

Major stack by Dr. VINAY PRASAD, excellent sharing, informative highlighting what we knew & adding to the body of evidence of the deadliness of the Bourla Bancel Sahin Weissman Malone mRNA vaccine
"COVID19 vaccines linked to myocarditis, pericarditis, ITP, Guillain Barre Syndrome, Bell's Palsy, ADEM, PE, Febrile seizures & more A new analysis of 99 million people"...no age-risk stratification

We knew early on that COVID was amenable to risk stratification and that baseline risk e.g. age and risk was prognostic on outcome so to present this risk data (researchers) devoid of age (and even gender) stratification is sub-optimal and meant in some way to deceive. To hide something, and certainly leaves the reader with questions as to where the risk is…
How could healthy 5 year-old Johnny with no underlying medical conditions be at the same risk of severe outcome as 85 year-old granny with 4 underlying medical conditions? We need to know. This issue of equal risk of severe outcomes regardless of age and baseline risk was one of the great lies of this fraud fake COVID non-pandemic along with the lie of asymptomatic transmission, recurrent infection pre-omicron era etc. What was the purpose of this mRNA vaccine when out of the box we knew it was non-sterilizing and did not stop transmission? Why did we have to take it?
Vinay is excellent here using these words and I quote (Vinay gets it and is being declarative here):
“First, let us be clear, the benefit of COVID vaccination is small, uncertain or not present in several populations. For instance, there is no reliable evidence anyone who had COVID previously had a further reduction in severe disease from getting a dose (or 7 doses) of vaccine.
The theoretical absolute benefit of vaccination depends on the baseline risk so the *upper bound* absolute benefits to healthy people under 20, 30 or 40 were always minuscule— bordering on zero— and possible not present. Available data lacks power to show a benefit in 20 year olds.
Worse, there is not even one reliable study that shows a benefit in children. This means- that for these populations- even rare safety signals can tilt the entire balance. We have previously shown that boosters and dose 2 of mRNA vaccines were, on balance, harmful to young men because the risk of myocarditis was greater than the further upper bound absolute risk reduction in severe COVID19 outcomes.”
Also:
“Now, we see concerning signals for
Idiopathic thrombocytopenic purpura (ITP)
Febrile seizures
Myocarditis/ pericarditis
Racing heart - SVT
Bells palsy (facial paralysis)
Pulmonary embolism
Acute disseminated encephalomyelitis and more”
I want you to understand what he is saying. I am not even focusing on harms here, just the serious limitations we have had whereby we have no sound data, none, across 4 years for COVID and now 3 years for this fraud vaccine. I have been clear, IMO these mRNA vaccines never ever worked. Never protected the upper airways.
As of today, we have no RCT, no reliable comparative effectiveness research, none, showing that these shots reduce risk on hard patient-important outcomes like death, hospitalization, ICU etc. None. Adults or children. We have lots of statements by vaccine makers and sub-optimal ‘confounded’ observational type research on vaccine driving surges in antibody levels but even that shows the play of original antigenic sin (immune prejudice, immune imprinting on the initial prime or exposure).
Vinaj is superb with that statement above.
See actual paper:

‘Conclusion
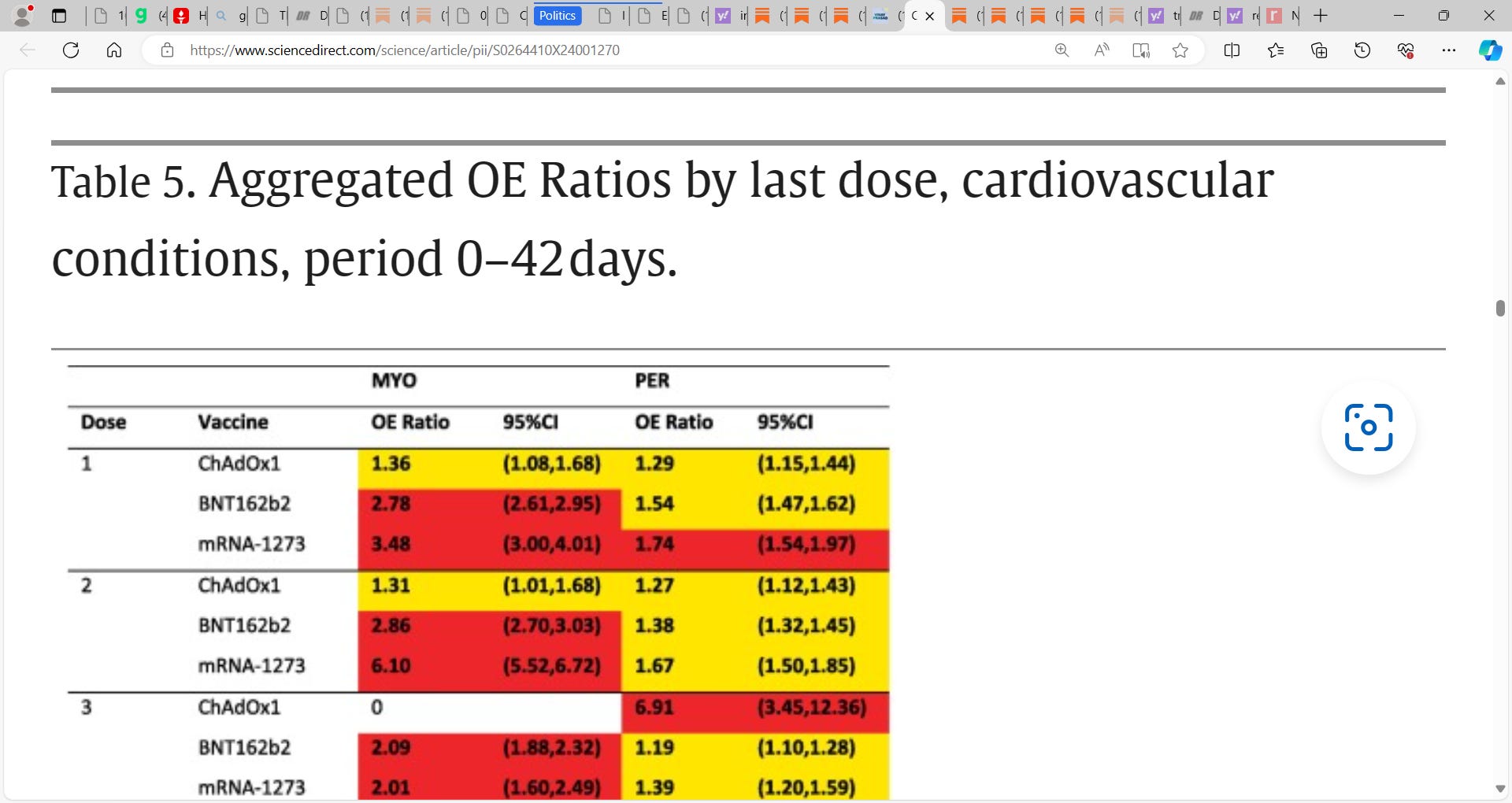
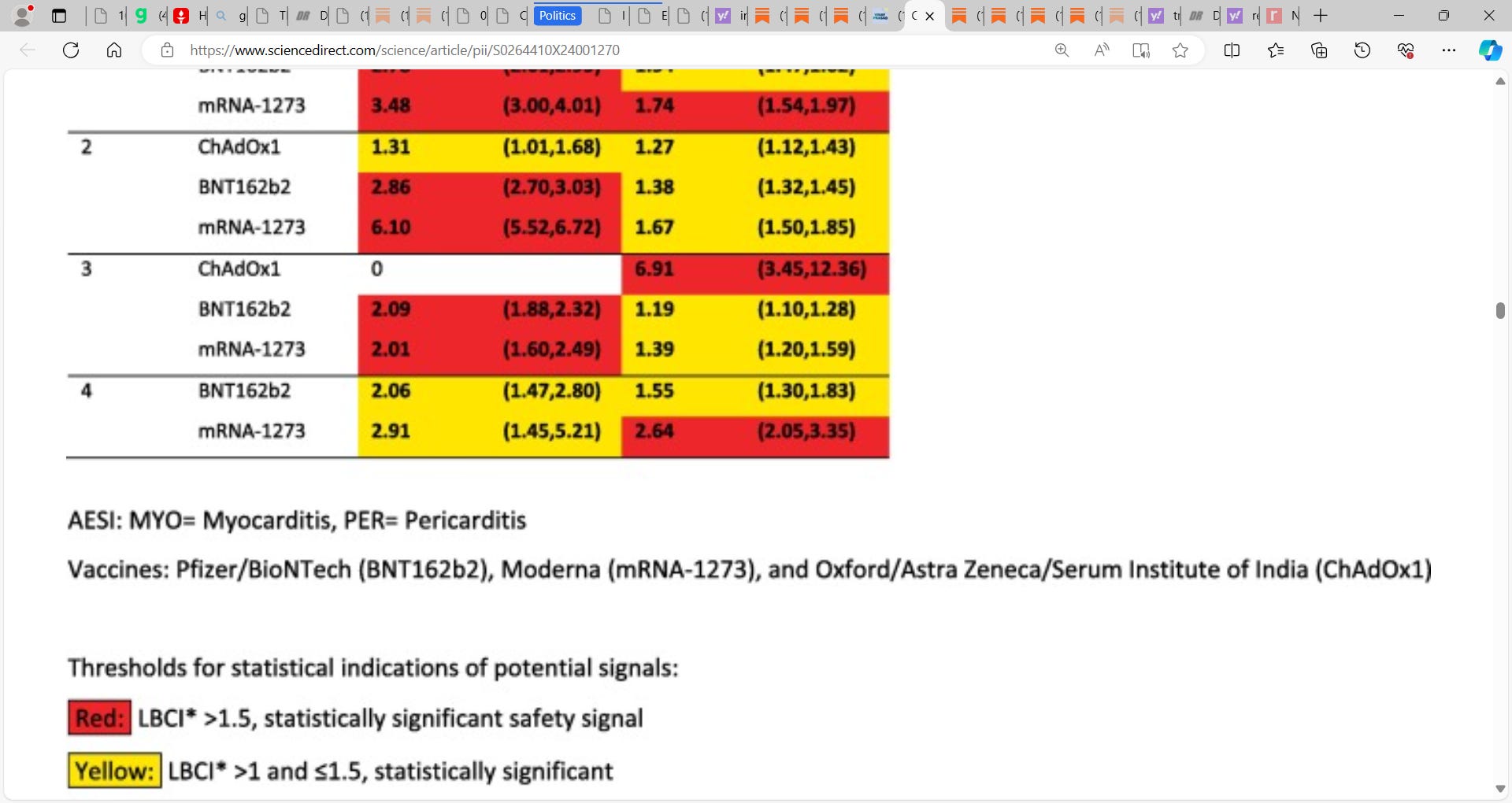
This multi-country analysis confirmed pre-established safety signals for myocarditis, pericarditis, Guillain-Barré syndrome, and cerebral venous sinus thrombosis. Other potential safety signals that require further investigation were identified.’
‘OE ratios with LBCI > 1.5 were observed for Guillain-Barré syndrome (2.49, 95 % CI: 2.15, 2.87) and cerebral venous sinus thrombosis (3.23, 95 % CI: 2.51, 4.09) following the first dose of ChAdOx1 vaccine. Acute disseminated encephalomyelitis showed an OE ratio of 3.78 (95 % CI: 1.52, 7.78) following the first dose of mRNA-1273 vaccine. The OE ratios for myocarditis and pericarditis following BNT162b2, mRNA-1273, and ChAdOx1 were significantly increased with LBCIs > 1.5.’

See more in Vinay’s substack:
“Now let us look at the paper. It has 2 huge limitations. While the denominator (vaccination) is solid, the numerator is weak. It is EHR detected cases of these clinical outcomes across different systems. The biggest problem is that MANY cases of adverse events are likely NOT TO BE CODED. The authors will argue that not coding these events should occur both before and after vaccination and ergo there is no bias (the method looks only at the relative change), but this is incorrect.
It is likely there is differential missing data. That some of these events are missed much more often after vaccination. For instance, the myocarditis due to vaccination is different than myocarditis after a cold. Doctors may not recognize it as such, and be more dismissive. Some diagnoses— like splanchnic vein thrombus— may be increased in populations where you are less likely to consider that diagnosis (young healthy people) and rates of angiography and imaging (needed to diagnose it) may occur less likely. In other words, vaccination could cause a huge increase in abdominal pain from clot in a group of people in whom you would not normally suspect that in— and this analysis assumes doctor’s work it up with the same vigor as they would do for an older, frailer population pre vaccination, and they code it the same. Ergo, all the signals here are, in my view, LOWER bound estimates. I think the truth will be worse.
Second, this analysis does not stratify by demographic group. The increased risk of myocarditis you will see is ACROSS ALL AGES AND GENDERS. That is a big error, when we know it is a problem that plagues young men. Doing this will mask the harm signal. If the increased risk is 3 fold, it may be 100 fold in the demographic that is facing the harm. This is a classic mistake in the field that we have published on.
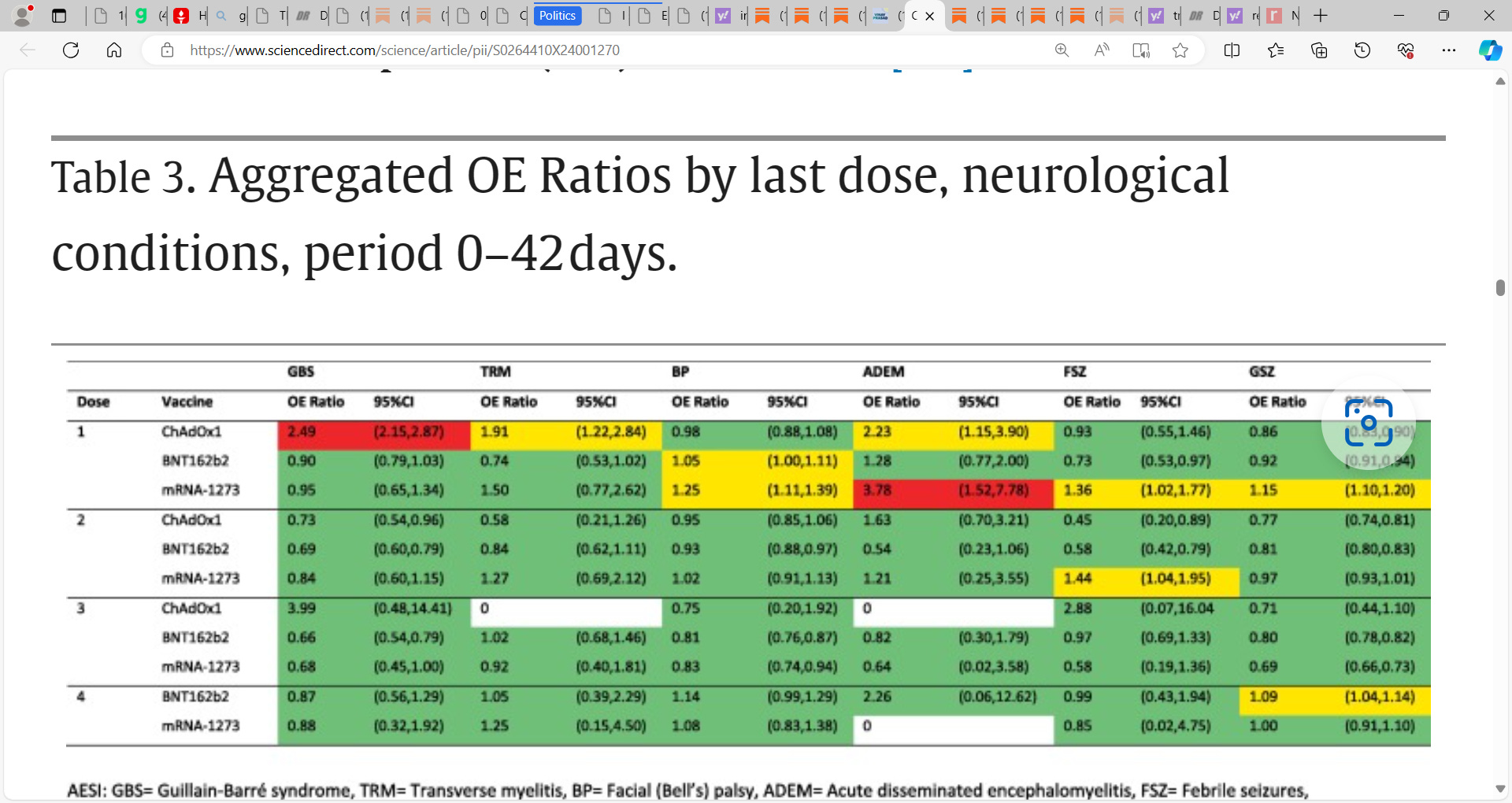
For this reason, every time we see a signal, we should assume it will be worse. And we should think that it doesn’t take much harm to tip the benefit-harm balance in young people, or people who already had COVID. Here is what researchers find.
Everything yellow or red are concerning, significant safety signals.



Increases in cerebral vein clot were known and I wrote about them at the time

Now, we see concerning signals for
Idiopathic thrombocytopenic purpura (ITP)
Febrile seizures
Myocarditis/ pericarditis
Racing heart - SVT
Bells palsy (facial paralysis)
Pulmonary embolism
Acute disseminated encephalomyelitis and more
My overall thoughts. A few years ago a vaccine safety researcher told me she worried tinnitus was linked to COVID19 vaccination. Yet, she had to abandon the project because the political pressure to not find safety signals was too high. We repeatedly see researchers saying that COVID19 is still worse than vaccination, but this is dishonest. Vaccination was worse for young men, and that can be easily shown mathematically.
One mistake these people make is they consider the rate of harms post-covid only among people sick enough to present to the doctor with COVID, but this inflates the rate of harms, as I explained. A second mistake they make is lumping 20 year old men with 80 year old women (this paper also makes this mistake), which minimizes the extent of the harm.
I suspect there is widespread dishonesty in the COVID19 vaccine safety literature. There is a strong political effort to not admit that our vaccination policies harmed some populations, and these were known at the time and not just in retrospect. For this reason, the current paper is deeply concerning. It shows that COVID vaccines are capable of lowering platelets, causing clots, damaging hearts and resulting in partial paralysis.
Imagine a 20 year old man who had covid and was doing fine, and then their college forced them to get the shot, and they suffered bell’s palsy or myocarditis. This man suffered net harm. The mistake was known not in retrospect but at the time. I know because I published a paper saying so in the summer 2021 (before mandates). Public health should be ashamed of itself for harming people in pursuit of a misguided policy goal, and worse, for obfuscating the data, and not admitting error. With time and distance, I suspect most academics will see the wisdom of my argument.”
Great stack Jonathan.
It is good (if not understated), but did you click on his paper which he urged all to read? His introduction reads as follows:
"The COVID-19 vaccine has been a miraculous, life-saving advance, offering staggering efficacy in adults, and was developed with astonishing speed. The time from sequencing the virus to authorizing the first COVID-19 vaccine was so brisk even the optimists appear close-minded."
The mind boggles at this doublethink, so I am afraid I had to point it out:
https://sanityunleashed.substack.com/p/vinay-prasad-wants-it-both-ways