Dr. Joe Ladapo: those criticizing last study on mRNA gene vaccines showing 84% increased cardiac deaths in young men (18-39) DON'T grasp research methods; Self-controlled Case Series (SCCS) is strong
SCCS is strong (modified cohort) research methodology utilized to control between-person confounders (known & unknown), individuals act as their own control; if you DON'T understand Joe's work, STFU!

If you do not know what you are talking about or are scared to debate Ladapo one on one about the data and methods, then keep quiet. Stop embarrassing yourself.
Firstly, what we have seen that is thematic throughout the response to COVID across governments, within academic, within the medical profession, and within alphabet health agencies etc. is not simply miscommunication, but a vicious attack and smearing of any person (persons) who seek to share information surrounding risk and benefits of the COVID policies and vaccines. Especially polices that have all turned out to be 100% flat wrong.
All have failed (lockdowns, school closures, mask mandates, vaccine mandates etc.) yet those who design and implement the policies, using an uninformed media as their attack dogs, simply go on the attack and a slander of credible people ensues, a slander and demeaning of people who simply are trying to help save lives. This has been highly destructive and the usual suspects, true to form, were at it again pummeling Dr. Joe Ladapo when he published and raised some very concerning findings about cardiac risks post COVID mRNA vaccines in young males.
The point is, these IMO academic and technical malfeasants, with their apparent academic sloppiness and cognitive dissonance, attacked his research methods yet failed to grasp that when well conducted, SCCS is a very potent research methods design. It yields potent signals and a core tenet is its capacity for using the subject as its very own control.
We know that ideally you want a randomized controlled study (RCT) to define causality etc. yet proper conducted observational studies (prospective or even retrospective while the former is ideal) can be as good or even superior than small sample sized and sub-optimal RCTs with corrupted research methods e.g. sub-optimal randomization, allocation concealment subversion or breaching of the generated sequence, data loss (especially if differential across trial arms and over 10%), failure to blind adjudicators of outcome and data analysts etc., severe baseline imbalance etc.
Yet detractors took to the internet to lash Ladapo for the strong SCCS study that showed an elevated risk for young males post COVID mRNA gene injection, this risk for being cardiac deaths. Yet these are politicized fools and they know it. They know (or I hope they did) that the SCCS while not the top dog method, is also very strong for it can help eradicate all stable confounding (known and unknown/unmeasured) by using the person as their own control.
Not even and RCT does that. The SCCS (yields relative incidence) helps deals with the often huge problems of finding a proper control group matched on the relevant variables if an RCT cannot be conducted. This approach also does not require the massive sample numbers needed for RCTs etc. especially if the baseline risk is very negligible and thus one would need to massively power the study to tease out differences (thus power is often addressed nicely). No doubt it will be plagued by the biases other research studies are affected with yet we try to adjust and control and moderate them best we can. No study is perfect and even randomization at times can fail in RCTs.
With such massive COVID vaccine coverage in western nations (where his question was being extrapolated to), it would be very difficult today to find unvaccinated people to comprise control groups. Yet the key potency is that persons act as their own controls and thus you eliminate the individual differences ‘between’ people that often color and distort the resulting estimates of effect and bias them.
So I find this to be a good study and the results robust enough to raise very serious questions on cardiac risk due to these mRNA vaccines, and not just in young males, but across the board in age-groups.
You seek to always find unbiased estimates to make informed decisions. You wish to reduce the impact of confounders. SCCS has been used in hundreds of studies for medications and vaccines. It is self-controlled and thus effectiveness or safety of a medication etc. can be dealt with via this self-controlled design as it can be regarded as quite unbiased. Different people will have different behaviors and backgrounds and likes and dislikes, preferences etc. and thus this can confound the estimates of effect and the SCCS reduces these constraints. Outside of an RCT, it is hard to control for distorting confounding variables. SCCS can do this. This is the power of the SCCS design. If you did not understand what he did or the approach, go read it. You did not need a control group here for it is ‘self-controlled’ for the 50th time. Moreover, many studies published in high impact journals did same, same design, yet you did not hammer those researchers. Why Ladapo? What is it about him? hhhhhmmmmm
Again, it is a self-controlled design and you use people (as their own controls) with their own baseline risk and it helps tease out the effect of the intervention without the confounding (one may argue confounding is removed). So you did not need another control group (for the 100th time now), it is the key potency. It is people with their own baseline risk and any aspect (intervention) that increases or decreases risk is linked to the intervention exposure e.g. the drug or vaccine. You have removed the individual differences and preferences and behaviors that impact estimates of effects.
You are looking at if the distribution of the outcome over time is ‘random’ (so for example, if you thought the exposure had zero/nothing to do with the outcome) or not random (outcome happens right after the exposure or later on or at different times yet highly likely linked to the exposure). This approach assesses whether the exposure (and in this case, the COVID vaccine) changes the likelihood of the outcome being experienced. So we are trying to see if the exposure changes the likelihood of the outcome, based on exposure.
They found (key finding) that the mRNA vaccines linked to an 84% increased risk of cardiac deaths in younger males. Also an increased risk in cardiac mortality in men over 60. Young males 18-39 years show increased risk, clearly due to these mRNA vaccines.
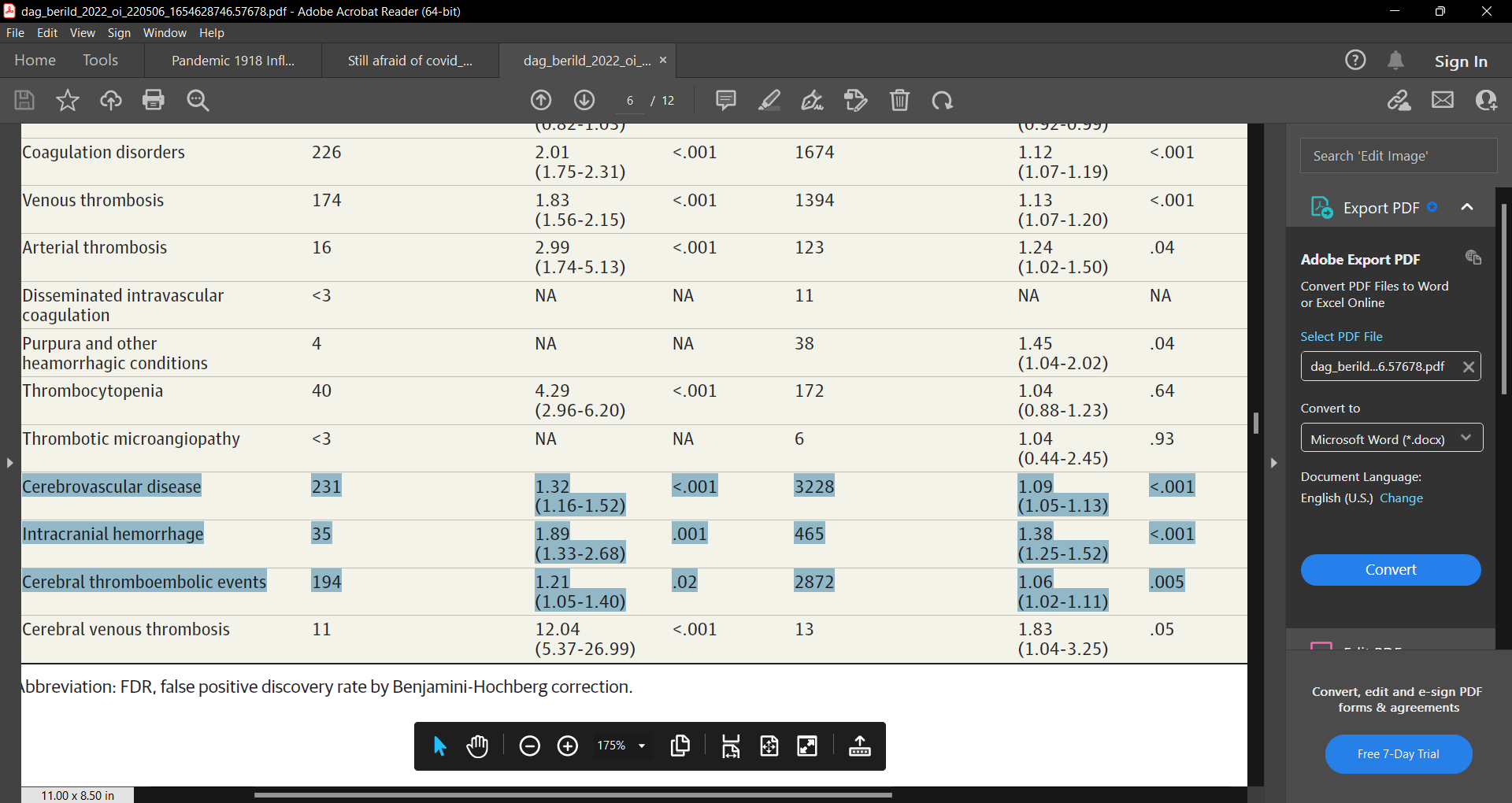
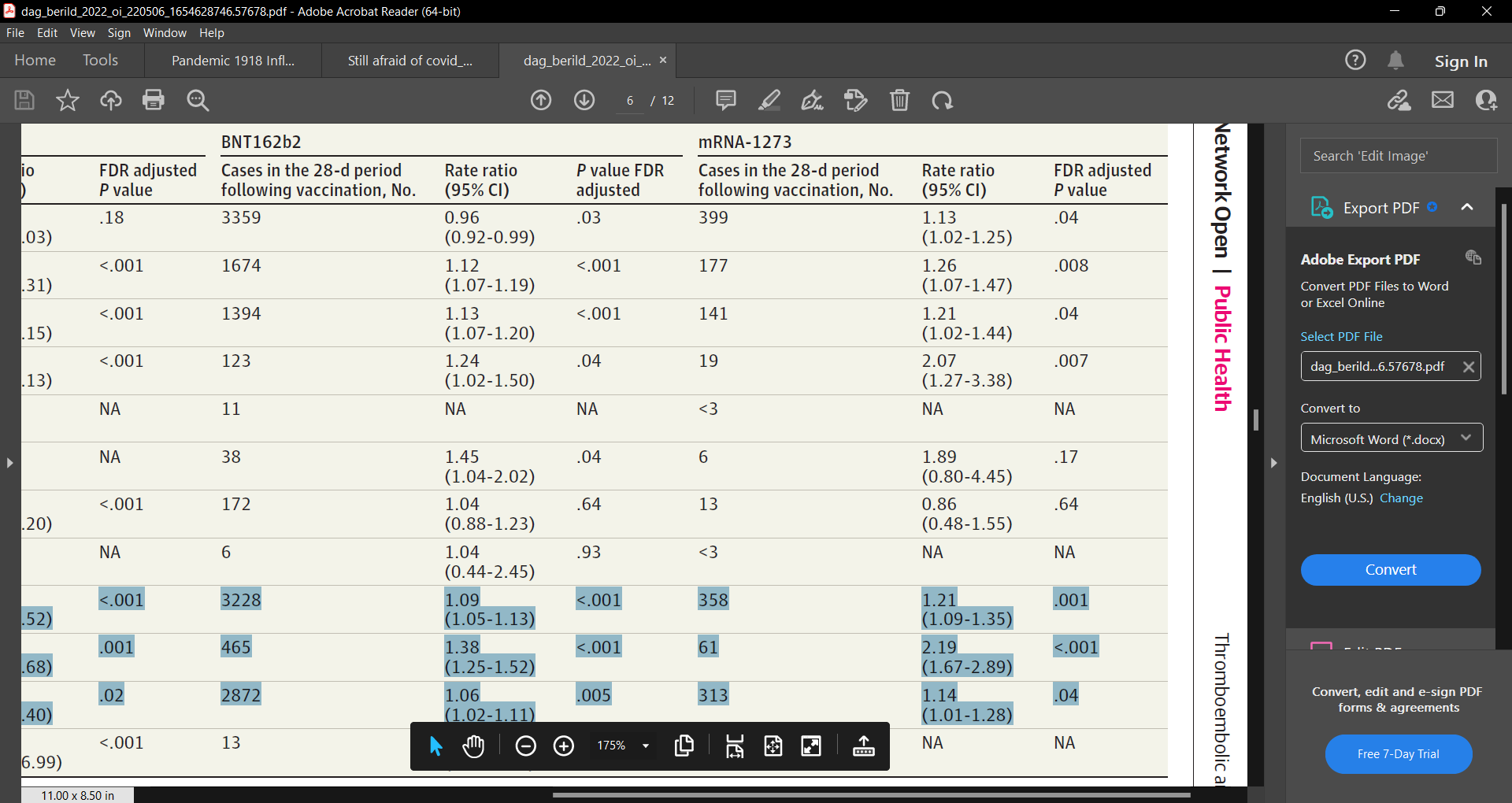
Note, a similar self-controlled case series study (we did not hear the politicized biased Ladapo critics come out to hammer these researchers on the methodology, did we?) published in JAMA Open titled “Analysis of Thromboembolic and Thrombocytopenic Events After the AZD1222, BNT162b2, and MRNA-1273 COVID-19 Vaccines in 3 Nordic Countries” (Jacob Dag Berild), found that there was an increased rate of hospital contacts because of coagulation disorders and cerebrovascular disease, especially for thrombocytopenia and cerebral venous thrombosis, following vaccination with AZD1222 (https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2793348). This was Scandinavian data (Norway, Finland, and Denmark). They also found increases in risk due to the COVID vaccines e.g. intracerebral hemorrhage (e.g. Moderna 119% increased risk signal). There are many studies showing increased risk of myocarditis risk post COVID mRNA vaccine risk.
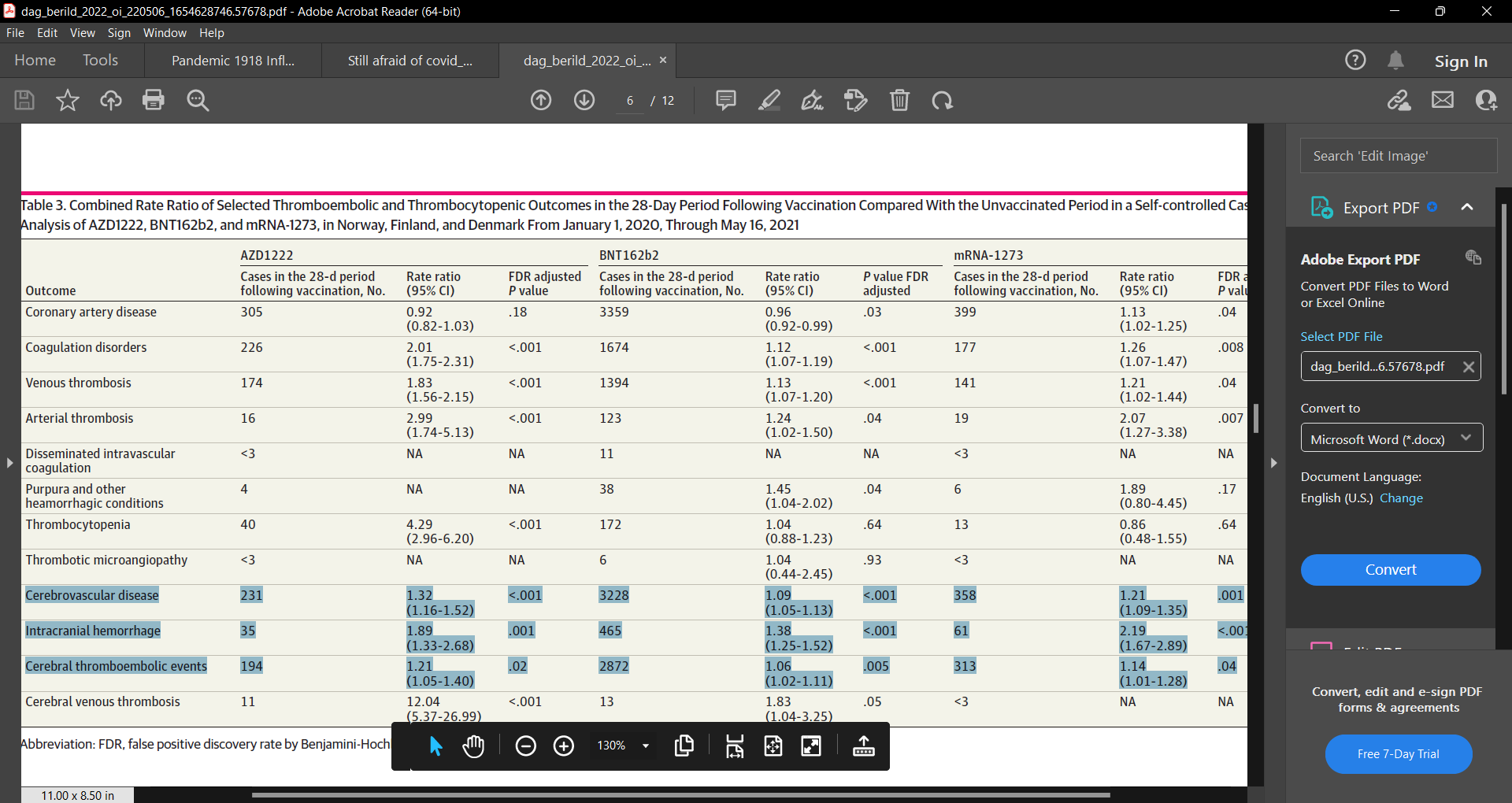
Table above enlarged:
Remember this stunning graph out of Israel I showed in a prior substack? It showed increased risk of cardiovascular events post COVID vaccine roll-out (https://www.nature.com/articles/s41598-022-10928-z).
See graph B:

BTW, my doctorate is in research methods (schooled and supervised and post doc by the founder of ‘evidence-based methods (EBM), Dr. Gordon Guyatt, and thus I MAY, just MAY, know something about what I am saying and I say it as nicely as I can, those who do not know what they are talking about, or simply wish to tear down Ladapo for political reasons and you are a lockdown lunatic COVIDian vaccine “oh I want a vaccine IV drip bag as I can’t get enough as now on the booster treadmill and I cannot get off as I deranged my underlying prior functional natural innate and acquired-adaptive immune system” maniac, should just keep quiet and if I would be so bold, STFU! And go away.
Enter the debate if you have read the issues and come add to the debate, constructively, it should not be a means to ‘catch you’. To destroy. There is enough out there that we have published to school you up on. Go read. Go read the study and read about research methods and then talk your garbage. I suggest you just say thank you to Dr. Ladapo and people like Dr. Harvey Risch and Dr. Ramin Oskoui and Dr. Peter McCullough, Dr. Tenenbaum etc. (as well as myself) for he (and they/we) is/are at least ‘trying’ while you sit in your mommy’s basement in crocs in your flannels pulling fuzzballs from your navels and from in-between your toes, worrying about your summer vacation next year. Folk like Joe is/are trying to save peoples’ lives. Cut the guy slack and give him the praise he deserves, he is doing what you are not.
See my prior substack on this (see also https://www.breitbart.com/politics/2022/10/10/florida-surgeon-general-responds-critiques-mrna-vaccine-guidance/):
Two forces at work here.
1. Paid pharma hit men.
2. Cognitive Dissonance and refusal to look jab lethality in the face, especially those that allowed themselves to take the jab.
if the FDA or any other type of agency in other countries wanted that type of study, they could have had it before the EUA was issued.
so now they are complaining that the original study wasn't done right?
well, now they are stuck with the best study
btw there ware more deaths in the Pfizer RCT of the vaccinated than the placebo before the unblinding. Which is consistent with heart failure in the Florida Study.