Vicious rapid aggressive lethal TURBO cancer in 2 patients, 1 day & 2 weeks after 2nd Pfizer mRNA technology gene injection! Two cases of axillary lymphadenopathy diagnosed as diffuse large B-cell
lymphoma developed shortly after Pfizer COVID-19 vaccination; Mizutani et al.; 67 year old Japanese man, 80 year old Japanese woman; TURBO cancer, where is Malone, Kariko, Weissman, Sahin, Bourla?

https://onlinelibrary.wiley.com/doi/10.1111/jdv.18136
CASE 1:
Case 1 was a 67-year-old Japanese man who visited Tokyo-kita Medical Center complaining of a 6.0-cm subcutaneous mass in the left axilla 2 weeks after the second Pfizer BNT162b2 vaccination. Tenderness and a palpable lymph node (LN) in the left axilla were noted 1 day after the first BNT162b2 vaccination. Computed tomography revealed an enlarged LN in the left axilla (Fig. 1a), and it was suspected as a reactive lymphadenopathy. However, the nodule became bigger and was accompanied with redness of the surrounding skin. Hence, biopsy specimens were taken from the swollen LN and erythematous skin (Fig. 1b). Histopathological examination revealed a diffuse infiltration of large, atypical lymphocytes with centroblast and immunoblast in the LN (Fig. 1c) and the skin. The large, atypical lymphocytes were stained strongly with CD20, BCL2 and MUM-1/IRF4 (Fig. 1d–f) and were negative for CD3. The Ki-67 positivity was over 80%. He was diagnosed with DLBCL, and R-CHOP (rituximab plus cyclophosphamide, doxorubicin, vincristine and prednisone) regimen was initiated, resulting in the shrinkage of the LN.
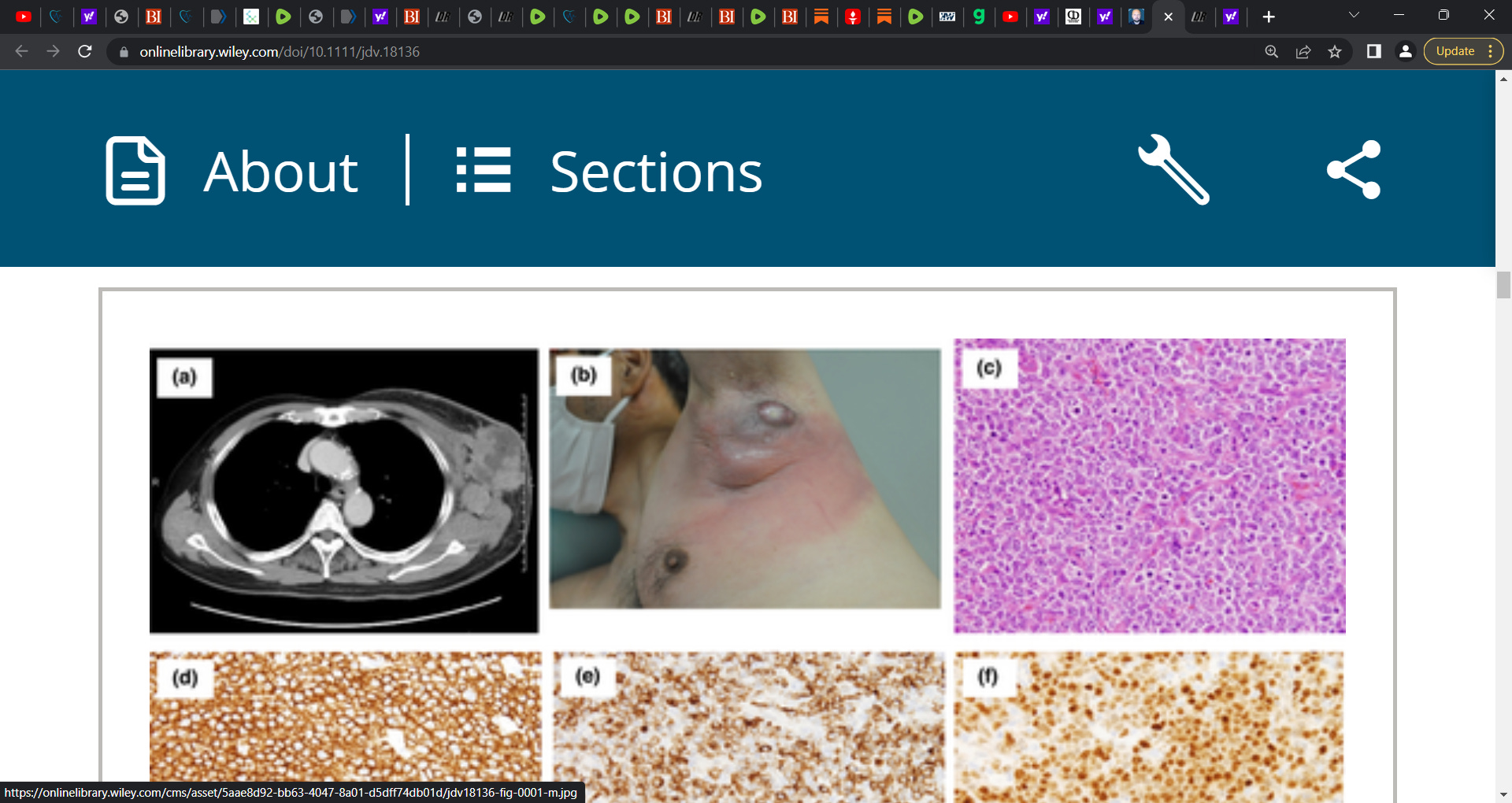
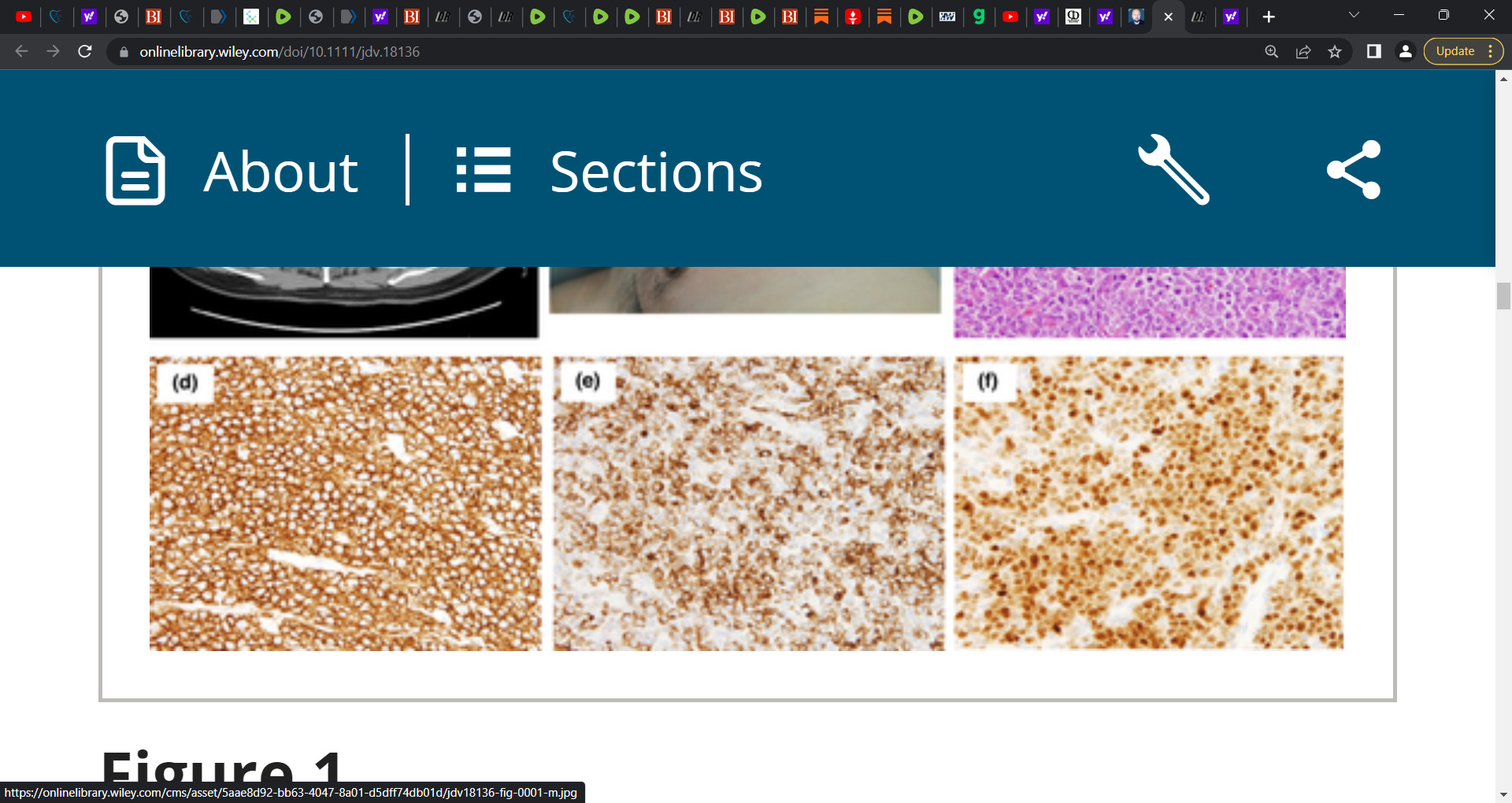
Clinical and histopathological characteristics of case 1. (a) CT image revealed enlarged mass in the left axilla. (b) A clinical image of the case 1 at the biopsy was presented. (c) An image of Haematoxylin and Eosin staining was shown (×200). (d–f) Images of immunohistochemical staining for CD20 (d × 100), BCL‐2 (e × 100) and MUM1/IRF4 (f × 100) were shown. [Colour figure can be viewed at wileyonlinelibrary.com]
IF THIS IMAGE HAS BEEN PROVIDED BY OR IS OWNED BY A THIRD PARTY, AS INDICATED IN THE CAPTION LINE, THEN FURTHER PERMISSION MAY BE NEEDED BEFORE ANY FURTHER USE. PLEASE CONTACT WILEY'S PERMISSIONS DEPARTMENT ON PERMISSIONS@WILEY.COM OR USE THE RIGHTSLINK SERVICE BY CLICKING ON THE 'REQUEST PERMISSIONS' LINK ACCOMPANYING THIS ARTICLE. WILEY OR AUTHOR OWNED IMAGES MAY BE USED FOR NON-COMMERCIAL PURPOSES, SUBJECT TO PROPER CITATION OF THE ARTICLE, AUTHOR, AND PUBLISHER.
CASE 2:
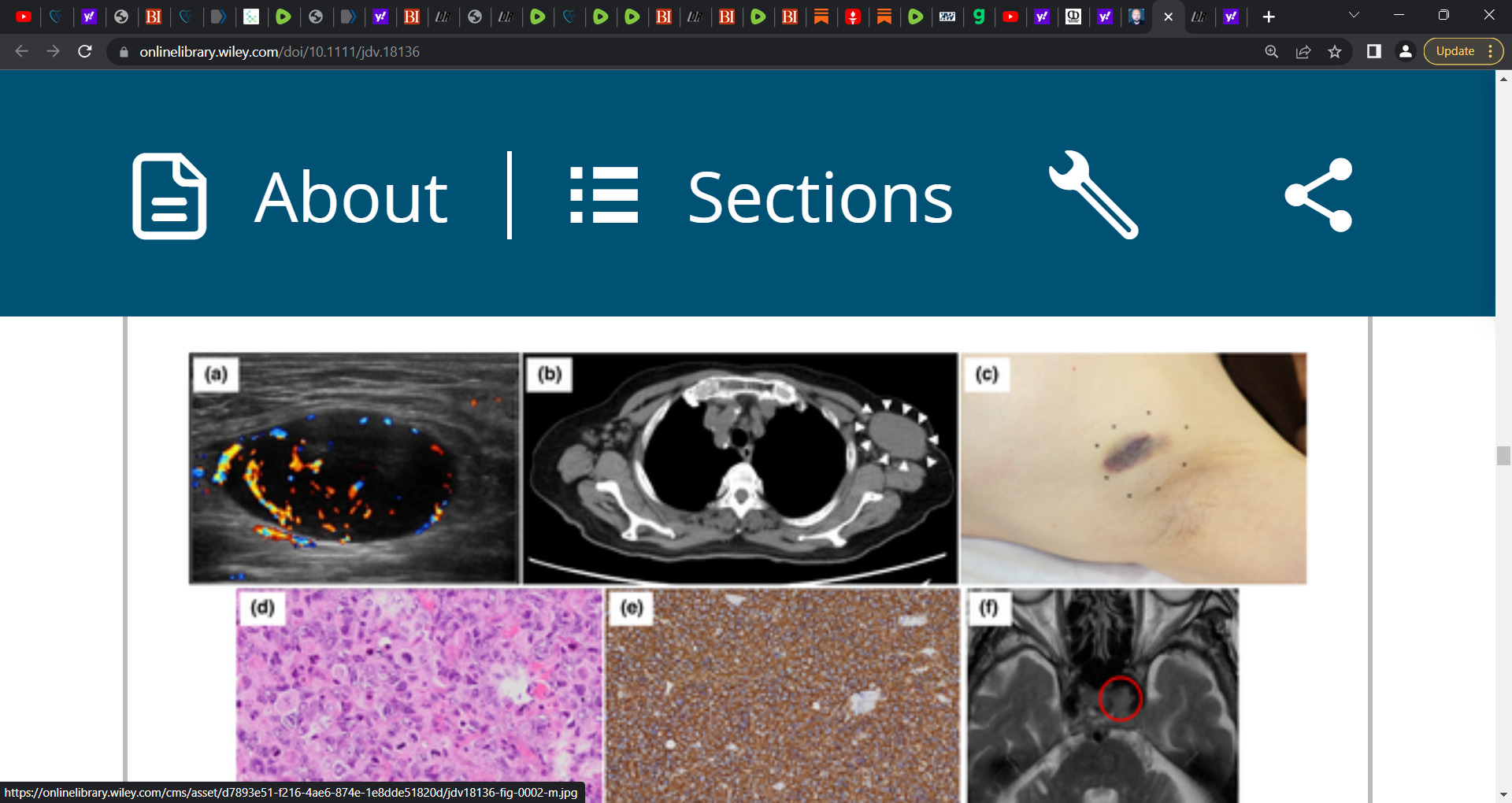
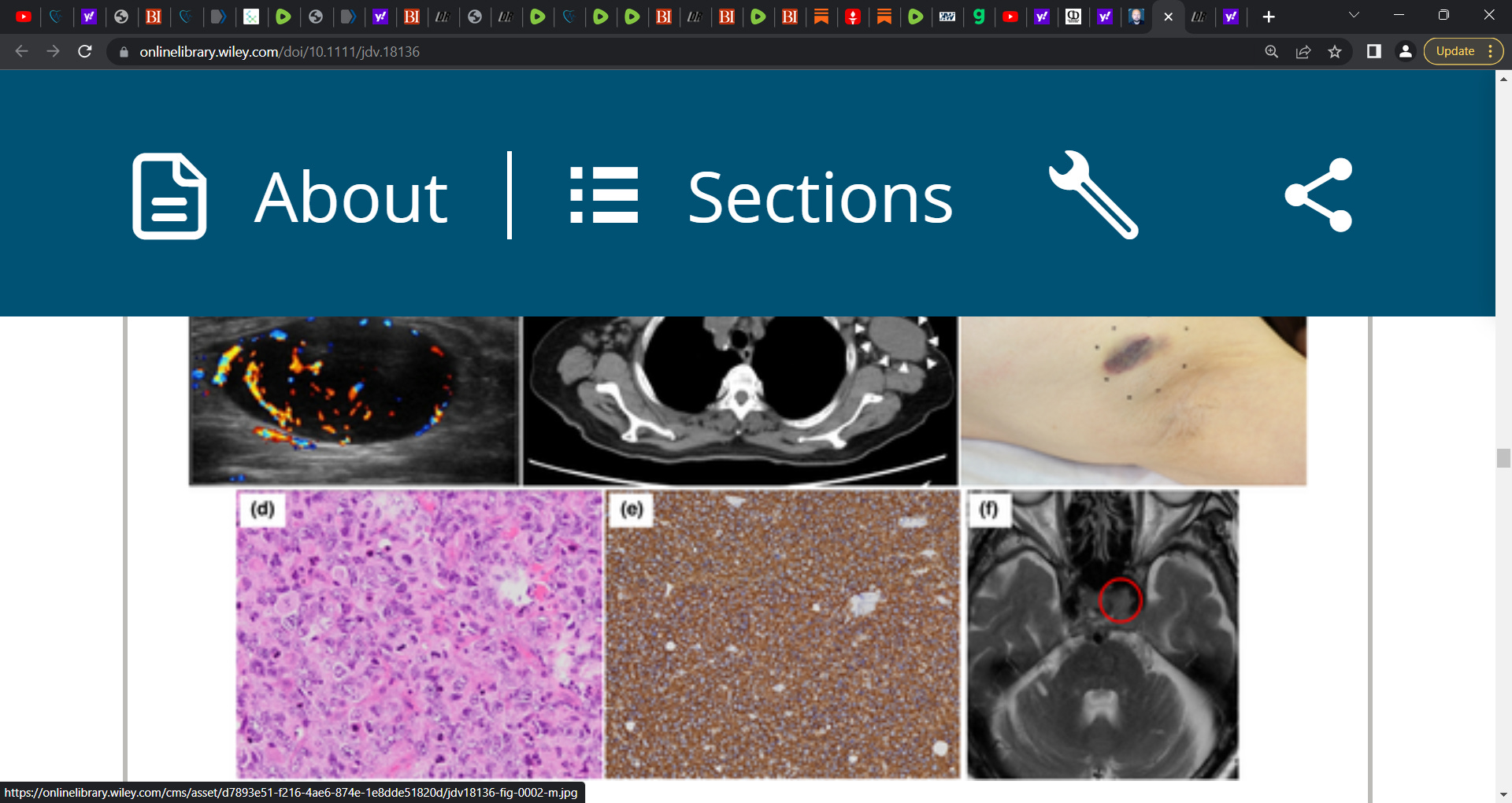
Case 2 was an 80-year-old Japanese woman who visited the University of Yamanashi Hospital due to an enlarging nodule in her left axilla 1 day after the second BNT162b2 vaccination. The nodule appeared 2 days after the first vaccination. Ultrasonography detected a 4.1-cm round mass with blood flow (Fig. 2a), which was suggestive of lymphadenopathy. Two months after the first consultation, the nodule gradually enlarged, and computed tomography revealed a 6.0-cm mass in the left axilla (Fig. 2b) and another 2.8-cm mass in the left mesentery. A biopsy of the nodule in the left axilla (Fig. 2c) demonstrated a sheet-like diffuse infiltration of atypical lymphocytes (Fig. 2d). The atypical cells were positive for CD20 (Fig. 2e), BCL6 and BCL2 and negative for CD3 and MUM-1/IRF4. The Ki-67 positivity was over 90%. A diagnosis of germinal centre B-cell DLBCL was made. The patient complained of diplopia and left eyelid ptosis 8 days after the biopsy. Magnetic resonance imaging detected a small tumour, a suspicious DLBCL lesion, in the left cavernous sinus (Fig. 2f). The dose-attenuated CHOP regimen with standard dose of rituximab was initiated. Besides, radiotherapy (40 Gy) targeting the brain nodule was performed. Through combined modality therapy, the nodules in the left axilla and left cavernous sinus disappeared.
This is the first case report of DLBCL developed shortly after Pfizer BNT162b2 vaccination, although the recurrence of remitted T-cell lymphoma cases has been reported.1, 2 Reactive lymphadenopathy after COVID-19 vaccination has been repeatedly reported; hence, both cases were initially suspected as temporal LN swelling. The influence of vaccination on the development of DLBCL is uncertain. BNT162b2 vaccines have been reported to induce a cytokine signature featuring IL-15, IFN-γ, CXCL10 and IL-6.3 On the contrary, the elevation of these cytokines was observed in the sera of patients with pretreated DLBCL,4 suggesting some roles of these cytokines in the growth or survival of DLBCL. Thus, it might be conceivable that pre-existing or subclinical DLBCL may rapidly grow in a specific condition induced by BNT162b2 vaccination. Nevertheless, the precise mechanism regulating the induction of DLBCL by this vaccination must await further investigations, including interaction between lymphoma cells and tumour microenvironment, genetic instability and so on.5, 6’
great articles and lots of great information to share. I wish we could do this on merck pharma t owith the drug called : KEYTRUDA is killing to many people and now they are experimenting with children using it. It was pulled off market in May 2021 and given to hubby 2 times and he died from it enlarging his heart double in size.
So horrible to realise that no matter how bad this gets, They will never acknowledge the likely cause. The chasm between reality and pretense/feigned ignorance widens ever further. The dissonance at every level of society is already essentially unbearable, in terms of allowing for anything which might be called sanity on anyone's part. Praise god and the warrior heroes like our author and his tribe. Their work, example, and inspiration are the rays of the sun in this dark dysfunction.