

NORWAY and SOUTH AFRICAN Omicron evidence; does Omicron impede our emergence from COVID-19 and change our proposed 15 point plan/steps? No and in fact OMIRCRON tells us COVID is over! DONE!
Two studies, one out of Norway and one out of South Africa tells us OMICRON is infectious, very mild, and that vaccines fail in hitting it, it blows past the immunity; COVID is done!

The data is very clear, that the risk of severe sequelae or death linked to COVID-19 in healthy children is statistical zero and virtually non-existent. The same is for OMICRON variant which presents as very mild illness that is even less than cold like symptoms, IF the child is symptomatic. The risk of death in children from OMICRON is exceedingly rare. This is the data and do not let the media or Fauci or Walensky or CDC or NIH deceive you any longer! Or the irrational, illogical, hysterical, fear porn propaganda complicit media!
We can attribute this to the substantial immunological advantages children have relative to older persons e.g. persons > 50 years of age and certainly for those over 65 who are at greater risk and is the high risk population. The core issue is that vaccine developers did not perform the proper safety studies (follow-up) and thus we have no idea what the future will be post vaccine in children. Children have been spared from COVID and come with natural protections and bypassing these with vaccine could kill our children. I am trying to be as straightforward and honest as possible, to help calm you. No healthy child in the US has died from COVID. This is the data.
Very good recent research by Dowell et al. has helped re-iterate a molecular and biological basis whereby children are so very protected in that children develop robust and sustained cross-reactive spike-specific immune responses to SARS-CoV-2 infection. This has lots to do with prior exposure to common cold coronaviruses that confers robust long-lived protection on children. This supports the prior Brownstone op-ed I wrote (“Dear Pfizer, leave our children alone”, which I have now updated to reflect this Dowell et al. paper) showing a molecular/biological basis as to why children must be considered already vaccinated.
What you should be concerned about is a recent publication by Kostoff et al. (Toxicology Reports, Volume 8, 2021, Pages 1665-1684) that showed 5 deaths in older persons (elderly) due to the vaccine for each life saved from COVID. They reported
“A novel best-case scenario cost-benefit analysis showed very conservatively that there are five times the number of deaths attributable to each inoculation vs those attributable to COVID-19 in the most vulnerable 65+ demographic.”
Your principle role today as a parent is to protect your children from these vaccines, to protect their safety and set this as the hill you are prepared to wage war for them and to die on! The vaccine developers Pfizer et al. and CDC and NIH and Bourla and Francis Collins and Fauci et al. will not stop so you have to defend your children and be prepared to fight with all your very all! Your life came to this moment, it was for this, your entire life, all you are, is for this moment, and it is for your children!
The views expressed here are entirely my own as an academic scientist and does not reflect any institution or other persons. It is based on all I have experienced and learnt across the last near 2 years regarding COVID-19. I can defend my views such as i) asymptomatic transmission remains one of the greatest falsehoods and fallacies of this pandemic and also the issue of ii) recurrent infections also being a fallacy. These are and were very rare and some argue non-existent. I will never say ‘zero’ but I will say ‘statistical zero’ and ‘vanishingly small’ and ‘approaching zero’ to describe these two phenomenon for they were used in my opinion in a duplicitous manner to drive mask use and lockdowns. I can defend this based on the actual science.
Remember, we are dealing with vaccine companies that claimed a 95% efficacy of these vaccines as they sought EUA e.g. Pfizer and Moderna, but they deceived the nation and world for this is relative risk reduction (RRR) figure but what mattered to you is the absolute risk reduction (ARR) and this was actually <1%, in fact, approximately 0.7%.
Incredibly, while Pfizer reported 91% efficacy in their recent publication in NEJM, they reported more deaths in the intervention arm and this is astounding that the media and FDA dismisses this important aspect. There is more harm than good. “During the blinded, placebo-controlled period, 15 participants in the BNT162b2 group and 14 in the placebo group died; during the open-label period, 3 participants in the BNT162b2 group and 2 in the original placebo group who received BNT162b2 after unblinding died. None of these deaths were considered to be related to BNT162b2 by the investigators. Causes of death were balanced between BNT162b2 and placebo groups (Table S4).” (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8461570/). It is important you understand that the trials are unblinded now as placebo was offered to the vaccine group and this means while they say the trial is ongoing (with you as part of the trial), it was effectively over and moot when the placebo received intervention. There is no longer comparative groups and we will not be able to compare groups in the future.
Animal testing was not done and this is a devastating missed step and the FDA has failed in demanding this. Remember, it is in the animal phases of study for SARS-1 studies post SARS-1 (2003), that the animals died post vaccine. Also, there were about 1600 persons in each of the vaccine and placebo arms who were ‘suspected’ but not confirmed. When you model the data with these omissions for both arms and add them back to the ‘confirmed’ data, then the RRR drops dramatically to 19% which is less than the 50% threshold for EUA. The vaccine companies did not include this data as they would have never gotten EUA and I think the FDA knew this and went along. These are key considerations you must keep in mind as you consider these vaccines.
The great FANTASTIC news is that we can shut the COVID virus down in the nose/oral-nasal passage using nasal-oral wash (virucidal wash) e.g. using povidone-iodine (betadine) or hydrogen peroxide, diluted, then swish and spit, do not swallow, and use a Q-tip clean the inner tips of the nostrils and a bit more deeper inside the nostrils. Decontamination of the nose and mouth with direct virucidal therapies/washes is very effective. People breath it in, the virus settles in the nose and it begins to replicate and it has to arrive at a certain threshold to overcome other pathogen in the nose and our own immune system to become a clinical infection. There is a 3 to 5 days window to kill the virus directly. Diluted virucidal therapies/washes is very effective.
What is my view on COVID today, December 31st? The key message is that COVID-19 is done, it is over! It is time we allowed people to make their own decisions about these COVID vaccines and to live their lives as they see fit, based on common sense decisions, taking every-day reasonable safety precautions. It is time all mandates (vaccine, masks, vaccine passports and otherwise) be ended, complete. It is time we allowed early outpatient treatment to be given by doctors. It is very very effective in reducing hospitalization and deaths. It is shameful and reprehensible and I say criminal what governments and doctors have done in terms of early treatment, prohibiting it. No high quality innovative treatments going on, none! It is time for society to open up in full! I also provide a warning in the last paragraph.
Basic epidemiology and immunology will tell you that the massive surge of COVID-19 infections/cases (Omicron variant) would, if all goes true to form, eventually lead to a point where the virus enters an endemic (dynamic equilibrium) state. The Norway data tells us this as to omicron’s mildness. South African data tells us this. Based on all reporting to date, omicron is very mild and non-lethal, and is behaving as nature’s vaccine. It is milder than the common cold and really spells the end of COVID-19 as it has attenuated itself to a place whereby it is very infectious but highly non-lethal.
A very recent South African study (published December 28th) showed decreased severity of disease during the first global omicron variant covid-19 outbreak in a large hospital in Tshwane, South Africa. Researchers compared 466 hospital COVID-19 admissions (14 November 2021 to present) to 3976 prior admissions since 4 May 2020. Researchers reported that deaths and ICU admissions were “4.5% vs 21.3% (p<0.00001), and 1% vs 4.3% (p<0.00001); length of stay was 4.0 days vs 8.8 days; and mean age was 39 years vs 49 years for the Omicron and previous waves respectively.” This led researchers to conclude a “decreased severity of disease in the Omicron driven fourth wave in the City of Tshwane, its first global epicentre.”
Similarly, Brandal et al. reported on an outbreak caused by the SARS-CoV-2 Omicron variant in Norway, November to December 2021. This omicron outbreak followed a Christmas party with 117 attendees in Oslo, Norway. They reported an “attack rate of 74% and most cases developed symptoms. As at 13 December, none have been hospitalized. Most participants were 30-50 years old. Ninety-six percent of them were fully vaccinated.” The overall findings indicated that Omicron was very infections, very mild, and that being vaccinated was ineffective in preventing infection when compared to Delta.
This is very good news and these findings are backed up by animal experiments from multiple independent laboratories that demonstrate weakened (attenuated) very mild lung disease in animals such as rodents, and this mirrors preliminary human clinical data. Wolf (Blaze media) also released a nice summary showing that Omicron is basically an upper respiratory infection/disease and does not go deeper into the lungs. Bentley et al. also looked at the animal model and reported that SARS-CoV-2 Omicron-B.1.1.529 Variant leads to less severe disease than Pango B and Delta variants strains in a mouse model of severe COVID-19. These animal data add to the human data and is potent.
There is even tantalizing evidence recently published (again, preliminary) that Omicron may have jumped from humans to the animal model (mice), derived mutations, and then jumped back to humans. “Our results suggest that the progenitor of Omicron jumped from humans to mice, rapidly accumulated mutations conducive to infecting that host, then jumped back into humans, indicating an inter-species evolutionary trajectory for the Omicron outbreak.” Fascinating and we are studying this publication’s data.
This data is indeed exciting, exceptional, and terrific for with this mild Omicron variant, this will contribute rapidly to population-level herd immunity (natural immunity) (see Figure 1). Natural immunity will work its magic and this is what I and others have been claiming for 2 years now. Step back and allow the healthy population, the low-risk ‘well’ and ‘healthy’ in the population, to handle this pathogen with their strong immune systems (innate and natural immunity), while we properly protect the vulnerable and elderly. Strong protections of the elderly first always, and properly. This view remains unchanged. Moreover, the recent emergence of omicron and its very mild (highly infectious but non-consequential) footprint tells us that COVID-19 is in the final stages and as populations, we should be urgently pushing to begin living our lives again. Omicron in the COVID recovered is being described as mother nature’s booster.
Figure 1 is a critical one for it tells us that the omicron variant drove a rapid increase in infections and cases, but no concomitant hospitalizations and deaths (hospitalizations not shown but the extrapolation can be made). It shows the uncoupling of cases with deaths. Figure 1 also shows us that India and Japan that turned to early treatment and prophylaxis such as hydroxychloroquine and ivermectin, experienced no such rise in cases and no rise in deaths. These have remained flat in spite of OMICRON. I have plotted data as to December 30th 2021. Bottom line, early treatment was the factor (in my opinion) that stopped the escalation in OMICRON in Japan and India, and while South Africa experienced dramatic escalations, the mildness of OMICRON resulted in no appreciable deaths. This is fantastic news! It underscores the potency of early treatment and the mildness, benign nature of OMICRON.
Figure 1: Infections/cases and deaths in South Africa, India, and Japan in the era of OMICRON
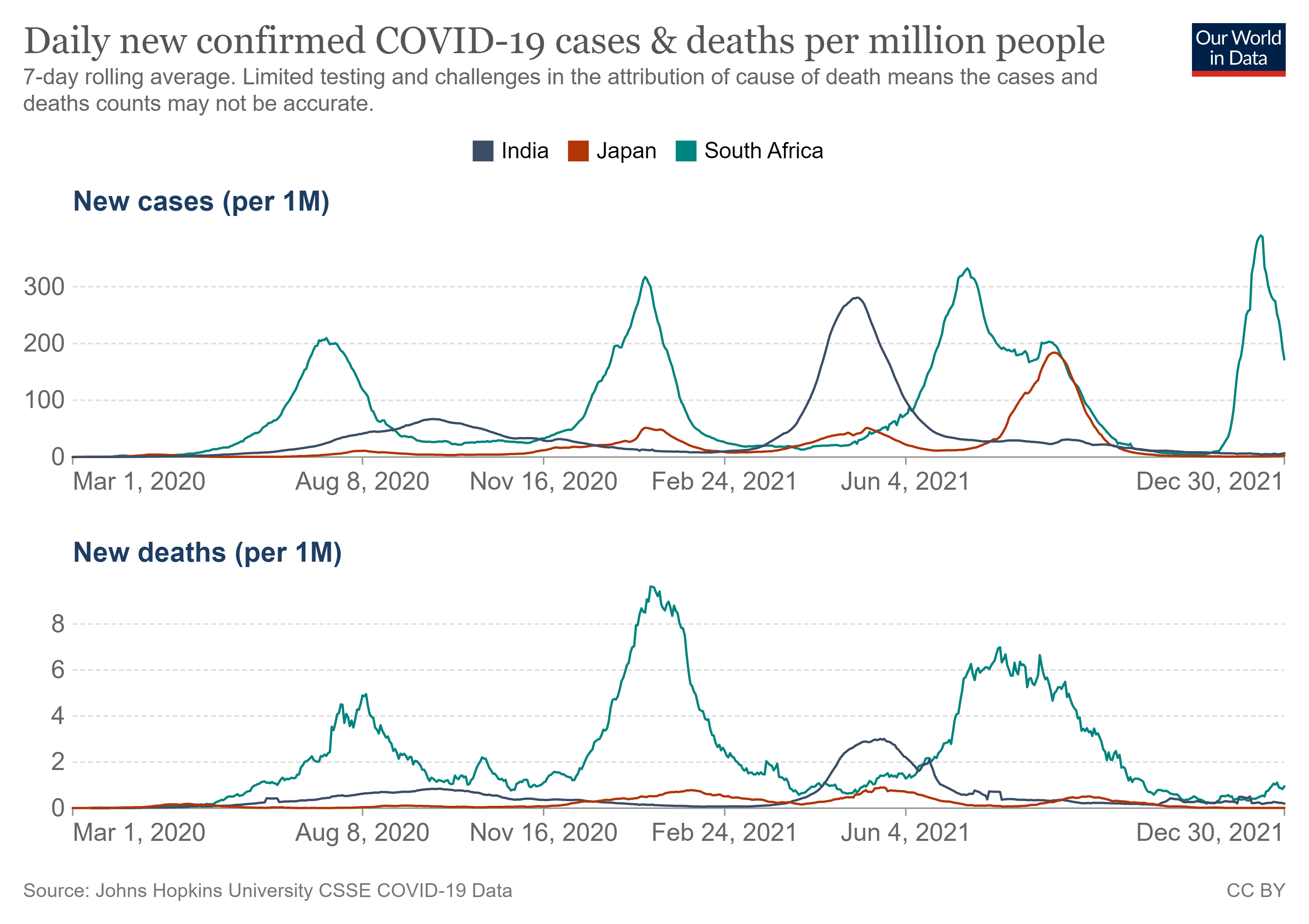
https://ourworldindata.org/coronavirus
Before re-iterating and updating the multiple points to help us moving forward, I turn to Dr. Donald A. Henderson who helped eradicate small-pox and who wrote, “Experience has shown that communities faced with epidemics or other adverse events respond best and with the least anxiety when the normal social functioning of the community is least disrupted. Strong political and public health leadership to provide reassurance and to ensure that needed medical care services are provided are critical elements. If either is seen to be less than optimal, a manageable epidemic could move toward catastrophe.”
Henderson also wrote “The pandemic was such a rapidly spreading disease that it became quickly apparent to U.S. health officials that efforts to stop or slow its spread were futile. Thus, no efforts were made to quarantine individuals or groups, and a deliberate decision was made not to cancel or postpone large meetings such as conferences, church gatherings, or athletic events for the purpose of reducing transmission. No attempt was made to limit travel or to otherwise screen travelers. Emphasis was placed on providing medical care to those who were afflicted and on sustaining the continued functioning of community and health services.”
My suggested 15-point plan is as follows (I tweaked it slightly to reflect OMICRON):
1) Turn off any television or media device that airs the hysterical and irrational often inaccurate media pundits, turn them off, they are destructive in their often spun and deceptive reporting on COVID-19; turn it all off with the drivel they spew now on OMICRON, and the propaganda and fear they seek to drive; it is shocking how much the so-called medical experts push these vaccines on children yet provide no science and data to back up their claims of safety and effectiveness. They routinely point to an undersized study by Pfizer (n=2,200 children) that is designed to miss safety signals e.g. if myocarditis occurs at 1 in 5,000, how could a 2,000 sample sized study detect a case? Moreover, they point to efficacy when Pfizer used antibody levels (immune-bridging?) compared to another age-group, knowing full well that antibody level is not a credible proxy for immunity and is not a ‘patient-important’ outcome like death or hospitalization.
Immediately turn it all off; stop listening to any of the hysterical nonsensical inept COVID Task Force advisors, television medical experts, and government technocrats and bureaucrats. Immediately. We have to be courageous and brave and trust ourselves and our own instincts and decision-making to know what is best for us and our family. Not the government as there is always a price to pay and this price is usually your liberties and freedoms.
Anytime Dr. Anthony Fauci of NIAID or Dr. Rochelle Walensky of CDC or Dr. Francis Collins of NIH is giving a press conference or interview, turn it off. Listen to not one minute of it! Nothing on OMICRON! Listen to or be guided by anything CDC or NIH has to say on COVID-19; nothing! They have earned our distrust in spades as all they have stated the last 2 years have routinely been flat wrong, spun, duplicitous, and meant to mislead and mis-inform. Never ever allow these craven lockdown type lunatics the emergency powers we gave them, ever! NEVER!
Importantly, we must end this era of attacks on dissenters and contrarians, these horrible unfounded attacks and smears on skeptics. We must be open to discrepant viewpoints and immediately return to the place where all views were encouraged and championed. The ‘Enlightenment’. Continuing this way whereby those with varying and discordant views are silenced and cancelled, will spell the end of true academic research and debate. Open discussion and disagreement is the life of science and conformity is its death.
2) Walk through your home and search all of your belongings and throw away every single blue surgical mask and cloth face mask or any of the COVID-19 masks. Any type of face mask, you burn it. None of them have ever been effective and have been harmful, especially for children. Masks have been shown by the overwhelming body of evidence to not effectively work and are very futile and even harmful! Throw them away, but keep one or two for those instances when you are in the company of a high-risk vulnerable person and this is not only for COVID-19, but for all respiratory type pathogen. You make common sense reasonable decisions on this and guide yourself accordingly based on the circulation about you, the ventilation, and the risks. You decide, not nonsensical CDC and NIH technocrats. COVID is done! It is over!
3) Demand that early outpatient (ambulatory) drug treatment is available across society and that doctors and pharmacists can prescribe and dispense it. Make sure to keep your own supply in your private homes and demand that nursing homes and long-term care facilities have a treatment protocol in place and an ample supply. Have early treatment options available not just for this virus but for other respiratory viruses that are more lethal than this and can kill the elderly in nursing homes. Estimates are that 90% or 750,000 Americans would be alive today had doctors stopped the therapeutic nihilism and administered early therapeutics to their sick patients.
4) Allow children to be free again, free, to run and play with their families and friends and no masks and to roll in the grass and hug and laugh and just be free!!!!!!!!!!! Open everything up to them, it is a crime to continue locking children down and restricting them, school or otherwise. Let them live again! COVID is done! It is over!
5) Use common sense precautions and decision making and strongly and properly protect the vulnerable and high-risk and elderly and immunocompromised etc. in society e.g. in your private homes and in nursing homes and long-term care facilities and any such congregated settings. Take reasonable precautions as this pathogen (or similar can be lethal to them, alike influenza). You have done this usually and before, and can do it again. This is your responsibility and not that of the government. You never gave it two minds before because the elderly are ‘invisible’ in the society and ‘out of sight, out of mind”. COVID-19 has shown us that nursing homes can become a tinder box and killing field (outbreaks started usually by infected staff who enter the homes) and they do not take care of the elderly, our parents or grand-parents. Many thousands died due to sub-optimal improper care e.g. in US, Canadian, UK etc. nursing homes and we must hold nursing homes and all involved accountable. Promise we will circle back to them in time for legal accountability for our parents and grandparents who died in their care NEEDLESSLY!
6) Allow the low-risk ‘healthy’ and ‘well’ in the society, the infants, the children, the teens, the young persons, young adults, middle aged persons and even older persons to live normally, with unfettered lives, taking reasonable precautions with common-sense decisions. Trust that their INNATE immune systems will protect them and it usually does and WILL. It is their first line of defense and it is potent. It crushes most pathogen easily. Will do same for COVID and any of its variants. Do not ever lock down the ‘healthy’ and ‘well’ in a society as it causes devastating harms and deaths. COVID-19 is amenable clearly to risk stratification and baseline risk predicts future sequelae. Fundamentally, an age-risk stratified approach is critical. Focused protection. We focus on the vulnerable high-risk and understand that the infants, children, young persons, healthy people are not at risk for severe outcome. The Athenians at the time of the Great Athenian Plague 400 or so BC so 2500 years ago, understood this, and knew that the recovered person takes care of the sick. 2500 years ago! Take note.
7) There must be testing of sera for antibody and also testing for T cell immunity before vaccinating the designated group. This was not done and remains a catastrophic failure. This should have been done before ANY person received these vaccines for it is very risky to vaccinate on top of COVID recovered status (aka natural immunity). If we are vaccinating the higher-risk persons, we do not vaccinate persons who have active infection or who have recovered from infection, the same way if your child gets the measles infection and get the rash and fever etc., you do not then vaccinate them after they have recovered; you send them to school for they are now immune; bullet proof natural immunity and so use that same logic with Covid-19.
8) Stop immediately all mass testing of asymptomatic persons and all isolation and quarantining of asymptomatic persons; it is very harmful and does nothing to reduce the transmission; only ‘test’ and ‘isolate’ symptomatic ‘sick’ persons who are unwell. Persons with a strong clinical suspicion, symptomatic. Do not use the flawed over-cycled PCR 95% ‘false-positive’ test, throw it away. No more testing of asymptomatic well people. If you had COVID, recovered, then never ever go near a test. Ever!
9) Immediately stop all school closures, all lockdowns, all mask mandates, and shelter-in-place policies. They have all failed. Every one of them. My research of over 420 studies and pieces of evidence shows this. Never allow these restrictive policies again for these types of illnesses and if schools as an example, demand masks for your children, then be prepared to remove them from schools and use home schooling etc. No one, not one government, no official, no Task Force, has done a cost-benefit analysis of alternative courses of lockdown and closure actions and this was a catastrophic failure. The crushing harms of these policies were never considered.
10) Implement routine public service announcements (PSAs) on the importance of vitamin D (sun light and supplements) for immune function and not only for COVID-19; also, inform the public using the public health podium on the importance of a healthy lifestyle and body weight (obesity emerged as a super-loaded risk factor for severe COVID).
11) Cease the illogical, irrational, inaccurate, and nonsensical absurdity that Covid-19 vaccine immunity is superior to naturally acquired immunity (or innate immunity) when the science (the body of evidence with actual studies and expert reports) is clear that natural exposure immunity is broad, robust, durable, mature, long-lasting and similar to if not way superior to the narrow, and immature immunity conferred by the Covid vaccines. A recent article by Scott Morefield at the Brownstone Institute reveals the ridiculousness of the CDC and NIH.
12) The vaccine has failed against Delta (and now omicron variant, see refs 34-39)) and so there must be no vaccine passports (or immunity or antibody passports), as these mandates will constrain the rights of citizens under the questionable guise of safety; end any demand for vaccine mandates and this will go a long way as it is crushing society; the vaccines as designed so far do not protect an individual by the provision of “sterilizing immunity.”
By sterilizing immunity we mean that there are neutralizing antibodies and there is no further prospect of either getting infected by the SARS-CoV-2 virus after a vaccination nor of passing along the virus to others; the evidence is very clear that the vaccines do no such thing and have failed especially against the Delta variant whereby even the CDC states that the vaccinated and unvaccinated carry virus and can spread; a recent seminal and transformational Israeli study by Gazit et al. has revealed that natural immunity confers longer lasting and stronger protection against infection, symptomatic disease and hospitalization caused by the Delta variant of SARS-CoV-2, compared to the BNT162b2 two-dose vaccine-induced immunity. Omicron is showing mild ‘less than common cold’ symptoms and is non-lethal based on all reports to date. Infectious but non-lethal and indeed a Christmas gift. The Omicron hysteria and hype is misplaced and this is more propaganda and to drive needless fear.
13) Implement immediate data safety monitoring, ethics committees, and critical event committees to ensure the proper long-term surveillance of the adverse events and deaths that have occurred due to the COVID-19 vaccines.
14) Respect COVID recovered persons natural immunity. Recognize it as similar to and even superior to vaccine immunity. This is immunology 101. Re-educate doctors and scientists who may have not known this or have forgotten this.
15) These COVID-19 vaccines were not properly developed and especially so for safety. A fifteen-year process was boiled down to 4 months and there were corners cut. This is horrendous and severe risk and we just do not know the long-term outcomes. Efficacy remains in serious doubt and we have the evidence that the vaccines have failed on Delta and Omicron, and even negative efficacy. We cannot ‘exclude harms’ and they are contra-indicated for our children. Do not take these vaccines and while I initially thought that they would be applicable to high-risk seniors, the present lack of efficacy and safety concerns has evolved my thinking and I am calling for a pause/hard stop on all COVID vaccines.
We have to assess the safety before proceeding and as such, I also call for no vaccine mandates as there is no difference between the vaccinated and the unvaccinated in terms of harboring virus and transmitting virus. In fact, the former is presenting as more likely to transmit the virus to vulnerable susceptible persons. If you have not taken any of the vaccines, do not take them. If you have taken a dose (or two), do not take any booster. These views are mines and mines alone.
It remains the mass aggressive vaccination while there is massive virus all around us that is driving evolutionary adaptation and natural infection to select more infectious variants. It is the infectious pressure intersecting with sub-optimal vaccine immune pressure that is driving this. If we wanted this to continue for years and for the variants to keep coming, then we should continue vaccinating how we are at present and we should vaccinate children, turning them like adults now, into potential spreaders. Indications are that it is the vaccinated that is potentially spreading pathogen based on the numbers we are seeing in UK etc. among the vaccinated and unvaccinated. We can never tame or calm or stop this virus by using non-sterilizing vaccines for we will never be able to cut the chain of transmission. We would be better to stop this vaccination now. Infections will stop and variants will stop. Natural immunity etc. can bring this to a close but we threaten this with the continued mass vaccination and boosting. It is as we see, driving the emergence of variants.
You have summarized in this article my book The Defeat Of COVID, as well as my later articles here on Substack regarding the hazards and lack of effectiveness of the COVID vaccines. The book has more than 500 peer-reviewed studies to back us up.
I endorse everything my friend Dr Alexander writes here.
I’m the person who first went right out on a limb & predicted that mass vaccination of children would lead to 50X deaths from the vaccines vs deaths FROM SARS-CoV-2.
Note that Sweden & Germany did close monitoring & report zero child deaths FROM covid19. I can’t recall if they had some deaths WITH covid19, but I do remember that there were no child deaths where, in the opinion of the attending physician, the virus was a significant contributor to the death.
Leave the kids alone! Also, all healthy young adults (I mean up to 60 years old or so). As for pregnant women, I can’t tell you how angry & upset this makes me. How have we so quickly forgotten thalidomide? There, we had no potential mechanism for the micromelia. Here, we have several grounds for serious concern (1. Accumulation in ovaries; 2. Raising antibodies which cross-react to some extent to syncytin-1; 3. Thromboembolic & neurological event risks.
Weigh that up against
A. The probability you’ll even encounter the virus again (under 10%, according to Dr McCullough).
B. The probability, if infected, that you’d get really ill &
C. The probability that early treatment will fend off adverse consequences of infection.
Masks, lockdowns, asymptomatic transmission, clinically relevant reinfection & PCR mass testing either don’t work, don’t happen or are untrustworthy.
Innate & acquired immunity, early treatment & getting to good levels of Vitamin D are all strong enough to rely upon.
It’s time for ALL OF US to halt the entire malign circus. Get governments out of our faces. Nobody died & left them in charge. I don’t recognise them as having authority over me.