

Massive number of deaths of young US military men & women due to the COVID mRNA technology based gene injection 'vaccine', in other nations too!; Korean military proves recent military recruit's death
Pfizer mRNA vaccine linked, declaring the primary cause of death was determined to be myocarditis, causally-associated with the Pfizer vaccine; sudden deaths under 25 is NOT normal (Choi et al.)

It is critical that the US military and all global militaries investigate each death of their soldiers via autopsies with full histology to ascertain if these sudden deaths are COVID mRNA technology based gene injection related. The fact is that this age group e.g. persons usually 20 to 25 years old should not be dying suddenly, especially if they are fit, strong military personnel.

In this example:
‘The primary cause of death was determined to be myocarditis, causally-associated with the Pfizer vaccine.’
Researchers present a case of a 22-year-old South Korean male military recruit who ‘developed chest pain 5 days after the first dose of the Pfizer mRNA vaccine (mRNA technology) and died 7 hours later. Histological examination of the heart revealed isolated atrial myocarditis, with neutrophil and histiocyte predominance. Immunohistochemical C4d staining revealed scattered single-cell necrosis of myocytes which was not accompanied by inflammatory infiltrates. Extensive contraction band necrosis was observed in the atria and ventricles. There was no evidence of microthrombosis or infection in the heart and other organs.’
‘There were three main histological findings in the heart: 1) myocarditis predominantly involving the atrial wall, with neutrophil and histiocyte predominance; 2) non-inflammatory single-cell necrosis; and 3) diffuse CBN throughout the myocardium, predominantly in the left ventricle. These pathological findings were not evident on macroscopic examination. The only abnormal gross finding was cardiac enlargement, which may have been secondary to hypertension.’
SOURCE:
https://synapse.koreamed.org/articles/1147953?utm_source=substack&utm_medium=email
More detailed description:
‘The deceased was 22-year-old male military recruit. His blood pressure was elevated on physical examination 17 and 7 months before his death (156/94 mmHg and 128/74 mmHg, respectively), but he was otherwise healthy. On June 13, 2021, 5 days after the first dose of BNT162b2 mRNA vaccination, he complained to a colleague of chest pain at 1:00 AM, during a smoke break, and went to bed. At 8:00 AM, he was found unconscious hunched beside the bed. He was taken to an emergency department and was found to have ventricular fibrillation on electrocardiography. Cardiopulmonary resuscitation was performed for two hours, but he could not be resuscitated.
An autopsy was performed 24 hours after his death. The deceased was well-nourished with no visible injuries on external examination. The heart weighed 470 g and had multiple petechiae on its surface. The pericardium was smooth with no fibrin deposition or exudate. The coronary arteries were patent, and the heart valves were unremarkable. The myocardium was of normal thickness and there was no dilation of the atria or ventricles. The myocardium was homogeneously brown with no obvious necrosis or fibrosis. On microscopic examination, diffuse inflammatory infiltration, with neutrophil and histiocyte predominance, was observed within the myocardium (Fig. 1A). Notably, the inflammatory infiltrates were dominant in the atria (Fig. 1A and B), and around the sinoatrial (SA) and atrioventricular (AV) nodes (Fig. 1C), whereas ventricular area displayed minimal or no inflammatory cells (Fig. 1D). Occasional myocyte necrosis or degeneration was found adjacent to the inflammatory infiltrates, without abscess formation or bacterial colonization.
There was also scattered single-cell necrosis of myocytes without accompanying inflammation. Multiple scattered foci of contraction band necrosis (CBN) was identified throughout the myocardium, predominantly in the left ventricle. No other specific pathological changes were found in the lung, liver, kidney, spleen, pancreas, or brain on macroscopic or microscopic examination.’
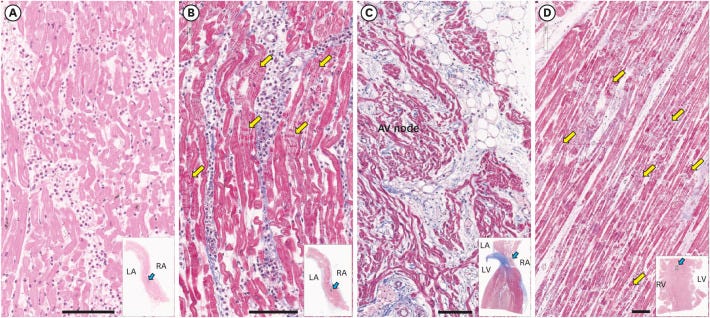

Fig. 1
Histopathology of the heart. (A) Hematoxylin and eosin stains of atrial septum shows massive inflammatory infiltration with neutrophil predominance. (B) The myocytes often show contraction band necrosis (yellow arrows), which were highlighted by Masson's trichrome staining. (C) The atrioventricular node area shows extension of atrial myocarditis to the superficial layer of the node. (D) The ventricular myocardium is free of inflammatory infiltrates, but there are multiple large foci of contraction band necrosis (yellow arrows) particularly in the left ventricular wall and the ventricular septum. Bars represent 100 µm. The blue arrows in insets show where the section was taken from the low magnification views. Hematoxylin and eosin stain was used for the specimen shown in (A) and Masson's trichrome stain was used for the specimen shown in (B-D).
RA = right atrium, LA = left atrium, RV = right ventricle, LV = left ventricle.
The sub clinical myocarditis likely could be as high as 20-30%. Under stress this sub clinical condition becomes clinical. Which is why athletes under stress are dropping. What is the most stressful situation one can be under? Combat! If US troops go boots on the ground there will be catastrophic heart failures occurring. The US has been rendered impotent.
From what I understand the US military department planned and executed the Covid infection globally. They could care less how many US military die from a Covid or vaccine jab infection.
Watch this speech by Sasha Latypova.
https://duckduckgo.com/?q=Sasha+Latypova+speech&t=h_&iax=videos&ia=videos&iai=https%3A%2F%2Fwww.youtube.com%2Fwatch%3Fv%3DIaqHNsj9j-o