherlands, Spain, or the United States in early 2020.” We’ve known this for a very long time now but governments continue to double down, causing misery upon people with ramifications that will likely take decades or more to repair.
The benefits of the societal lockdowns and restrictions have been totally exaggerated and the harms to our societies and children have been severe: the harms to children, the undiagnosed illness that will result in excess mortality in years to come, depression, anxiety, suicidal ideation in our young people, drug overdoses and suicides due to the lockdown policies, the crushing isolation due to the lockdowns, psychological harms, domestic and child abuse, sexual abuse of children, loss of jobs and businesses and the devastating impact, and the massive numbers of deaths resulting from the lockdowns that will impact heavily on women and minorities.
Now we have whispers again for the new lockdowns in response to the Omicron variant that, by my estimations, will be likely infectious but not more lethal.
How did we get here? We knew that we could never eradicate this mutable virus (that has an animal reservoir) with lockdowns and that it would likely become endemic like other circulating common cold coronaviruses. When we knew an age-risk stratified approach was optimal (focused protection as outlined in the Great Barrington Declaration) and not carte blanche policies when we had evidence of a 1,000-fold differential in risk of death between a child and an elderly person. We knew of the potency and success of early ambulatory outpatient treatment in reducing the risk of hospitalization and death in the vulnerable.
It was clear very early on that Task Forces and medical advisors and decision-makers were not reading the evidence, were not up to speed with the science or data, did not understand the evidence, did not ‘get’ the evidence, and were blinded to the science, often driven by their own prejudices, biases, arrogance, and ego. They remain ensconced in sheer academic sloppiness and laziness. It was clear that the response was not a public health one. It was a political one from day one and continues today.
A recent study (pre-print) captures the essence and catastrophe of a lockdown society and the hollowing out of our children by looking at how children learn (3 months to 3 years old) and finding across all measures that “children born during the pandemic have significantly reduced verbal, motor, and overall cognitive performance compared to children born pre-pandemic.” Researchers also reported that “males and children in lower socioeconomic families have been most affected. Results highlight that even in the absence of direct SARS-CoV-2 infection and COVID-19 illness, the environmental changes associated with the COVID-19 pandemic is significantly and negatively affecting infant and child development.”
Perhaps Donald Luskin of the Wall Street Journal best captures what we have stably witnessed since the start of these unscientific lockdowns and school closures: “Six months into the Covid-19 pandemic, the U.S. has now carried out two large-scale experiments in public health—first, in March and April, the lockdown of the economy to arrest the spread of the virus, and second, since mid-April, the reopening of the economy. The results are in. Counterintuitive though it may be, statistical analysis shows that locking down the economy didn’t contain the disease’s spread and reopening it didn’t unleash a second wave of infections.”
The British Columbia Center for Disease Control (BCCDC) issued a full report in September 2020 on the impact of school closures on children and found para “that i) children comprise a small proportion of diagnosed COVID-19 cases, have less severe illness, and mortality is rare ii) children do not appear to be a major source of SARS-CoV-2 transmission in households or schools, a finding which has been consistent globally iii) there are important differences between how influenza and SARS-CoV-2 are transmitted. School closures may be less effective as a prevention measure for COVID-19 iv) school closures can have severe and unintended consequences for children and youth v) school closures contribute to greater family stress, especially for female caregivers, while families balance child care and home learning with employment demands vi) family violence may be on the rise during the COVID pandemic, while the closure of schools and childcare centres may create a gap in the safety net for children who are at risk of abuse and neglect.”
Now places like Austria (November 2021) have re-entered the world of lockdown lunacy only to be outmatched by Australia. Indeed, an illustration of the spurious need for these ill-informed actions is that they are being done in the face of clear scientific evidence showing that during strict prior societal lockdowns, school lockdowns, mask mandates, and additional societal restrictions, the number of positive cases went up!
The pandemic response today remains a purely political one.
What follows is the current totality of the body of evidence (available comparative studies and high-level pieces of evidence, reporting, and discussion) on COVID-19 lockdowns, masks, school closures, and mask mandates. There is no conclusive evidence supporting claims that any of these restrictive measures worked to reduce viral transmission or deaths. Lockdowns were ineffective, school closures were ineffective, mask mandates were ineffective, and masks themselves were and are ineffective and harmful.
For a public health regime that claims to "follow the science" they sure do an amazing job of ignoring the studies & side effects that prove them wrong!
This article by Dr. Alexander is an extraordinarily valuable resource for those of us expecting to have to defend ourselves against near-future mandates to participate in ridiculous, harmful, and ineffective measures against this Fall's "new variant."
Meanwhile...
The UK Royal Society has issued a dishonest report that claims non-pharmaceutical interventions (masking, social distancing, lockdowns) 'unequivocally' reduced transmission and death from Covid:
https://www.lifesitenews.com/opinion/fearmongering-experts-try-to-claim-lockdowns-masks-helped-slow-the-spread-of-covid/?utm_source=digest-freedom-2023-08-28&utm_medium=email