

Pfizer mRNA gene therapy injection & giant coronary aneurysm in a 5 year-old child: did this child cheat death while Grant Wahl died? Did Pfizer vaxx cause child's coronary aneurysm & Wahl's death?
Khadija et al: "Multiple MIS-C Readmissions and Giant Coronary Aneurysm After COVID-19 Illness and Vaccination: A Case Report"; the patient’s care team decided against further COVID-19 vaccination

Very disturbing reporting is emerging whereby the mRNA injections may be causing weakening of the coronary vessel walls including the key aorta vessel, with devastating life-ending consequences.
Let us focus on this very troubling case of a 5-year old boy who presented with MIS-C symptoms 55 days after COVID-19 illness and 15 days after being in receipt of his first Pfizer (BNT162b2) COVID-19 injection (so called ‘vaccination’).
Firstly, while a decision is to be made by parents and the child’s doctor, based on the full body of evidence thus far, there should have been no COVID gene injection shot in a 5 year old healthy child. No child. None! There is no clinical basis for this and there is no medical or clinical research to substantiate this action. No clinical trial exists to show that these COVID gene injections confer any benefit to such low-risk (near zero) children. There is statistical zero risk of severe outcome or death in children from COVID in February 2020 and still today December 2022. Stanford’s Ioannides reported that the risk in persons 0-19 years is approximately 0.0003% and we also know the risk in children 0-10 years old is 0.000%. We have found no healthy child (Makary et al.) in the US for the last 3 years of COVID, for the entire period, who has died of COVID infection. Not one! The same in many global nations who are reporting honestly and fully.
‘This is the only such reported case of a patient who was admitted 3 times for MIS-C complications after COVID-19 vaccination.’ This case raises many questions including how wide spread is this or how widespread it could it get?
This is a healthy child by all accounts and the evidence is building that these mRNA injections can cause coronary type aneurysms including giant cell arteritis. Does the mRNA injections cause weakening of the coronary vessel walls including the key aorta vessel e.g. increased risk of vessel wall bulging due to the mRNA injection vaccine and consequent aortic dissection or full rupture whereby blood rushes through the tear and the end result is potential death (though there is a chance of survival if promptly treated))?
Are these aortic type aneurysms likely due to the COVID gene injection manufactured spike proteins and as a consequence, the then immune system (lymphocyte) attack on the aortic vessel walls? We will discuss this more below.
Yet I laid out my case (substack below) why the COVID gene therapy injection may have likely killed Grant Wahl and may have killed this 5 year old child. The medical management may have been optimal and saved the life and especially the decision to not have any more shots. Certainly not until the crisis resolved.
Before proceeding to this tragic child’s case, see my prior substack on Grant Wahl’s sudden tragic death and the case I laid out to show that it is more than likely due to the mRNA COVID gene injection:
Now back to this 5-year old child’s situation. Overall, I find the reporting in the journal still skewed toward supporting the COVID gene injection (en toto) which as you know, I do not. These journals continue to report very devastating findings yet still go onto conclude that the vaccine is ‘safe and effective’ and use language to suggest this. This is a major problem for the population/reader is being deceived and misled really with propaganda:
SOURCE:
Here is a report on the case of a 5-year-old boy with onset of MIS-C symptoms 55 days after acute COVID-19 illness and 15 days after receiving the first dose of BNT162b2 (Pfizer-BioNTech COVID-19 vaccine) who had recrudescence of MIS-C requiring multiple readmissions associated with significant coronary artery dilation.’
‘A 5-year-old boy had onset of MIS-C symptoms 55 days after COVID-19 illness and 15 days after receiving his first BNT162b2 COVID-19 vaccination. He was admitted 3 times for MIS-C, and twice after his steroid dose was tapered. On his initial admission, he was given intravenous immunoglobulin and steroids. During his second admission, new, moderate coronary dilation was noted, and he was treated with intravenous immunoglobulin and steroids. At his last admission, worsening coronary dilation was noted, and he was treated with infliximab and steroids. During follow-up, he had improvement in his coronary artery dilatation. However, his inflammatory markers increased after steroid wean, and his steroid taper was further extended, after which time his inflammatory markers improved. This is the only such reported case of a patient who was admitted 3 times for MIS-C complications after COVID-19 vaccination.
MIS-C rarely involves delayed giant coronary aneurysms, multiple readmissions, or occurrence after COVID-19 vaccination. Whether our patient’s COVID-19 vaccine 6 weeks after COVID-19 illness contributed to his MIS-C is unknown. After consultation with the CDC-funded Clinical Immunization Safety Assessment Project, the patient’s care team decided against further COVID-19 vaccination until at least 3 months post normalization of inflammatory markers.’
How does this happen? Is there any research or putative explanation? Dr. Sucharit Bhakdi, MD and his team have written about findings to help explain this and we are trying to connect the dots of Grant Wahl’s death as well as this situation in this 5-year old child. The reporting below is a potential explanation involving attack by one’s very own immune system on the cardiovascular vessel walls (key players are the endothelial layer (and will have to be the glycocalyx) and the killer type lymphocytes), and represents at least in part, the underlying mechanics of this disaster:
i)Endothelial stripping and destruction of a small blood vessel after vaccination
‘We now turn to the evidence of immune attack on the endothelial cells which produce the spike protein. On the left, a normal venule, delimited by an intact endothelium and containing some red blood cells and few white blood cells (stained blue) inside.
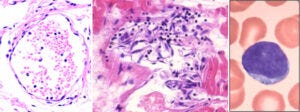
The image on at the centre shows a venule that is being attacked and destroyed by the immune system. The outline is already dissolving, and the spindle-shaped (and swollen) endothelial cells have peeled off from the vessel wall. Furthermore, we see lymphocytes—the small cells with dark, round nuclei and with very little cytoplasm around them; a single lymphocyte (at much higher magnification) is shown on the right.
Lymphocytes are the backbone of the specific immune system—whenever antigens are recognized and antibodies are produced, this is done by lymphocytes. Also among the lymphocytes we find cytotoxic T cells and natural killer cells, which serve to kill virus-infected cells—or ones that look to them as if infected, because they have been forced to produce a viral protein by a so-called vaccine.
A crucial function of the endothelium is to prevent blood clotting. Thus, if the endothelium is damaged, as it is in this picture, and the tissues beyond it make contact with the blood, this will automatically set off blood clotting.
ii)A crack in the wall of the aorta, lined by clusters of lymphocytes, leading to aortic rupture

On the left, a section through the wall of an aorta. This picture is taken at an even lower magnification than the one before; the lymphocytes now appear as just a cloud of tiny blue specks. To the left of this blue cloud, we see a vertical crack running through the tissue. Such a crack is also visible macroscopically in the excised specimen of an aorta shown on the right.
The aorta is the largest blood vessel of the body. It receives the highly pressurized blood ejected by the left ventricle of the heart, and it is thus exposed to intense mechanical stress. If the wall of the aorta is weakened by inflammation, as it is here, then it may crack and rupture. Aortic rupture is normally quite rare, but Prof. Burkhardt found multiple cases in his limited number of autopsies. Some of the affected aortas were also shown to have expressed the spike protein.’
Dear Readers,
I also embed this short piece on The Wellness Company and The UNITY Project.
First, The Wellness Company.

I am proud to announce a unique partnership with The Wellness Company and everyone who believes in medical freedom. My dear and esteemed colleagues Dr. Peter McCullough and Dr. Harvey Risch are also in partnership with The Wellness Company which provides telemedicine services for long-haul COVID, vaccine injury, and medical exemptions along with supplements and products that are fully aligned with our values. This support for The Wellness Company stems from the sub-optimal medical care and response that we experienced throughout the pandemic. It became apparent that there are many glaring gaps in our healthcare system and people were not properly treated. Thus, the pivot by us to support The Wellness Company. Take a stand against a broken healthcare delivery system with a membership in The Wellness Company, which directly funds our fight against medical tyranny. Click here The Wellness Company for more information.
I also provide scientific support to The UNITY Project out of California. A magical organization for good. I support this tremendous initiative with some fine colleagues who have been warriors in the fight against all the wrongs in COVID. The UNITY Project aligns with my core values for it is very fierce in its fight to protect children from the danger of the largely safety untested COVID gene injection (The Unity Project Formed by Concerned Parents to Coordinate Opposition to California's K-12 COVID-19 Vaccination Mandate).
“Pre morbidities - no.” How horrible. Previously HEALTHY child. What for??? Stupid parents. Poor child so unlucky to be born to wrong parents.
These aortic aneurysms are probably due to the jab manufactured spike proteins and the resulting immune system attack to the aortic walls.
“The spike protein is then expressed; some molecules are fragmented and presented on the cell surface by a special carrier protein (MHC1). This causes the endothelial cells to be attacked by cytotoxic T-cells. Destroyed endothelial cells slough off, facilitating leakage of vaccine particles into the adjacent tissues. This also exposes the deeper layers of the vessel wall to the blood, which triggers thrombocyte aggregation and blood clotting.” [1]
“10. A crack in the wall of the aorta, lined by clusters of lymphocytes, leading to aortic rupture” [2]
References:
1. https://doctors4covidethics.org/gene-based-vaccination-quo-vadis/
2. https://doctors4covidethics.org/vascular-and-organ-damage-induced-by-mrna-vaccines-irrefutable-proof-of-causality/