A miscarriage of statistics: The thalidomide sequel & how CDC etc. lied about COVID miscarriage rates that are far worse! NORMAL miscarriage rate is 5-6% but studies show it as 20% so that doubling
of rate is not captured and noted as devastating etc.; This is how the COVID vaccine managed to be sold as "safe in pregnancy" when it was far from it. CDC, NIH, FDA lied & deceived the public

This was an incredible piece of scholarship and the writer states this:
‘I hope this article has proven beyond a reasonable doubt, referenced throughout, that there is absolute certainty that the miscarriage rate has increased in those who have taken the COVID vaccines in early pregnancy.
What needs to happen now is the full CDC data set needs to be released to the public for independent analysis.’
Begin here:
‘This story is not going away, however much the pharma companies and their vaccination-in-pregnancy foot soldiers want it to. The recent revelations of the #Placentagate scandal has brought it to a head, and we are going to keep gnawing away.
I share this critical photo first and call on Dr. Naomi Wolf to follow up with this stunning piece of scholarship:

Because I know that everybody’s attention span is short I am going to put a summary here for this article.
The normal miscarriage rate of a healthy population is somewhere around 5-6%. For years, studies have been misrepresenting rates of 15-20% so that when new drugs are tested in pregnancy, a doubling of the miscarriage rate will fly under the radar.
This is how the COVID vaccine managed to be sold as "safe in pregnancy" when it was far from it. This article shows you how the data was misrepresented by the CDC and others to cover up the scandal.In a change of tack I’m also going to try and break up the article into sections with lay summaries at each point. Let me know what you think in the comments.
First, a recap
In the last article I showed you that the pharma companies had been abusing miscarriage statistics for decades. Essentially they ensured that miscarriage rates were recorded as higher than they should have been, using various methods but including “survival analysis” which can overestimate risk. Why would they do that? Well, in order to confuse you, so that when a drug hit the market with a higher than expected miscarriage rate they can say “oh it’s normal”.
Please read it if you haven’t already:
In that article I provided a preliminary model that was able to compare the published Naert 2021 (pre-COVID vaccine era) analysis of miscarriage rates to the CDC’s V-safe (COVID vaccinated cohort) miscarriage rates as discussed in depth here.
Because some people’s minds work pictorially lets put a face to the studies:

You can therefore think of the Naert cohort as the control group and the Zauche dataset as the vaccinated group - of course that’s all we have because the CDC chose not to invite a control group to their study (I wonder why).
The Naert dataset is the biggest (to date) publication of miscarriage data where the authors were able to follow a whole cohort of pregnancies. Although it is a retrospective study (looking back after collecting data, traditionally susceptible to bias) it attempts to recreate (model) a prospective study on the basis that all patients were included and it draws conclusions about the miscarriage rates as if you presented at 6 weeks of pregnancy. That’s the closest we have come to a prospective study in pregnancy - in order to do a real prospective study you would need to recruit thousands of women and follow them up for years (which is why it’s never done!).
One criticism levelled against the Naert paper (once the world of Pharma-affiliated doctors realised that it could expose them) is that it ignores pregnancy losses prior to 6 weeks. This is true, and that is because it is impossible to measure these. These include women who go for medical terminations and those that have a positive pregnancy test one day and then it’s negative the next. These wouldn’t normally be registered as pregnancies in any clinical scenario so they are mostly excluded from any studies. However, Zauche (who collected the V-safe pregnancy data for the COVID vaccine registry) also removed these patients from her analysis.

The Naert (independent, control) and Zauche (CDC, vaccinated) cohorts should be able to be directly compared with some adjustments as I go through below.
For this analysis I am going to assume that the distribution of miscarriages in the Zauche data is simply due to the way they have been allocated, but we cannot exclude the possibility that the large rise in miscarriages in week 8 & 9 is due to the impact of the COVID vaccine

So let’s get to it. I’ll try and summarise each section as we go…
1. Zauche overestimated the miscarriage rate in her first paper
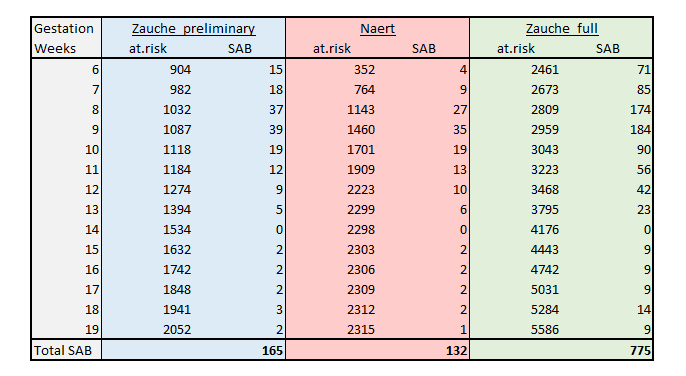
In Lauren Zauche's first paper she estimated the miscarriage rate at 14.1%, for 165 miscarriages out of 2217 pregnancies (7.4%). How is this possible?I’ll try and go over this again because it’s difficult to understand why such a simple calculation can be so complicated to present. Essentially, they are purposefully double-counting. Here is the table from the early Zauche paper

If you don’t want to do the calculation yourself it’s 165 SAB’s (miscarriages) and the total number of pregnancies in the number at risk at the end of the study period (2052) plus the 165 that miscarried, i.e. 2217. The “number at risk” in survival analysis, which is the way this was then calculated, is the number of people remaining at any one time, because some people have been lost to follow-up. In the analysis of cancer data that is usually because they have died or recurred. In this case it’s because they have miscarried.
In order to get to a 14.1% overall risk of miscarriage what the authors effectively did was add the percentages for each week
, which basically doubles the raw risk - the number most people would refer to.
To avoid switching between use of “raw risk” and “survival analysis risk estimate” all we have to do to compare the rates directly is treat the cohorts in the same way. Simple eh?
Annoyingly the two cohorts are distributed differently by week but we can assume the following:
Because the rate of miscarriages jumps at week 8-9 it is assumed
that the time point at which the miscarriage happens in the Zauche (vaccinated) cohort is the week of gestation in the table.
Conversely, in the Naert (control) analysis it is assumed that the time point at which the miscarriage happens is irrelevant and the miscarriage is attributed to the week that the woman presented for study.
It actually doesn’t matter that the distribution of miscarriages by week (e.g. of 100 miscarriages there were for weeks 6-12: 20,20,15,15,10,10,10 per week or there were 10,10, 30,20,10,10,10 per week) because we are going to match them.
In the analysis below what I have done is taken the whole cohort of pregnancies, and distributed the miscarriages in exactly the same way in accordance with Lauren Zauche’s distribution. That is, the number of miscarriages remain the same as in the publications but the way they are distributed through the weeks is now made to match up between the cohorts, so there is no confounding due to reporting technique. These are the new “modelled” data sets (in blue and pink):
The eagle-eyed of you will hopefully have noted the green column, which we will get to soon. For now we can plot (as we did before, but with much better matching) the two cohorts on a survival-style curve (remember that I don’t personally approve of this technique here, but we need to match the cohorts)

You should be able to see from this survival analysis-style comparison that the Zauche cohort does a lot worse. In fact we can quantify this with a Hazard Ratio which in this case is 1.5 - roughly that there was a 1.5x increase in miscarriages in the Zauche cohort than the historical Naert cohort. The p-value on this calculation was 0.001 meaning that it was a one-in-a-thousand chance that this was a random event.
Section summary:
In a properly matched comparative analysis between a contemporary published historical cohort of miscarriages and the early CDC (post-vaccine) data set there is a clear increase in the risk of miscarriage in the vaccinated group2. Zauche never published the follow-up data, but presented it to the CDC
Now comes the interesting bit. As this model is now comparable between cohorts we can again look at Zauche’s later data where she presented to the CDC the miscarriage data some months later. In that presentation there were an estimated 775 miscarriages out of 6,352 first trimester pregnancies
. To our knowledge this data has not been formally published. There is no logical explanation as to why this data was not published given that the original Shimabukuro paper came out within weeks of the first pregnant patients being injected.
Plugging these numbers into our model we get a “raw” miscarriage rate of 12.2% (775/6352) which you were told was “within historical limits”….
But hang on, that is a “raw” rate not a “survival analysis estimate” rate. And it’s jumped. A lot.
Just to recap. The "raw" miscarriage rate is the % of total pregnancies that end in miscarriage. This should be around 5-6%. It's what most people would think of as the miscarriage rate.
The "survival analysis estimate" rate is an overestimate of the miscarriage rate arrived at by (inappropriately) using cancer survival analysis methods to miscarriage data.
The two methods are so different that it is not possible to compare them, but if you wanted to hide a "raw" rate that was 10-14% instead of 5-6% you would say it matched "historical rates" whilst forgetting to declare that the historical rates were calculated with the higher rate method. So now what we can do is show you
what those figures look like if you make the necessary adjustments to match the cohorts up and do a similar survival analysis. This makes the cohorts directly comparable.
The pink curve is the original Naert (pre-vaccine) cohort and the green curve is the final Zauche CDC (post-vaccine) cohort presented to ACIP in October.

Now you see the green curve falling off much more dramatically than either the Naert historical data or the earlier Zauche preliminary data.
To see how significant the difference is we can compare them all on a forest plot which shows you the comparative “hazard ratios”, i.e the relative risks.

Now this time we see that the “Full” V-safe (COVID vaccine cohort) data, which was delayed and presented by Zauche in October has a hazard ratio (risk of death i.e. miscarriage) of more than double the “historical” data of Naert.
Just to push the point home we can pretty much now dispense with the sanitised “letter to the NEJM” version of the Zauche COVID vaccinated cohort data and just show you a comparison of the historical data against the interpolated CDC COVID vaccine data on a survival-style analysis.

As John Campbell said earlier in the week - this should be considered a slam dunk. The fuzzy colours around the lines are the confidence intervals (the range in which you could anticipate errors) and they are so far apart from each other you could drive a bus between them.
Why is the rise in miscarriage rate in the V-safe data so dramatic and obvious when presented like this? I’ll say it again
Lauren Zauche confused and conflated the public - by intention or incompetence - by misrepresenting the miscarriage data at different time points, providing different measures of the miscarriage rate and claiming them to be the same.
The real increase in miscarriage rate shown by the CDC data is dramatic - more than double - and should have immediately prompted cessation of administration of the COVID vaccines to pregnant women. 3. What does the real world data tell us about normal miscarriage rates?
On our side of the isle we don’t really like to rely on a single point of data. So have we got some corroboration of the 5-6% claim that I have been so vociferously banging on about for over a year? Well of course we have.
The UK NHS publishes its “Hospital Episode Statistics” (HES) data annually and so if there was a big increase in miscarriage we would expect to see it. Well, yes and no. Remember that most women of reproductive intent pushed back against the jabs so there were only a small proportion (driven mostly by healthcare workers forced to have it) that took it during pregnancy. For most of those who capitulated, other than the very indoctrinated, they would have delayed it as far as possible into later pregnancy. As most miscarriages require the insult to happen in the 4-8 week window, we are now talking about any effect being easy to hide.
In other words, if the vaccine doubled the miscarriage rate but was only taken in the relevant “miscarriage window” by 5% of women, for every 10,000 pregnancies there would only be an additional 25 miscarriages (that is, a 0.25% absolute increase in miscarriage rate)
It’s another way to hide the harm that pharmaceutical interventions cause in pregnancy, which is why we don’t use them - and especially in the first trimester.
Remember that the thalidomide scandal - the worst, most egregious act of pharmacy fraud ever perpetrated on women - only resulted in 2% of women who took the drug having an affected baby. It took nearly 5 years to identify the problem and over 50 years for recognition to be given to those victims.
The estimated increase in miscarriage rate attributed to thalidomide was approximately double, similar to what we are seeing with the COVID mRNA vaccines
Looking at this another way we can mock-up various scenarios for miscarriage rate before or after taking a drug (in the “miscarriage window”)

Note that the “% increase in miscarriages” here is the absolute rate increase… that is the extra miscarriages as a percentage of the total pregnancies. You might be familiar with this concept after the hullabaloo over ARR vs RRR in the vaccine “effectiveness” we discussed in “Don’t be ARRsey”.
As you can see even a high proportion of women taking a drug that doubles the miscarriage rate will be barely noticeable in the overall miscarriage statistics. Conversely, any increase in miscarriage numbers is hugely significant. In fact, according to the chart you would need 40% of the women to take the drug with a tripling of miscarriage rate to produce even a 4% increase in the overall miscarriage rate!
So what does the UK HES data say? Well this was gone into at length by the mouse in this thread (archived). Here’s the clincher:


What happened with the UK HES data was that in 2020, during “COVID” (when the hospitals were shut so that the nurses could make tiktok videos and the elderly in care homes were euthanised en masse) doctors were instructed to handle miscarriages and abortions out of hospital. There was therefore a drop in the number of “spontaneous abortions” registered in hospital and this makes comparisons difficult. However there was certainly an increase from 2021 to 2022 of about 5%. This is a significant increase given the above.
And, what was the overall rate of miscarriages in the UK HES data? Was it 15% like Caz Sampson claimed? Was it 20% like Viki Male claims?
Absolutely not.
According to the latest UK HES statistics 103,277 miscarriages in 1,889,974 pregnancies for 2018-2021, which is 5.5%
This figure has remained relatively constant at under 6% since 2013
The HES data do not include terminations (“induced abortions”), which have remained above 200,000 annually since 2018.
Adding abortions into the denominator reduces the background miscarriage rate in the UK to 4.1%.
Yep, 4.1%. Now you see how the Viki Males, Lauren Zauches, Tom Shimabukuros, Kevin Aults and Caz Sampsons of the medical world have lied to keep their beloved “safe in pregnancy” con going.
But let me reiterate (again and again if necessary)…
The background miscarriage rate of a normal population in 2023 is 5-6%. Following the rollout of the COVID vaccines all evidence that has been submitted shows that the miscarriage rate in vaccinated women has jumped to 15%.
The claim that this is within historical limits is a lie.
Furthermore, the fact that only a small proportion of women would have chosen to take the COVID vaccine in early pregnancy shows that the real danger is massively underestimated, and could well be much more than a doubling of the risk of miscarriage.
4. The thalidomide miscarriages
I realise that I keep returning to the thalidomide scandal but one important lesson that we should have learnt from it was that any increase in miscarriage rate is a massive red flag for severe congenital anomalies.
Although the figures are not easily accessible it is estimated that two million women took thalidomide worldwide and the UK had approximatedly one-tenth of the world’s affected babies, with 2000 victims. For that population it was estimated that there were also an additional 6,000 miscarriages, which is 3 percent.

This figure is vitally important. The most teratogenic drug in history only caused a 3% increased risk of miscarriage, yet here we are with the “safe and effective” (aka “never tested”) mRNA-LNP therapies showing a red flag 6% rise in raw miscarriage rates - more than twice what we saw with thalidomide.
Just to push the point home one other massive red flag for this kind of teratogenicity was this chart which opened up a huge can of worms now known as #Placentagate, explained in more layman’s terms in this great little substack.

The figure that is referenced shows a small drop in the number of viable fetuses in all the groups treated with mRNA or mRNA-in-lipid-nanoparticles. Nearly every type of lipid nanoparticle they used in this study went to the placenta. But what is not shown is the inverse of the numbers, that is “how many pre-implantation fetal losses occurred in each group?”. Of course by necessity there must have been more in the treated groups in order to have less viable fetuses. The “pre-implantation loss” in an animal mode is a surrogate for miscarriage in a human model.
But we already knew that the Pfizer vaccine animal tests showed a doubling of pre-implantation losses. I have discussed it ad nauseum but more overtly in “A miscarriage of medicine” here:

Note that caveat too - “within historical control range”. You can’t do that in a contemporaneous study, sorry. The reference to a historical control was a con in just the same way that “a 15% miscarriage rate in women after the vaccine is within historical limits” lie is.
It doesn’t just end there. The people approving this stuff should have known that any signal like this had to be thoroughly investigated. They couldn’t care less. All that mattered - for whatever reason - was getting those mRNA jabs into pregnant women.
And guess what happens when you treat small furry animals with thalidomide? Funnily enough they don’t lose limbs. What happens is exactly what happened in the Pfizer study - the number of preimplantation losses (“early resorptions” in the table below) goes up, with a small reduction in the overall number of live fetuses.
Here is a study of thalidomide in rabbits that shows exactly this:

Fortunately the penny seems to finally be dropping with some more mainstream COVID investigators as John Campbell shows his shock at the incompetence of the TGA in this interview with the most experienced immunologist in Australia, Professor Robert Clancy. He explains (at around 20:20) that the preimplantation losses are a red flag for miscarriage (and other congenital anomalies).
Let’s recap this section:
The TGA had information in preclinical reports that there was an increase in preimplantation losses in animal studies. The increase seen was of the same order of magnitude seen in thalidomide studies in animals.
Although thalidomide is famous for the limb abnormalities of the babies that survived, there was also a small increase in miscarriages which should have been a red flag for teratogenicity (fetal toxicity).
The increase in miscarriages seen with the mRNA COVID vaccines is bigger than that seen with thalidomide.
The TGA, MHRA, FDA and EMA and the OBGYN colleges had all this information and not only ignored it but ensures that those raising the alarm were suppressed using coordinated attacks on social media.
5. The CDC are involved in a massive cover up
So, the question that you should all be asking is: if some anonymous account on substack has been writing about this for over a year, why has the CDC not paid any attention?
The answer is simple and the only logical assumption that can be drawn is this:
The CDC knew that this was going to be a problem but were told to shut up and bury the story. They collaborated and colluded to force investigational gene therapy vaccines on pregnant women by lying to declare them safe and therefore justifying the imposition of vaccine mandates on pregnant women.
This really is Mengelian medicine.
Talking of which, here’s a fun fact (that may or may not be related). Two famous Nazis involved in horrendous war crimes never had to face the Nuremberg trials - Josef Mengele and Franz Rademacher.

Mengele - who conducted medical experiments on his captured population just as Minister Brad Hazzard did in South West Sydney in 2021 - escaped to South America and had a family and then grandchildren. The fate of Franz Rademacher - the Nazis’ lawyer - is less well known but he escaped to Syria.
The Rademacher name however prompted some consternation on twitter in the #placentagate scandal which erupted over the last few days. If you haven’t yet checked it out you should - here and here and with discussion of Thomas Rademacher here .
The “Placentagate” scandal relates to the fact that the very people involved in pushing the COVID vaccines on pregnant women knew that the nanoparticle vector would take it to the placenta, and had never ever been tested in human pregnancies.
How much more evidence to we need?
Now that we have investigated this as far as we can I’ll just list the evidence that we have that the COVID vaccine rollout has not only resulted in a glut of miscarriages but the CDC, Viki Male and Kevin Ault, as the main proponents of the “it’s safe, honest” dogma, have covered it up.
We have established beyond reasonable doubt that the background miscarriage rate should be less than 6%
Zauche, Shimabukuro and others have claimed that the post-vaccine miscarriage rate is around 14%
There are significant confounders in the miscarriage data and because the CDC refuse to release the V-safe data for independent analysis we have to interpolate the data on what we have
The CDC could have solved this problem by creating a control group (similar aged women who didn’t take the vaccine) for V-safe. Hundreds of thousands of women would have been happy to participate. They deliberately chose not to, to hide the increase in miscarriages.
Using directly comparable modelling that has never been performed before, we have shown in this article that the miscarriage rate as presented by Lauren Zauche, following the COVID vaccination, is at least double what it should be.
So what happens next?
I hope this article has proven beyond a reasonable doubt, referenced throughout, that there is absolute certainty that the miscarriage rate has increased in those who have taken the COVID vaccines in early pregnancy.
What needs to happen now is the full CDC data set needs to be released to the public for independent analysis.
There is no reason this cannot happen tomorrow. The data can easily be deidentified (SQL has built in functions for this and exporting this data would take less than an hour of work). It is clear that the people who have been running the V-safe registry have huge conflicts of interest and can no longer be trusted to deliver this data.
If you have got this far in the article you get to have your say on this. This one should be a slam dunk too, but let’s see.
POLL
Should the V-safe pregnancy registry data be immediately released for public academic re-analysis?
Yes
No
253 VOTES · 2 DAYS REMAINING
Irrespective of whether we ever get this data and can audit it, the thalidomide scandal should have taught us that the miscarriages may well be the tip of the iceberg. In fact Lauren Zauche knows this because it was part of her presentation.
This is the bigger disaster looming
:

Enough is enough. It was not OK for Tom Shimabukuro to refuse the release of the V-safe data or Lauren Zauche to misrepresent the miscarriage rates. This is not the end of the matter, but this series of articles should have provided you with enough information to file complaints against the institutions and the people acting with malfeasance or abject incompetence and those who told you it was safe. It wasn’t. Anybody that knows how the mRNA vaccines worked knew that it couldn’t possibly be assumed to be safe in pregnancy.
Our latest Welcome to Gilead montage is therefore designated to those prominently involved in this disgraceful propagandised assault on pregnant women. We’re running out of room though.
Welcome to Gilead.
Part 8.

We don’t believe that the authors literally added the percentages for each week to get to the final data but the effect of using survival analysis to estimate the risk is effectively that, as it calculates a cumulative risk of an event by adding the risks at each time point. Hence in some cases (as in miscarriage analysis) it overestimates the risk.
This has to be an assumption because of the lack of clarity in the methods. The distribution of the data suggests that this is what happens because instead of the most miscarriages being in the 6 week group, as we are told to expect, they are recorded in the 8-9 week group. Miscarriage risk always goes DOWN during the first few weeks of pregnancy so the only explanation is that Zauche’s data records the miscarriage during the week of the event. An alternative explanation is that the women were vaccinated in week 6 and a whole bunch of miscarriages happened in week 8-9, which is possible. Without this raw data it is not possible to decide this.
This excludes the preconception group (which were excluded anyway) and makes a 7% downward adjustment to exclude the small number of second trimester miscarriages as explained previously.
The R code for this analysis is available as a text file here:
https://files.catbox.moe/fmzgil.RIf you go back to the earlier article you will see why that’s not “normal”. And the increase is likely to be an underestimate for the same reason - it would likely only affect the minority who took the injection in very early pregnacy.
Recommend Arkmedic's blog to the readers of Alexander COVID News-Dr. Paul Elias Alexander's Newsletter
Striving for truth and transparency in science and medicine. Posts should be considered public interest disclosures in relevant jurisdictions. All comment sections are open so if you see a scientific or factual error please comment.
Lipid nanoparticle (LNP) activity below in the uterus of pregnant mice after distant injection, showing that they travel to every part of the body. PBS = control (no LNP). From https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9992266/
Strokes, Heart Attacks, Myocarditis, permanent Sterility,miscarriages, it's all coming to be understood, the culling of the World's population, those two words; "Safe & Effective" leading many to take the jab, with unknown consequences...
Our vaccinated niece miscarried in her fourth month. Are there separate stats for vaccinated women who became pregnant and THEN miscarried?