

Revisiting FDA's Vaccines and Related Biological Products Advisory Committee Meeting June 15, 2022: FDA Briefing Document: I wish to rend us how catastrophic, illogical, specious; WALGREENS data
FDA's decision is/was & then the CDC's is wrong, in vaccinating children 6 months through 4 years of age who bring near zero risk with a vaccine that is ineffective, harmful, & provides no benefit

SOURCE:
Vaccines and Related Biological Products Advisory Committee Meeting June 15, 2022
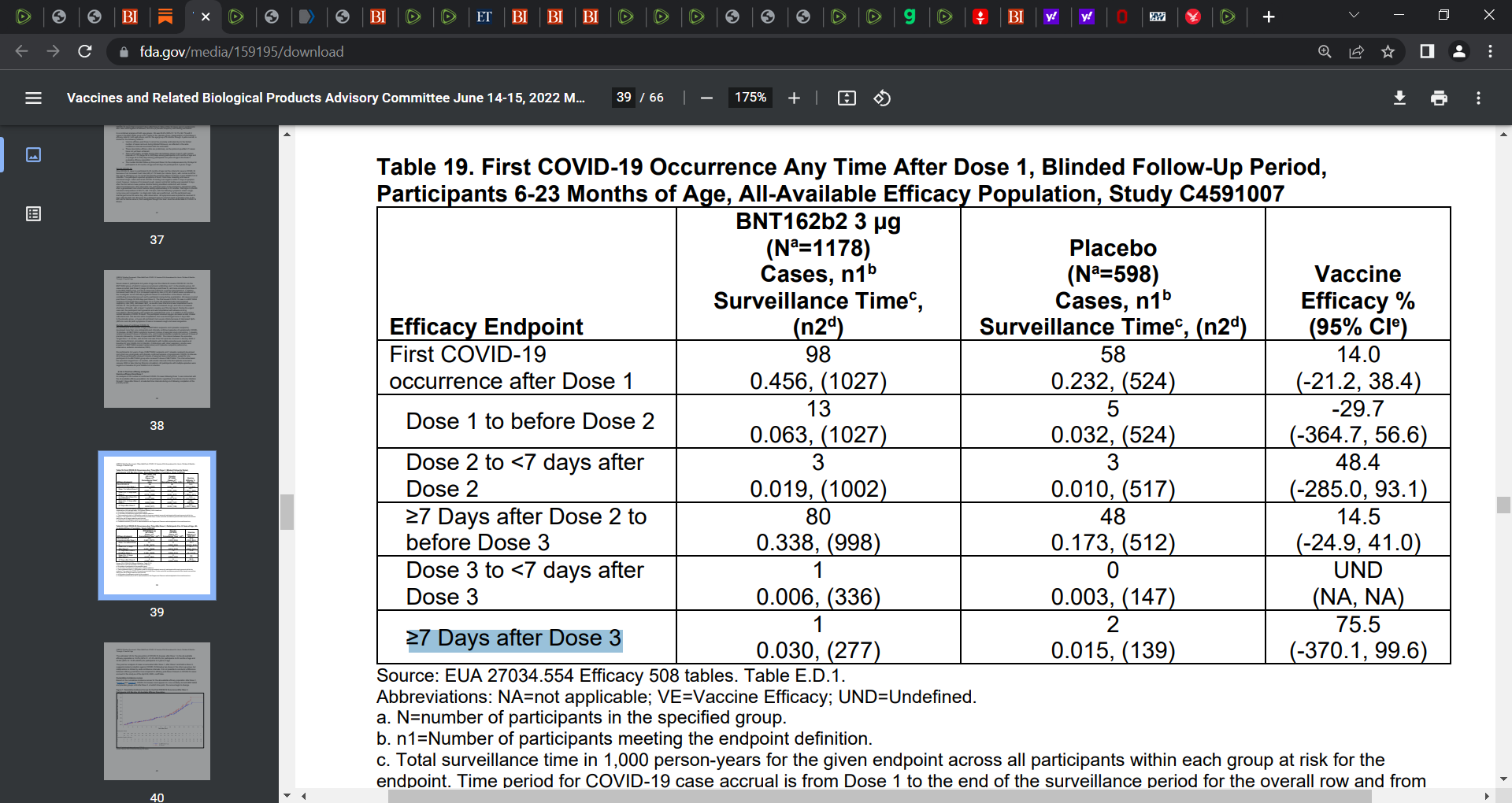
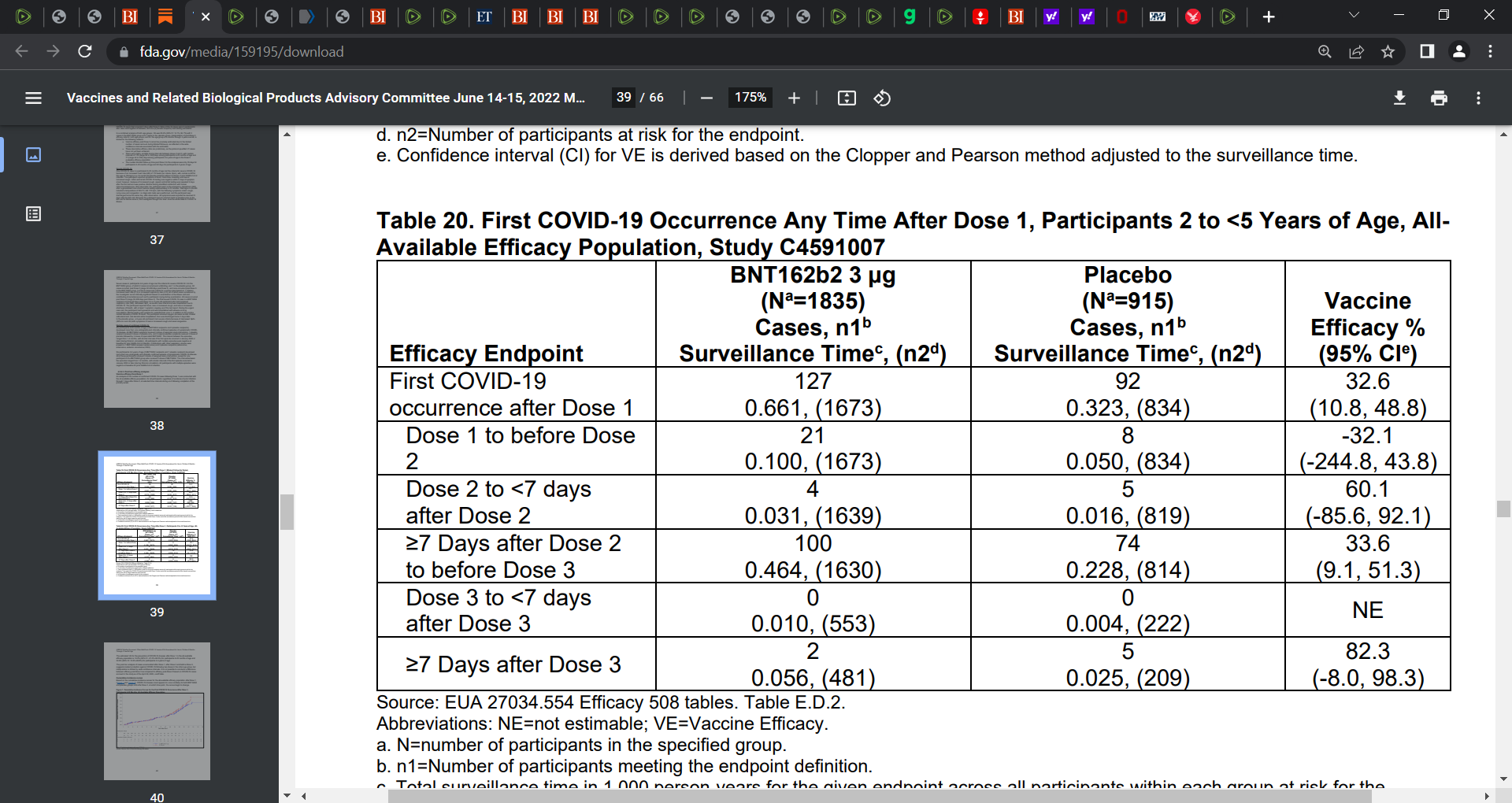
Again, pay attention to page 39, tables 19 and 20
Pay attention to the vaccine efficacy that is negative, the very insanely wide 95% confidence intervals that go to the moon and back, and the small events e.g. 3 Table 19, ≥7 Days after Dose 3.
Pay attention to Table 19, second row, dose 1 to before dose 2, the vaccine efficacy is -29.7%, and look at the insane 95% confidence intervals, spanning hell and back. I wrote about this prior but wished to again. Same in Table 20.
2. SOURCE:
“During September–December 2021, overall seroprevalence increased by 0.9–1.9 percentage points per 4-week period. During December 2021–February 2022, overall U.S. seroprevalence increased from 33.5% (95% CI = 33.1–34.0) to 57.7% (95% CI = 57.1–58.3). Over the same period, seroprevalence increased from 44.2% (95% CI = 42.8–45.8) to 75.2% (95% CI = 73.6–76.8) among children aged 0–11 years and from 45.6% (95% CI = 44.4–46.9) to 74.2% (95% CI = 72.8–75.5) among persons aged 12–17 years (Figure).”
Yet, this was in February 2022, and we are now in June 2022 and Omicron has proliferated and this seroprevalence is likely 90% now. Thus why would children in these age groups need this injection? They largely (most if not all) have natural immunity by CDC’s own report.
3.SOURCE:
Covid-19 Boosters — Where from Here?
Offit writes: “In addition, because boosters are not risk-free, we need to clarify which groups most benefit. For example, boys and men between 16 and 29 years of age are at increased risk for myocarditis caused by mRNA vaccines.10 And all age groups are at risk for the theoretical problem of an “original antigenic sin” — a decreased ability to respond to a new immunogen because the immune system has locked onto the original immunogen.”
Offit raises the issue of original antigenic sin here (OAS, I renamed mortal antigenic sin given the imprinting, priming, or prejudice to the immune response is life-long to that antigen or similar) and also that there is increased risk of myocarditis in young males due to mRNA shots.
SOURCE:
Witberg et al.: Myocarditis after Covid-19 Vaccination in a Large Health Care Organization
4.SOURCE:
Four vaccine adverse events reporting systems show massive numbers of deaths and adverse outcomes due to the COVID injections.
5.
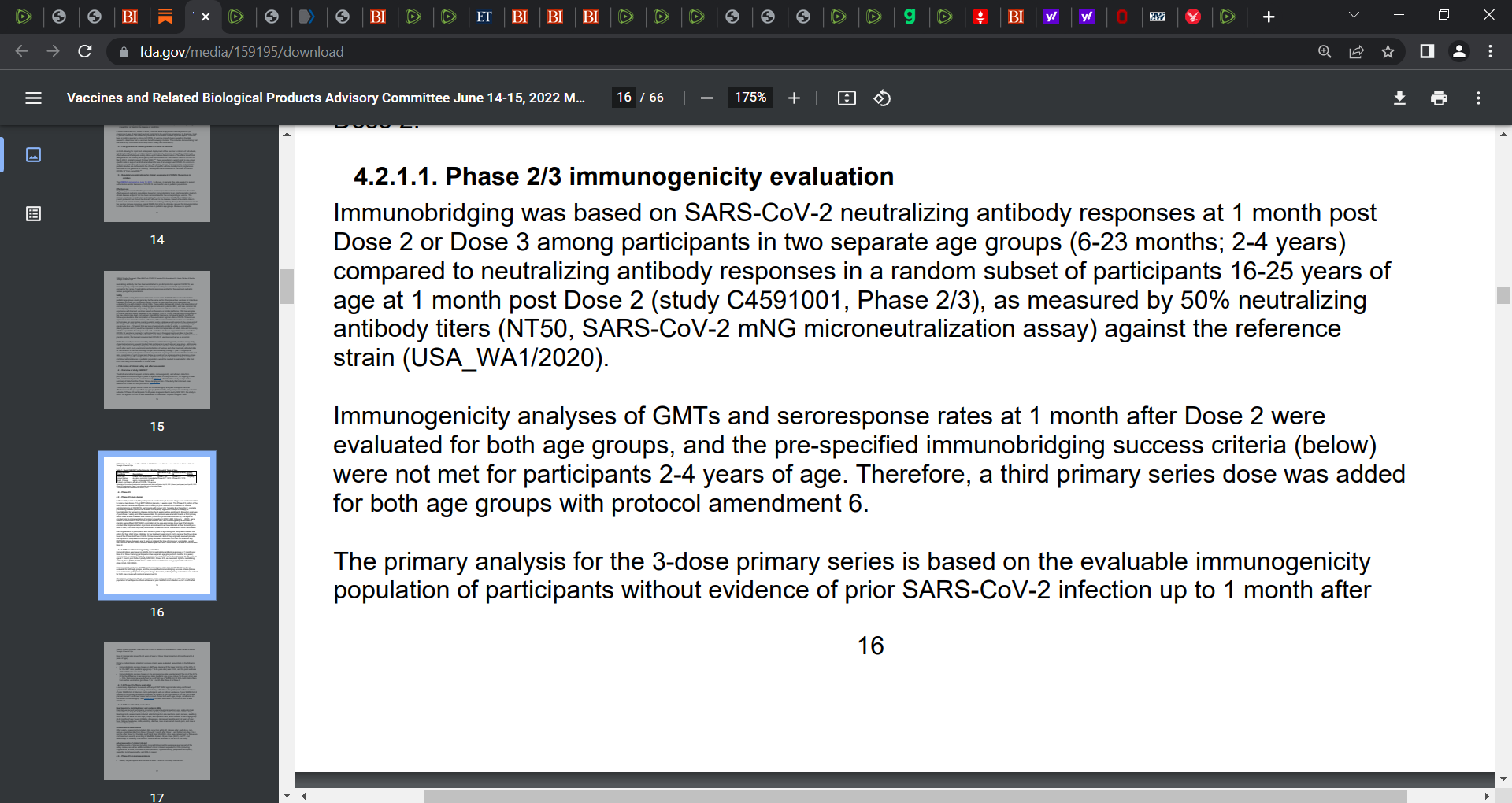
4,526 children were included in the study in kids aged 6 months to 4 years, yet thousands, well over 3,000 were excluded from analysis. Why? There is no explanation of why and this is a serious red flag as to data and study corruption. Why the the few hundred included? Only those. What was the selection criteria? They used samples (blood) from approximately 225 children, not the 4,500 odd children 6 months to 4 years (5%). This is called the immunogenicity population.
The comparative portion was just as insane for they compared the antibody levels in the kids (225) to the antibody levels in under 200 persons aged 16 - 25 years old and we are not told how and why this group of 16 - 25 years olds. How was it composed? Proper research is never conducted in this manner and these drug companies have made up research methods on the go and the FDA has not sanctioned them. They go on to claim success as long as the antibody levels are similar. Is this some bad dream?
Why no hard patient-important outcomes such as death or hospitalization or infection? What is immuno-bridging as this seems a very problematic sub-optimal research design method as well as why are antibodies the outcomes of interest? What value is that as we know it is meaningless in this context? Antibody levels are not a proper or accurate measure or even proxy of immunity. Why were children from the same trial not the control group? Why compare to persons (adults 16 to 25 years old) in another study? This makes no sense and suggests strong manipulation of the study and data.
This immuno-bridging is nonsensical, absurd, junk pseudo-science.
6.
By unblinding the studies as they did, and as such by vaccinating the placebo groups, means that Pfizer and Moderna know that the studies ended on the spot. There are no viable comparative groups anymore of vaccine versus no vaccine. All are vaccinated. The FDA and CDC knows this too, they are all defrauding the population. They know we cannot collect and compare any effectiveness or safety data anymore.
7.
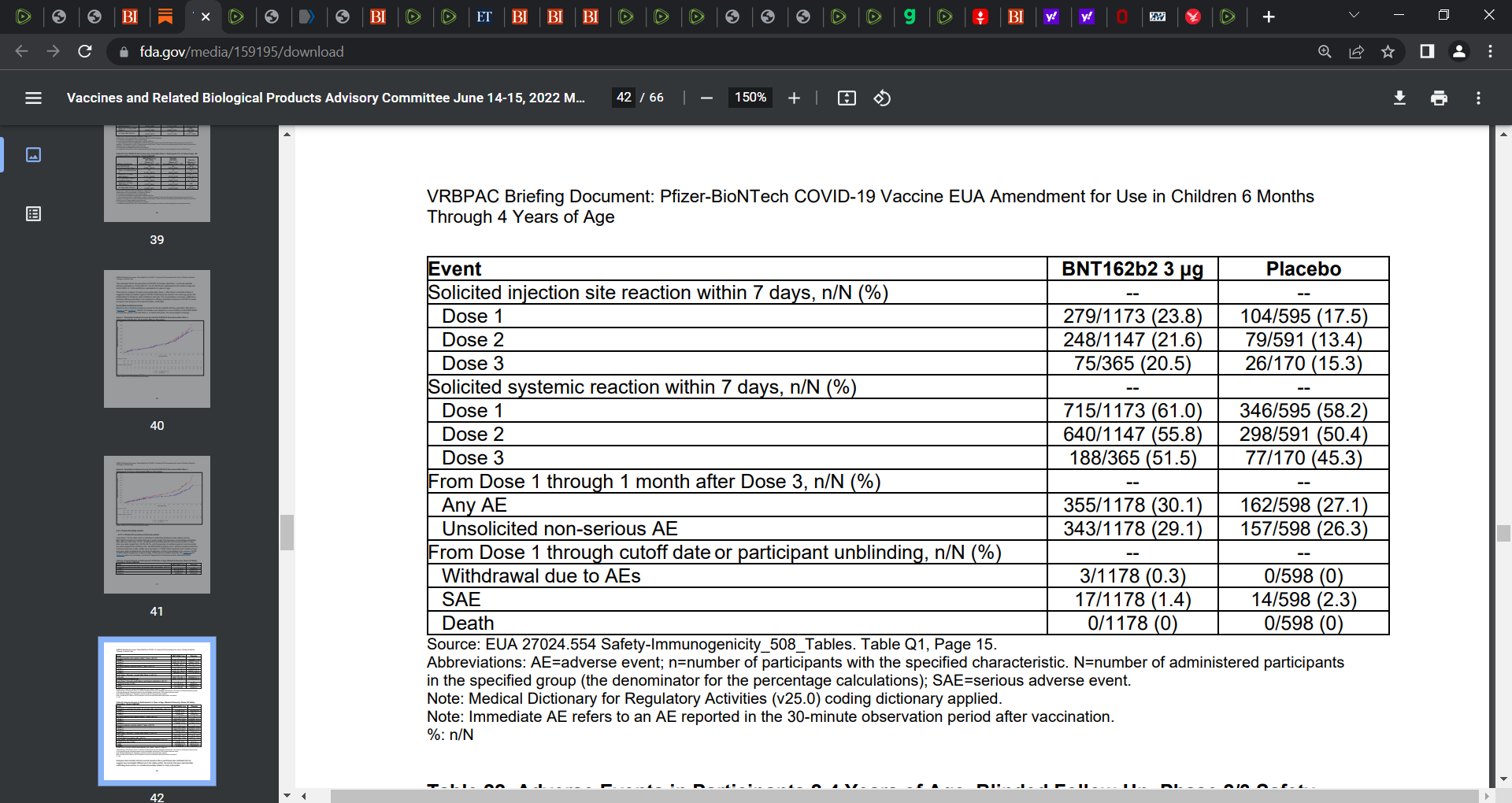
Look at Table 21 on page 41, showing that 61% and 55.8% had solicited systemic reaction (adverse events) within 7 days of doses 1 and 2 respectively:
WALGREENS:
Main dominant sub-variants of Omicron e.g. BA.2.12.1 is at 50%

Positive rate to 21st June 2022:
As you see, 2 and 3 doses (> 5 months) continue to precede the highest rates

I'm not a doctor or epidemiologist, but if the studies you cite were unblinded, then they aren't really true double-blind studies are they? So they would not be the "gold standard" Fauci used to talk about, right? So how can they be considered acceptable as evidence? It seems to me there may be a serious procedural error that some lawyers could use to get a court to issue a temporary restraining order on FDA approval...process violations aren't really a matter of subjective opinion!
How much do you wanna bet that Wen Paid for normal saline to go into her kids arms. Using the lot numbers on the , disposed of, vax veil to cover up.