

Worrying Barmada et al. study showed troubling serial MRI results in adolescents following primary mRNA technology based COVID gene injection series: "Cytokinopathy with aberrant cytotoxic lymphocytes
and profibrotic myeloid response in SARS-CoV-2 mRNA vaccine-associated myocarditis"; persisting cardiac tissue inflammation because 24/7 cellular translation of Wuhan spike proten (Pfizer & Moderna)

https://pubmed.ncbi.nlm.nih.gov/37146127/
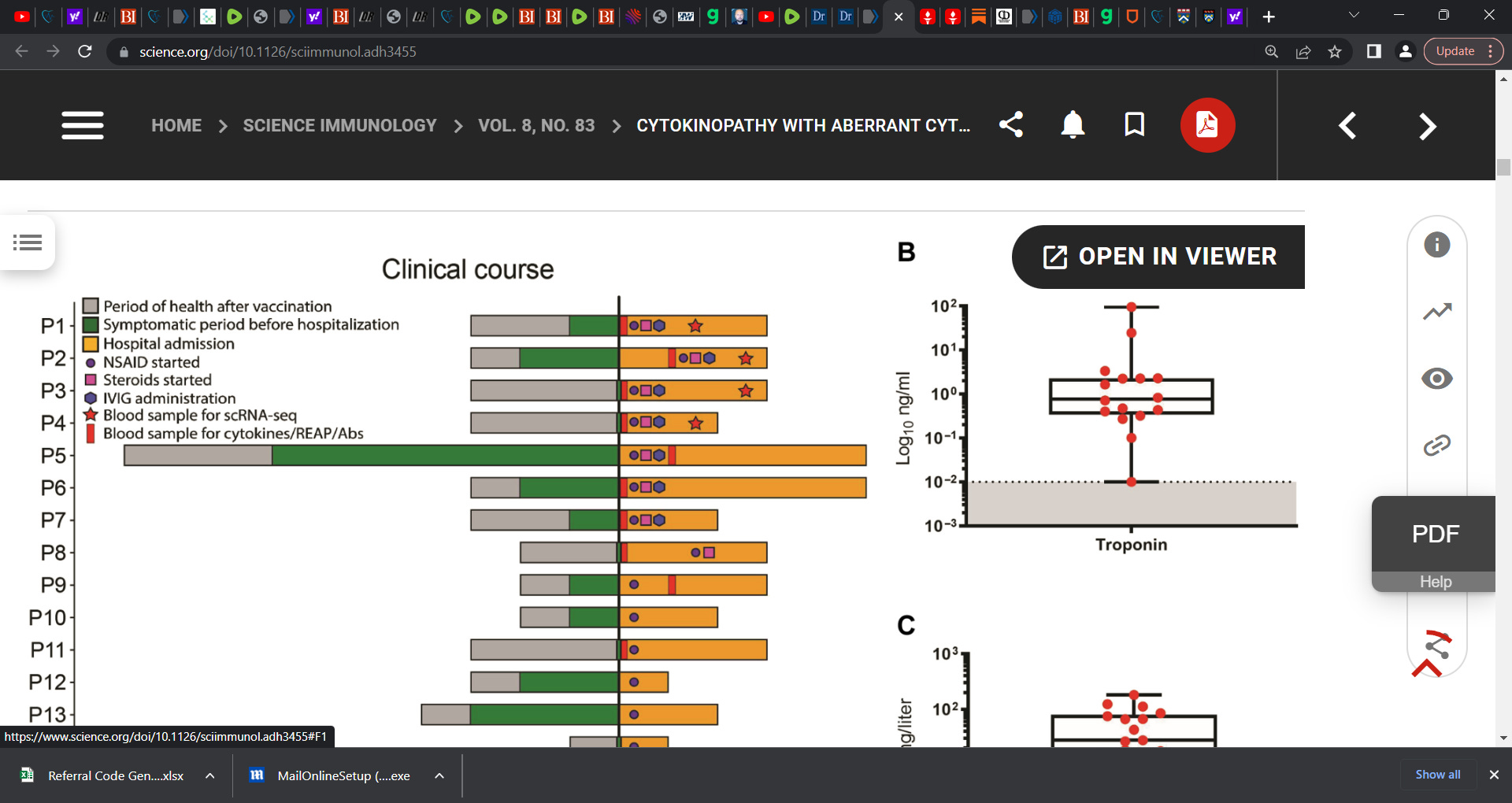
‘clinical cohort consists of 23 patients with vaccine-associated myocarditis and/or pericarditis. The cohort was predominately male (87%) with an average age of 16.9 ± 2.2 years (ranging from 13 to 21 years), in congruence with prior epidemiological reports (24). Patients had largely noncontributory past medical histories and were generally healthy before vaccination. Most patients had symptom onset 1 to 4 days after the second dose of the BNT162b2 mRNA vaccine (Fig. 1A and tables S1 and S2).’

‘Rare immune-mediated cardiac tissue inflammation can occur after vaccination, including after SARS-CoV-2 (COVID) mRNA vaccines…
the underlying immune cellular and molecular mechanisms driving this pathology remain poorly understood’…
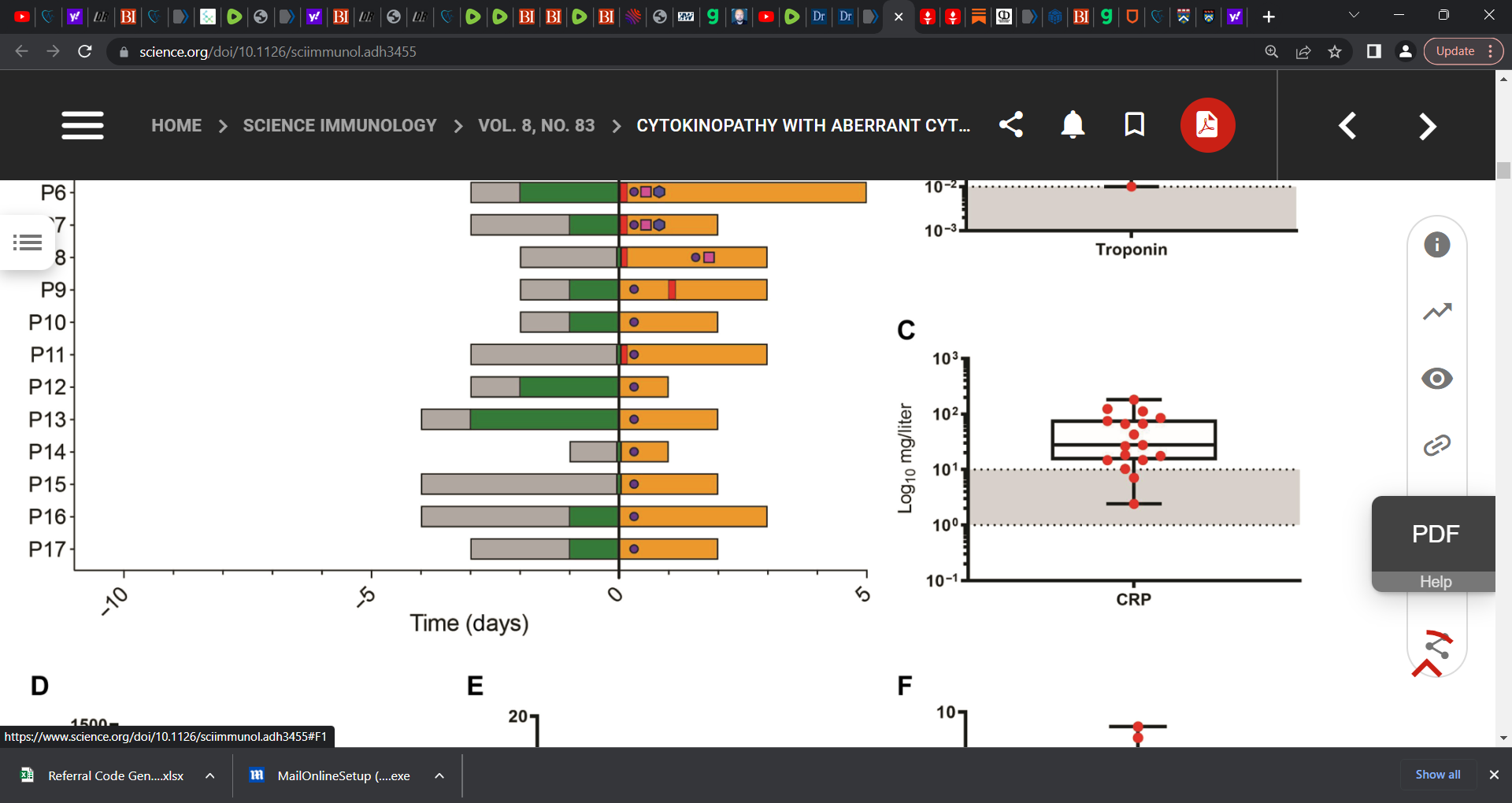
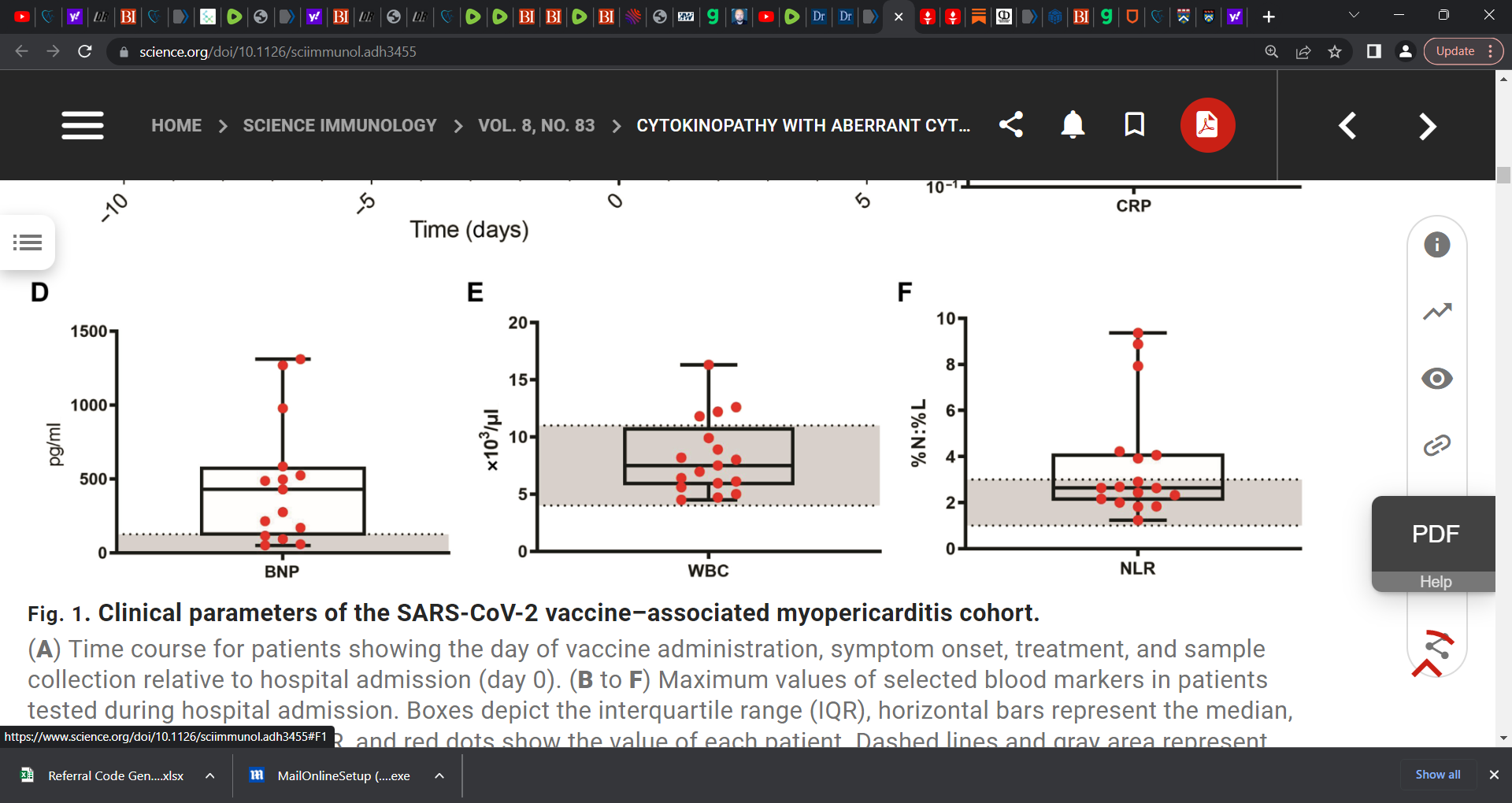
Researchers ‘investigated a cohort of patients who developed myocarditis and/or pericarditis with elevated troponin, B-type natriuretic peptide, and C-reactive protein levels as well as cardiac imaging abnormalities shortly after SARS-CoV-2 mRNA vaccination.’
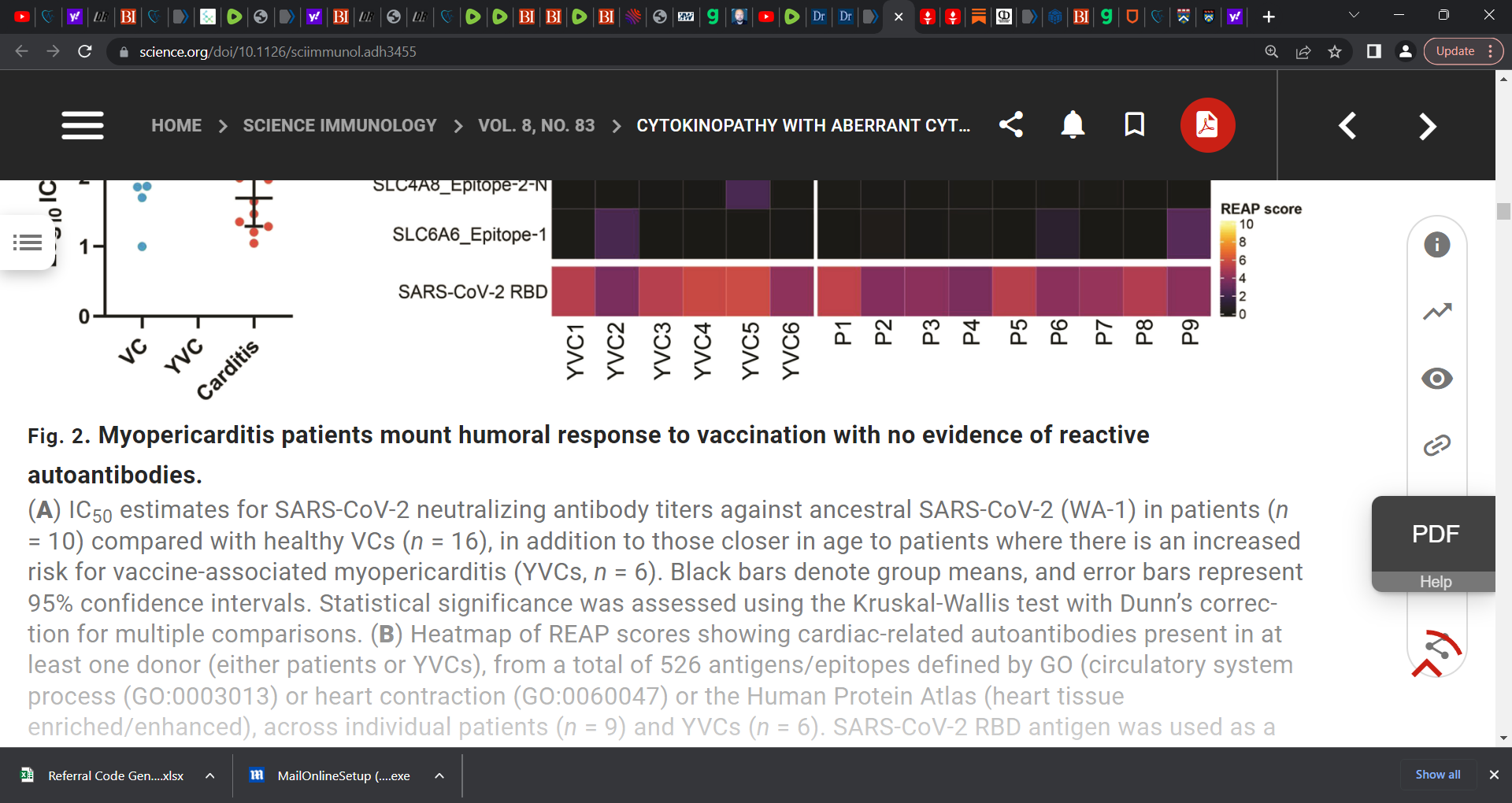
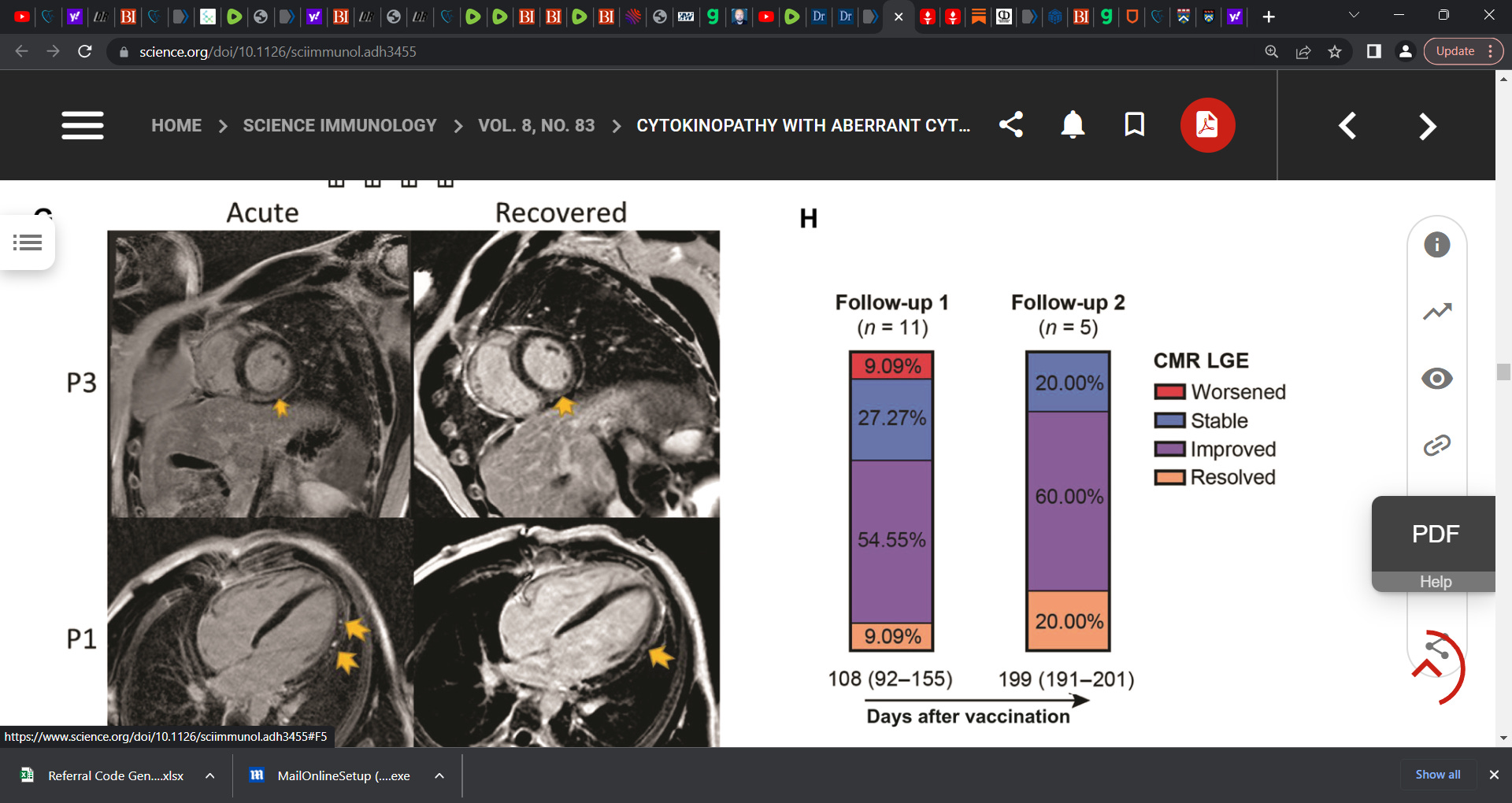
Contrary to early hypotheses, patients did not demonstrate features of hypersensitivity myocarditis, nor did they have exaggerated SARS-CoV-2-specific or neutralizing antibody responses consistent with a hyperimmune humoral mechanism. We additionally found no evidence of cardiac-targeted autoantibodies. Instead, unbiased systematic immune serum profiling revealed elevations in circulating interleukins (IL-1β, IL-1RA, and IL-15), chemokines (CCL4, CXCL1, and CXCL10), and matrix metalloproteases (MMP1, MMP8, MMP9, and TIMP1). Subsequent deep immune profiling using single-cell RNA and repertoire sequencing of peripheral blood mononuclear cells during acute disease revealed expansion of activated CXCR3+ cytotoxic T cells and NK cells, both phenotypically resembling cytokine-driven killer cells. In addition, patients displayed signatures of inflammatory and profibrotic CCR2+ CD163+ monocytes, coupled with elevated serum-soluble CD163, that may be linked to the late gadolinium enhancement on cardiac MRI, which can persist for months after vaccination. Together, our results demonstrate up-regulation in inflammatory cytokines and corresponding lymphocytes with tissue-damaging capabilities, suggesting a cytokine-dependent pathology, which may further be accompanied by myeloid cell-associated cardiac fibrosis. These findings likely rule out some previously proposed mechanisms of mRNA vaccine--associated myopericarditis and point to new ones with relevance to vaccine development and clinical care.’
McCullough further asked (posted by Dr Frank Yap, M.D. - May 13, 2023):
Is there ongoing heart damage and inflammation at six months?
Does the LGE in 80 percent represent a permanent “scar” putting these children at risk for future cardiac arrest? These data strongly call for large-scale research into this emerging problem given the large number of potential young persons at risk.
How can these findings be ignored? The temporal link to the covid shots is undeniable.
Last year Pfizer anounced they would "reduce the population by 50% by next year in 2023". I was 1 of many who saw and heard this last year. This took place in Davos, Switzerland at the WEF summit.
How do you think they will do this?