

P. Polykretis provides an excellent summary of the antigen (spike protein) presentation process in the immunization mechanism of the mRNA/DNA genetic vaccines against COVID-19; shows that every human
cell that intakes the LNPs & translates the viral protein (in case of the mRNA vaccines), or gets infected by adenovirus-based vaccines is recognized as a threat by the immune system and killed


https://onlinelibrary.wiley.com/doi/10.1111/sji.13160
‘The mechanism of ‘traditional’ vaccines consists in inoculating viruses, which have been previously inactivated (e.g. by thermal treatments), or attenuated (e.g. by multiple passages in suboptimal growth conditions).1
Such viruses, which lost the ability to cause acute infection, allow the immune system to recognize them as exogenous pathogens, promoting the production of specific antibodies and memory-T lymphocytes.1
The genetic vaccines against COVID-19 which obtained the authorization for use in the European Union, namely the adenoviral-based vaccines (produced by AstraZeneca and Janssen) and the mRNA vaccines (produced by Pfizer/BioNTech and Moderna), encode genetic information, which enables human cells to produce a viral antigen.
More precisely, the aforementioned vaccines induce the protein synthesis machinery of human cells to translate the spike protein of the viral capsid of SARS-CoV-2.2
Upon its translation by the ribosomes, the spike protein gets processed by the Golgi apparatus and presented to the immune system in two forms: i) as an entire protein, displayed on the cellular membrane, which can be recognized by B cells and T-helper cells (Figure 1A); or ii) in the form of fragments loaded on the major histocompatibility complex I (MHC I), which presents the endogenous antigens to CD8+ T lymphocytes (Figure 1B).
The immune system recognizes the exogenous antigen, initiates the inflammatory response (the immune response is an inflammatory response added by PA) and the subsequent steps leading to the production of specific antibodies by the B cells.2
In human cells, the antigen presentation process is performed by the MHC I and II, and this mechanism is essential for the cell-mediated immunity.3 The MHC I is a protein complex, located on the membrane of all nucleated cells, which presents to CD8+ lymphocytes fragments of endogenous antigens, generated upon the proteasomal degradation of intracellular proteins (Figure 1C).3
This mechanism allows the immune system to constantly screen the proteosynthetic activity of all nucleated cells of the body, in order to detect when a cell is synthesizing viral or mutant proteins. The MHC II is located on the membranes of professional antigen-presenting cells (APCs), such as macrophages, monocytes, B cells and dendritic cells, and it displays fragments of exogenous antigens ingested around the body to CD4+ lymphocytes (Figure 1D).3 In some cases, MHC II molecules can be found even on endothelial cells, as a consequence of inflammatory signals.3 When a CD8+ or CD4+ lymphocyte detects a cell expressing a viral gene (e.g. due to an infection), a mutant gene (e.g. due to cancer) or a foreign gene (e.g. due to a transplant), it binds the MHC activating the immune response that leads to the destruction of the abnormal cell.3
The aforementioned processes are essential for understanding the differences between the ‘traditional’ (eg. chicken and egg model) and the genetic vaccines, in terms of antigen presentation. The ‘traditional’ vaccines generally do not induce human cells to produce viral proteins, and thus, human cells do not expose viral antigens deriving from their proteosynthetic activity. On the contrary, the genetic vaccines against COVID-19 induce human cells to produce the spike protein, relying intrinsically to an autoimmune reaction, extended to all the cells that intake the genetic material and start the protein synthesis.’
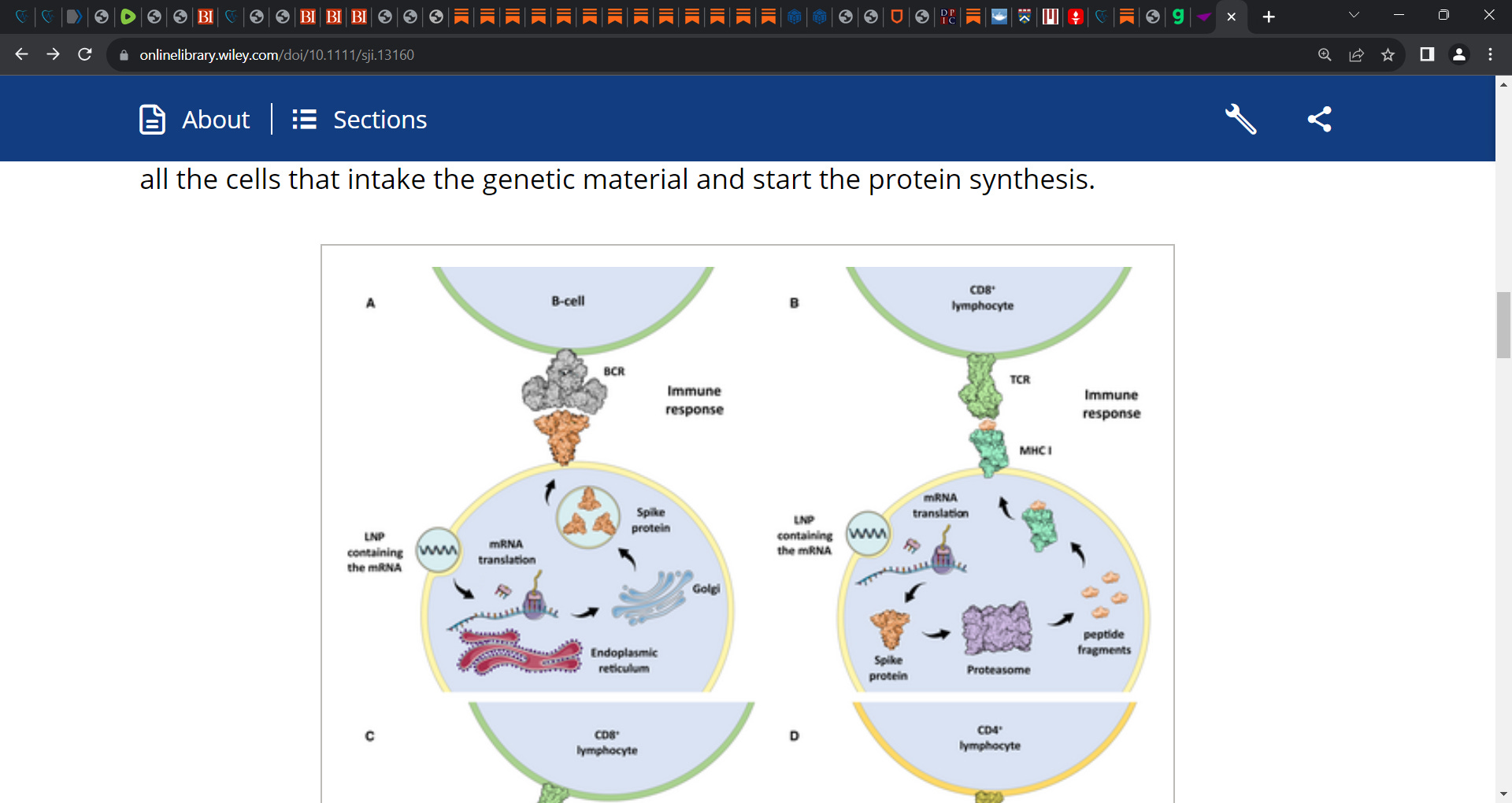
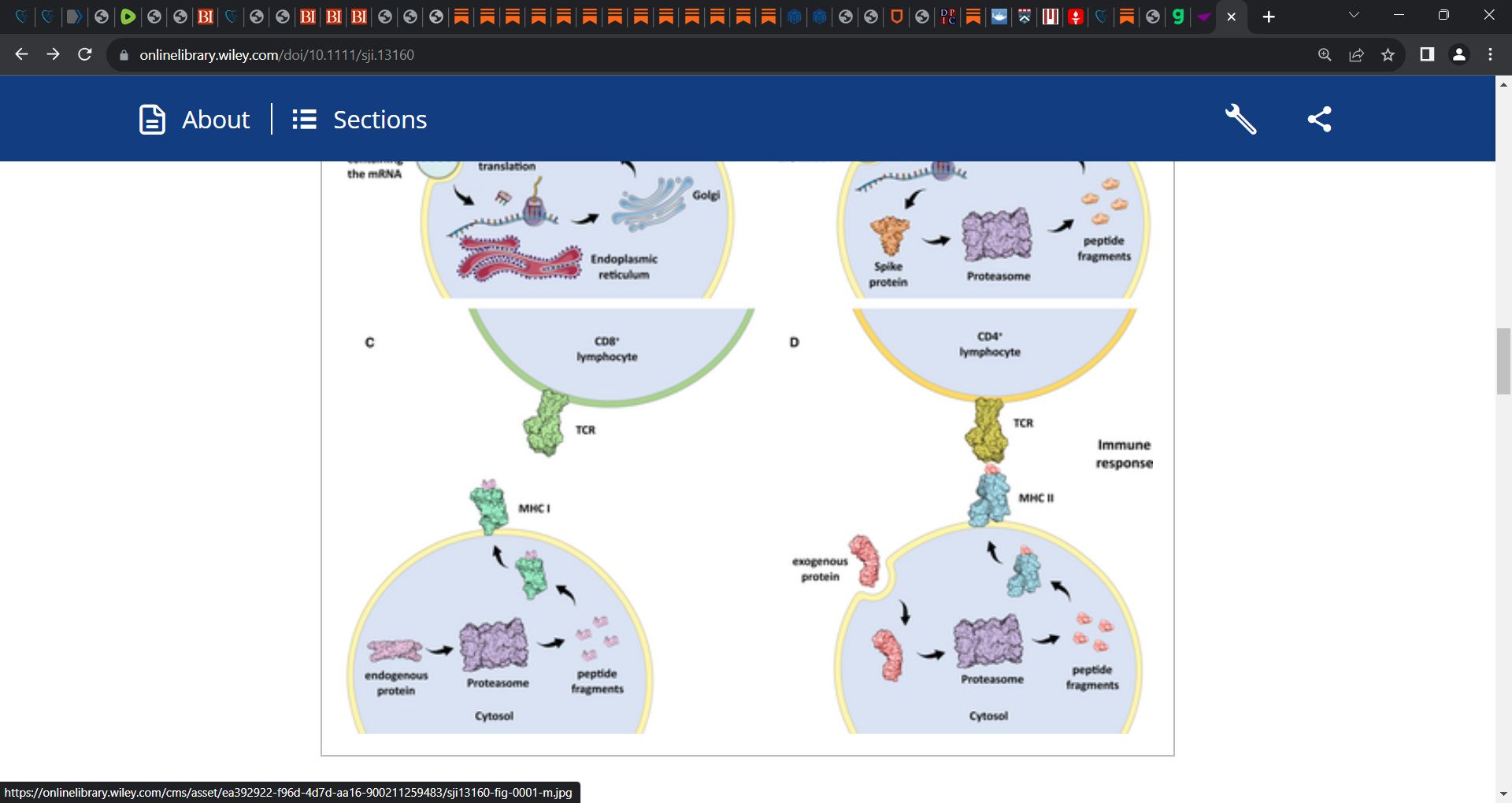
Figure 1: Schematic representation of: (A) A human cell intaking the lipid nanoparticle (LNP) containing the mRNA, translating the SARS-CoV-2 spike protein and presenting it to the B-cell receptor (BCR) of a B cell; (B) a human cell intaking the LNP containing the mRNA, translating the spike protein and presenting it to the T-cell receptor (TCR) of a CD8+ lymphocyte via the MHC I antigen presentation process; (C) MHC I presenting peptides deriving from the proteasomal degradation of endogenous proteins to the T-cell receptor (TCR) of a CD8+ lymphocyte; (D) MHC II presenting peptides deriving from the proteasomal degradation of exogenous proteins to T-cell receptor (TCR) of a CD4+ lymphocyte
Biodistribution studies are fundamental to determine in which tissues and organs an injected compound travels and accumulates. To the author's knowledge, up to now, such evaluation has not been carried out on humans for any of the emergency use approved COVID-19 vaccines. As concerns the Pfizer/BioNTech BNT162b2 vaccine, it is injected into the deltoid muscle, which drains primarily to the axillary lymph nodes. Theoretically, the lipid nanoparticles (LNPs) in which the mRNA is encapsulated should have a very restricted biodistribution, targeting the draining axillary lymph nodes.4 However, a pharmacokinetic study performed by Pfizer for the Japanese regulatory agency shows that the LNPs display an off-target distribution on rodents, accumulating in organs such as the spleen, liver, pituitary gland, thyroid, ovaries and in other tissues.5 Similarly, the results of the European Medicines Agency (EMA) assessment reports show an off-target distribution of the LNPs used by Pfizer/BioNTech and Moderna, in the liver and other organs of rodents.6, 7
Another harmful source of toxicity has proven to be the spike protein itself. A study measured the longitudinal plasma samples collected from recipients of the mRNA-1273 Moderna vaccine.8 The study shows that considerable amounts of spike protein, as well as the cleaved S1 subunit, can be detected in the blood plasma several days after the inoculation. The authors hypothesize that the cellular immune responses triggered by T-cell activation, which occur days after the inoculation, lead to the death of cells presenting the spike protein, releasing it into the bloodstream.8 The fact that the spike protein is released in the bloodstream, involves even the antigen presentation process mediated by the MHC II, due to the intake of the viral protein around the body by the APCs (Figure 1D).
Up to now, more than 1000 peer-reviewed studies evidence a multitude of adverse events in COVID-19 vaccine recipients.9 Such studies report severe adverse reactions following vaccination, including thrombosis, thrombocytopenia, myocarditis, pericarditis, cardiac arrhythmias, nervous system disorders and other alterations. It is noteworthy that several of the aforesaid side effects had already been reported in the confidential post-authorization cumulative analysis released as part of a Freedom of Information Act (FOIA) procedure, which provides data on deaths and adverse events recorded by Pfizer from 14 December 2020 to 28 February 2021.10
In conclusion, it is essential to underline that every human cell that intakes the LNPs and translates the viral protein (in case of the mRNA vaccines), or that gets infected by the adenovirus and expresses and translates the viral protein (in case of the adenovirus-based vaccines), is inevitably recognized as a threat by the immune system and killed (Figure 1).
There are no exceptions to this mechanism. The severity of the resulting damage and the consequences for health depend on the quantity of the cells involved, on the type of tissue and on the strength of the following autoimmune reaction. For instance, if the mRNA contained in the LNPs would get internalized by cardiac myocytes, and such cells would produce the spike protein, the resulting inflammation would likely lead to the necrosis of the myocardium, with an extent proportional to the number of involved cells. Therefore, it is fundamental to perform pharmacokinetic evaluations in humans, in order to determine the exact biodistribution of the vaccines against COVID-19, and thus to identify the possible tissues at threat.’
It's hard to see what good these jabs do, apart from reportedly curing cancer.
Complete Remission of Metastatic Renal Cell Carcinoma after COVID-19 Vaccination
https://www.mdedge.com/fedprac/avaho/article/257524/covid-19-updates/complete-remission-metastatic-renal-cell-carcinoma
Spontaneous tumor regression following COVID-19 vaccination
https://jitc.bmj.com/content/10/3/e004371
I wonder if another mechanism is being overlooked - that maybe the spike protein isn't just being presented on the membrane, but also is breaking free and flooding the bloodstream. I don't think you can account for the spike being so detected in the bloodstream just from the debris of attacked/destroyed cells, and especially for so long after injection. (Even more than a year now it can be detected? The immune system obviously has stood-down on it.). What's the quantity of that detection? Has than been looked at? In the early days of the movement, that was a common supposition as I recall - the spike (I think) flooding the bloodstream and acting like razor blades to the arteries and capillaries and so forth. And perhaps - just me wondering out loud here - maybe it was even engineered to be weakly attached to the membrane, so that it would release and be attacked in the bloodstream, rather than the presenting cells being attacked?