
URGENT: BA.5 subvariant/clade that has emerged we warned was going to be due to the COVID mRNA injection; it has come to pass; it is more infectious and now more serious symptoms in vulnerables
URGENT: BA.5 subvariant/clade that has emerged we warned was going to be due to the COVID mRNA injection; it has come to pass; it is more infectious and now more serious symptoms in vulnerables
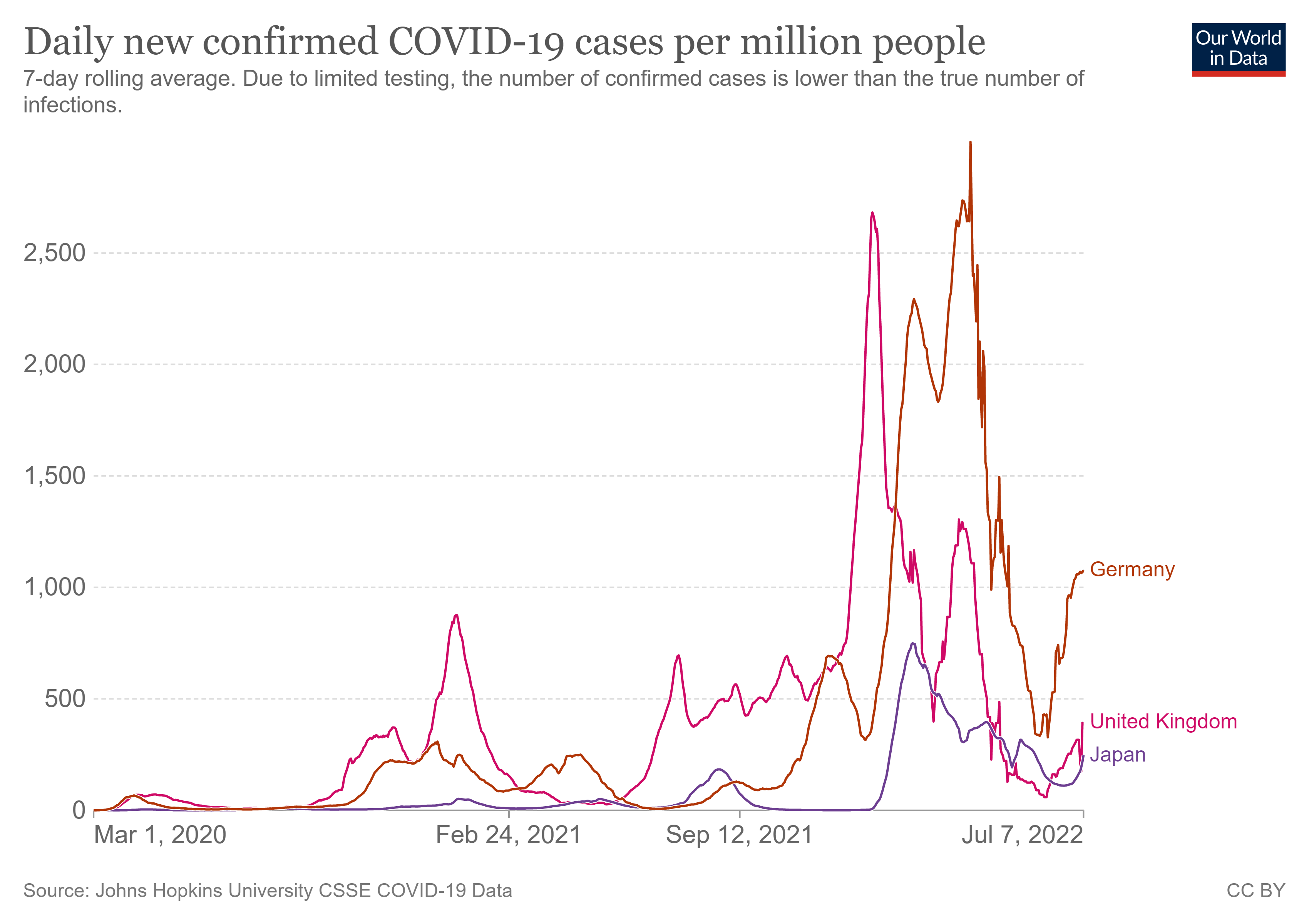
What is needed is early treatment, if hospital CEOs and doctors and government officials did not steal the PEP COVID money, then hospitals are already geared, won't be overwhelmed; GRAPHS

I am trying to explain it simply:
It is the COVID injection itself, the mRNA injections that are non-neutralizing now and are placing sub-optimal immune pressure on the virus’s spike and driving infectious variants one after the other, and we fear soon (now), emerging are variants that would cause severe symptoms in the lower lungs (lower respiratory tract). It is not the virus, it is the injection, the vaccine itself that is making the virus more infectious to the vaccinated population. It is the injection and it is illogical and reckless and dangerous to respond with more vaccine and booster. It is going to be lethal.
The COVID injection has long moved from being neutralizing to the target antigen, which is the one target, the spike protein spicule that sits on the ball of the virus (you know what I am referring to). It is a non-neutralizing injection today, has been for a while now, does not sterilize the virus and that means it does not stop infection, replication, transmission, confer immunity.
The reality is that within a highly vaccinated, in a well-mixed population, vaccinated persons should be regarded as asymptomatic reservoirs for transmission of new, and highly infectious COVID immune escape variants and also other highly infectious diseases to the balance of the population. We were warning of this disaster yet the CDC and NIH and FDA and Bourla (Pfizer) and Bancel (Moderna) are not listening. They are now coming for the children. You as parents better be prepared to lay your life down in protection of your kids. In this. Healthy kids will die due to these injections, will be severely harmed. Their innate immune systems are at risk of subversion.
We are warning that the consequential enhanced viral transmission rate has the potential to initiate new pandemics and these are not only of new, highly infectious, and antigenically shifted COVID variants (presenting of sufficiently different variants) but there is also the risk we argue of avian influenza virus and monkeypox virus expanding to the general population. We are very concerned at the terrible public health response to monkeypox and the allowed expansion into the general low risk population of this pathogen.
Vanden Bossche, Yeadon, myself, etc. have warned that if you keep vaccinating with a non-sterilizing injection, you are placing population immune pressure on the infectiousness of the virus, which is the spike. This while there is tremendous infectious pressure from the virus down onto the population, trying to infect. What happened? Well, infectious variant after variant is emerging and will never stop emerging as long as these ineffective, non-sterilizing, non-neutralizing vaccines continue that induce immature sub-optimal immunity. The sub-optimal immune pressure onto the spike drives selection pressure to ‘select’ the most infectious variant from among circulating variants that becomes enriched in the environment and becomes the new dominant.
We also know that the vaccinal antibodies (Abs) that are non-neutralizing (due to the vaccine) can still bind to the virus, such that binding is still taking place, but in binding, the virus’s infectiousness is increased for the vaccinee. The vaccinated person via antibody dependent enhancement of infection (ADEI) is getting infected. We have seen this many months now and we begged them to stop the vaccine. They did not. This is due to the non-neutralizing Abs from the vaccine pressuring the spike and driving the variants. Now we know the vaccinated person is massively at risk of infection.
We also warned that the increased infectiousness we were seeing (upper respiratory tract/URT) yet no severity (in LRT/lung) was not a good thing. Meant that the same way the variants overcame the neutralizing Abs on infectiousness (initially neutralizing Abs blocked infectiousness then the virus became largely resistant to the Abs and non-neutralizing Abs dominated) and non-neutralizing Abs were induced, then the same way initially there is blocking of severe illness in the lower respiratory tract (LRT) and lungs, the non-neutralizing Abs that would be induced would be overcome and surmounted by the virus variants (due to the sub-optimal immune pressure) and variants would emerge that would then cause severe disease.
We believe we are seeing it now in omicron BA.5 and more to come.
Again, it is not the virus that is getting serious, it is the COVID injection/vaccine that with the induced non-neutralizing Abs, places pressure in the spike (receptor binding domain and N-terminal domain) and is now potentially driving both infectiousness and severity/virulence.
The COVID injection must be stopped and must not be given to our healthy children as will damage their potent developing innate immune system that would be prevented from being optimally trained in childhood.
All we needed then and now, is to strongly protect the vulnerable population use vit D, use early treatment and nasal oral washes such as povidone iodine (Betadine) or hydrogen peroxide (swish and spit, no swallow, clean out nostrils), use chemoprophylaxis (prevention antivirals etc.) and allow the rest of society to live normal lives.
There is talk by Pfizer and Moderna of a reworked injection that is bivalent (OMICRON and Wuhan). This is very devastating for these inept clueless public health and vaccine maker people who did this will once again:
1)not recognize the potent interplay of the virus-host immune system ecosystem as it strives to regain/attain balance
2)you will be vaccinating a second time into a pandemic
3)by the time such a new vaccine and spike is produced, there will be new variants and as such as is now, we will have mass vaccination into a pandemic using a vaccine that induces vaccinal antibodies that are a mismatch for the target spike antigen.
Hospitals are geared up unless the PPE COVID prep money was stolen by those in charge of it.
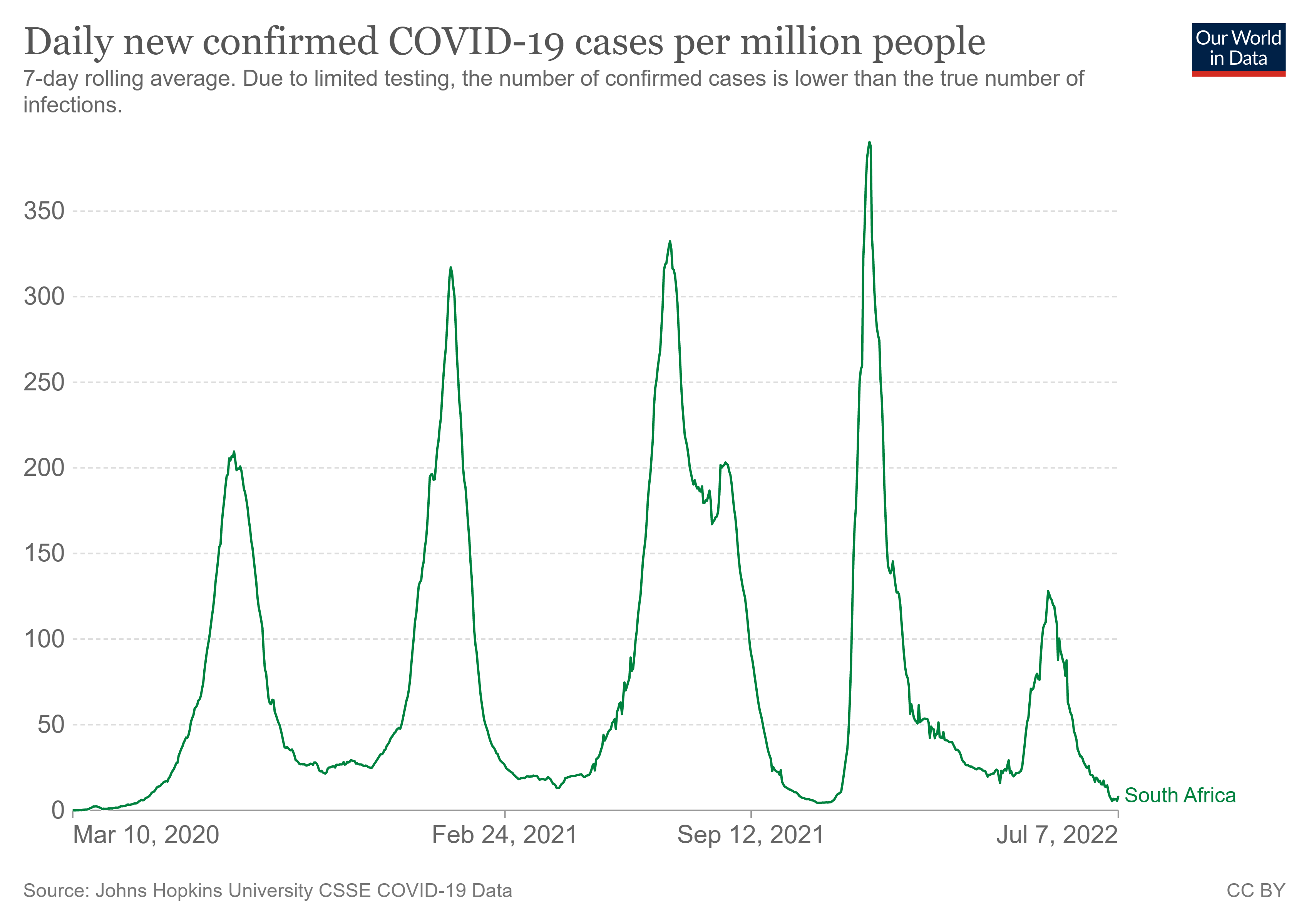
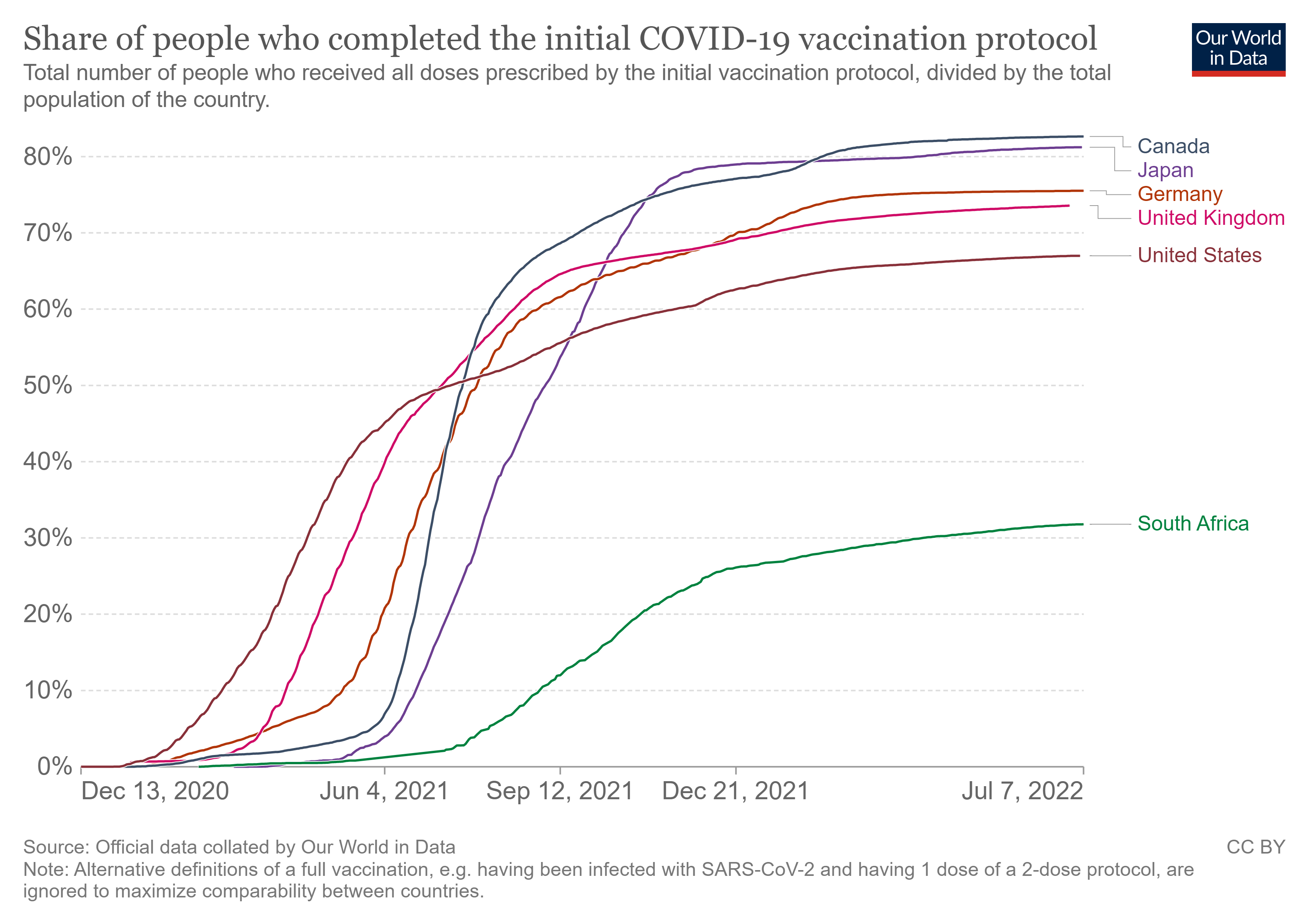
See graphs, we are not getting back to baseline on downward slope so massive virus hanging around and so we can never get to herd immunity and now the vaccine is driving massive infection in vaccinated persons globally, it has failed! South Africa fared well with Omicron BA 4 and 5 and why? Was it the low vaccination rate? I think so, certainly. There is a little blip but lets see. But what say you? Note, by delaying vaccine, the African nations also allowed training of the innate immune system in children and young persons who are now clearing out the virus. Children and young people are critical to any getting to herd immunity.

I have to keep asking. HOW? How do they not recognize ADE is developing? They HAVE to know!! So, what will the game plan be when this all starts happening? Who are they going to blame? They certainly won’t blame themselves!
Hey Paul and the other virology team.
Can you quit the parroting of your science language mubo jumbo and speak in simple English please..
I know you all want to impress each other with your completeness and accuracy,, but you are not reaching your audiences so they can effective turn your good info into persuading language to red pill the Vaxxed.
Use a scientific KISS methodology to communicate the same info into a usable form. GVB has the same problem.
Blue pulled vaxxers don't read your substack or follow you on Twitter.