

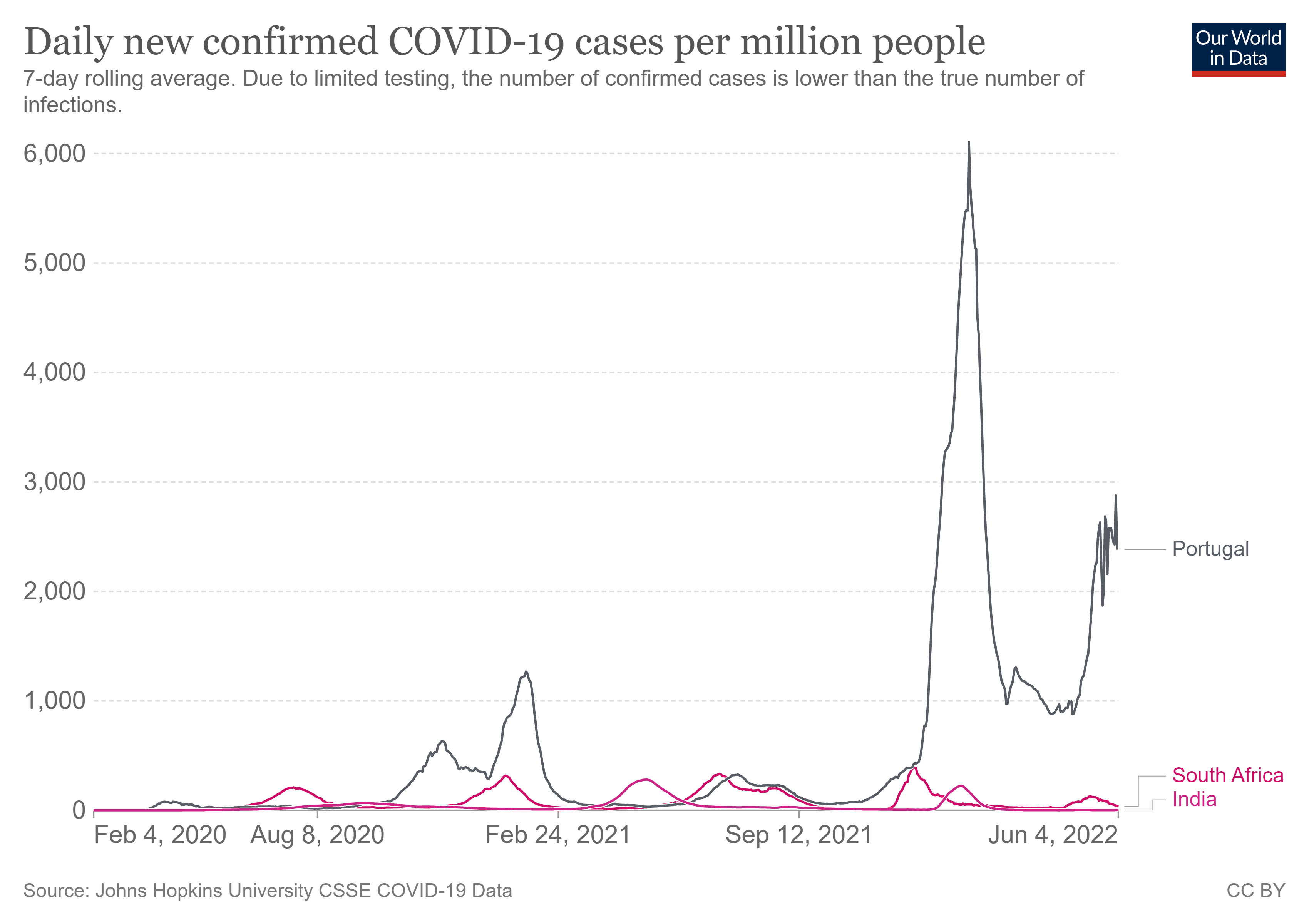
India, Portugal, and South Africa: I update the case graph as of June 4th 2022; why have three nations behaved so differently in recent OMICRON sub-variant (BA 4/5 waves)? In fact, across pandemic?
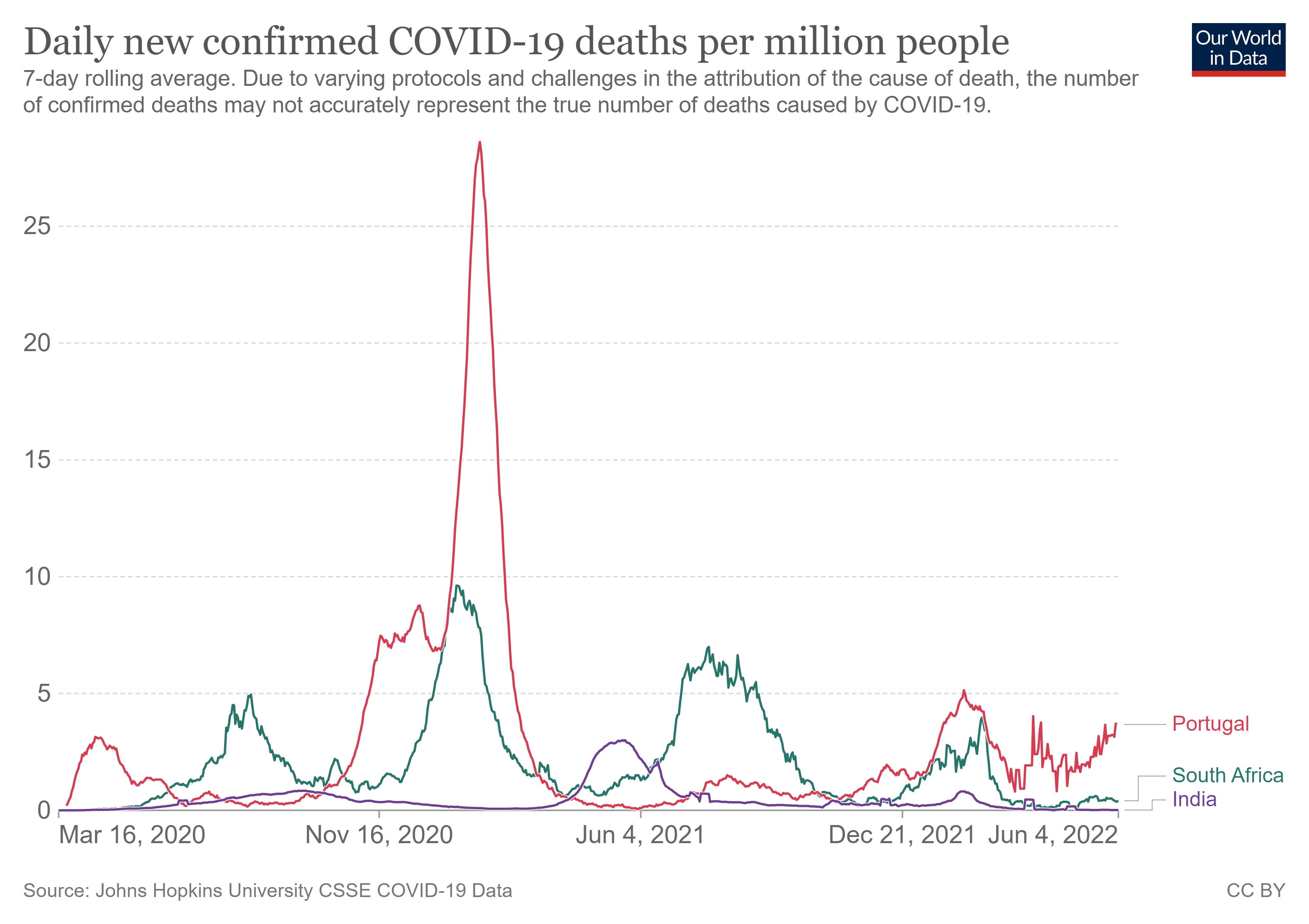
Data as of June 4th: for the less vaccinated South Africa, they handled the BA.4/5 & little deaths, for full vax Portugal (& boosted), huge problems & deaths increasing; why? Look at India & Australia

Once again, throwing out some data and information for debate. All are welcomed to partake as none of us have all the answers and we still try to learn. I do and I am always open to criticism and schooling. I welcome that and yearn to learn daily. We are still trying to understand this and the devastation by these COVID injections, especially the mRNA ones.
Here goes.
The main thesis is that different nations have been confronting the COVID sub-variants quite differently and there is a strong case that this depends on vaccine status/rates. The more vaccinated a nation is, the more infection/re-infection post vaccination, with even hospitalization and death.
This goes back to what others and myself have been saying, in that the unvaccinated in the South African population may be benefitting (very likely), especially the younger persons, from training of their innate immune system from the constant infectious pressure and exposure and re-exposure as the virus is circulating; the innate antibodies (Ab) are becoming trained and learn, in a way a type of ‘memory’ develops though you would know that it is the acquired adaptive immune compartment (systemic compartment) that forms memory (memory B-cells that churn out Abs on re-exposure). This ‘training’ of innate immunity (Abs) allows the unvaccinated to better cope with exposure and the Abs can sterilize/eliminate the virus. The poly-specific low-affinity, broad, innate Abs are not ‘outcompeted’ or subverted by the antigen highly- specific, ‘vaccine induced’ Abs (that are non-neutralizing and so only partially if at all, neutralizes the virus’s spike).
Proportion of population vaccinated:
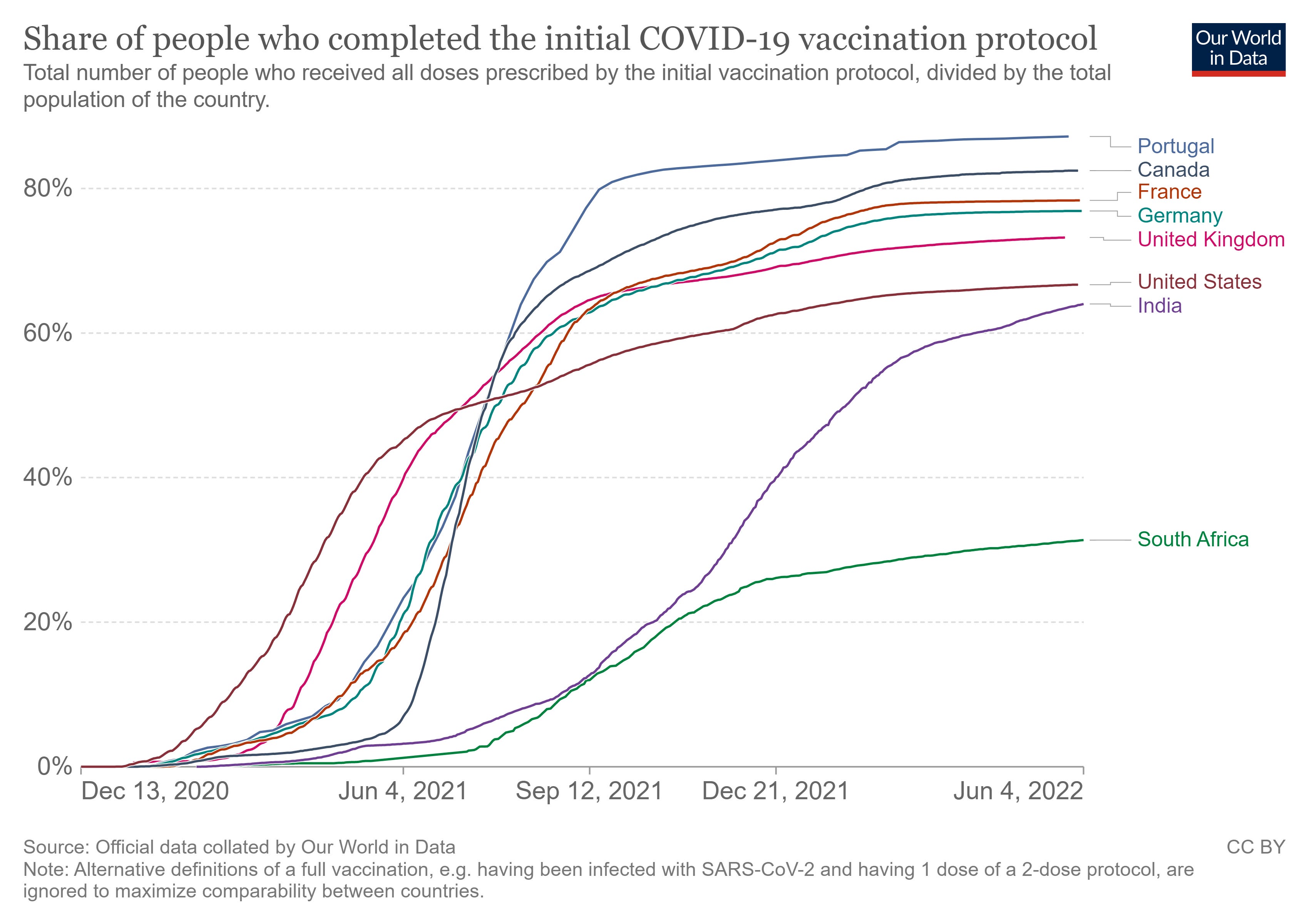
In Portugal on the other hand, the heavily vaccinated (and the population is 80-90% to near 100% vaccinated and boosted) may be contributing to the immune system being subverted and impaired and the non-neutralizing or partially neutralizing Abs (omicron sub-variants are now largely resistant to the vaccine induced Abs) are likely binding to the virus but not neutralizing (or only partially) the spike (preventing infection). The vaccinal Abs binding to the spike may also block the innate Abs from binding, thus the innate Abs unable to sterilize the virus/eliminate it/prevent infection. The innate Abs thus lose their functional capacity to sterilize the virus while being subverted and neutralization is constrained.
Do you see the issue of not coming down to baseline? That infection levels are elevated even after the wave and hangs out there placing tremendous infectious pressure. There is no ‘herd’ immunity when the curves look like this.
Some suggest massive chemoprophylaxis programs societally to reduce the infectious pressure. So that the mounting mass population non-neutralizing Abs have less virus to pressure and thus will have less risk of viral immune escape. What do you think? Problem is societies will not implement that (will not happen) for they still do not ascribe to the potency and role of early treatment and prevention anti-virals in COVID. So infectious pressure must come down via other means.
Look at India’s curves today, still near flat, infection, cases, deaths. Did their aggressive use of chemoprophylaxis and early treatment pre-OMICRON, help them stave of infection, cases, and severe outcomes? I say yes. They also were a nation that benefitted from limited vaccination especially early on (initially, though reports are that they are ramping up vaccination more recently) as there was very massive infectious pressure and their innate immune systems were trained. They are also a much younger population e.g. < 40 years old (South Asian nations are principally younger).
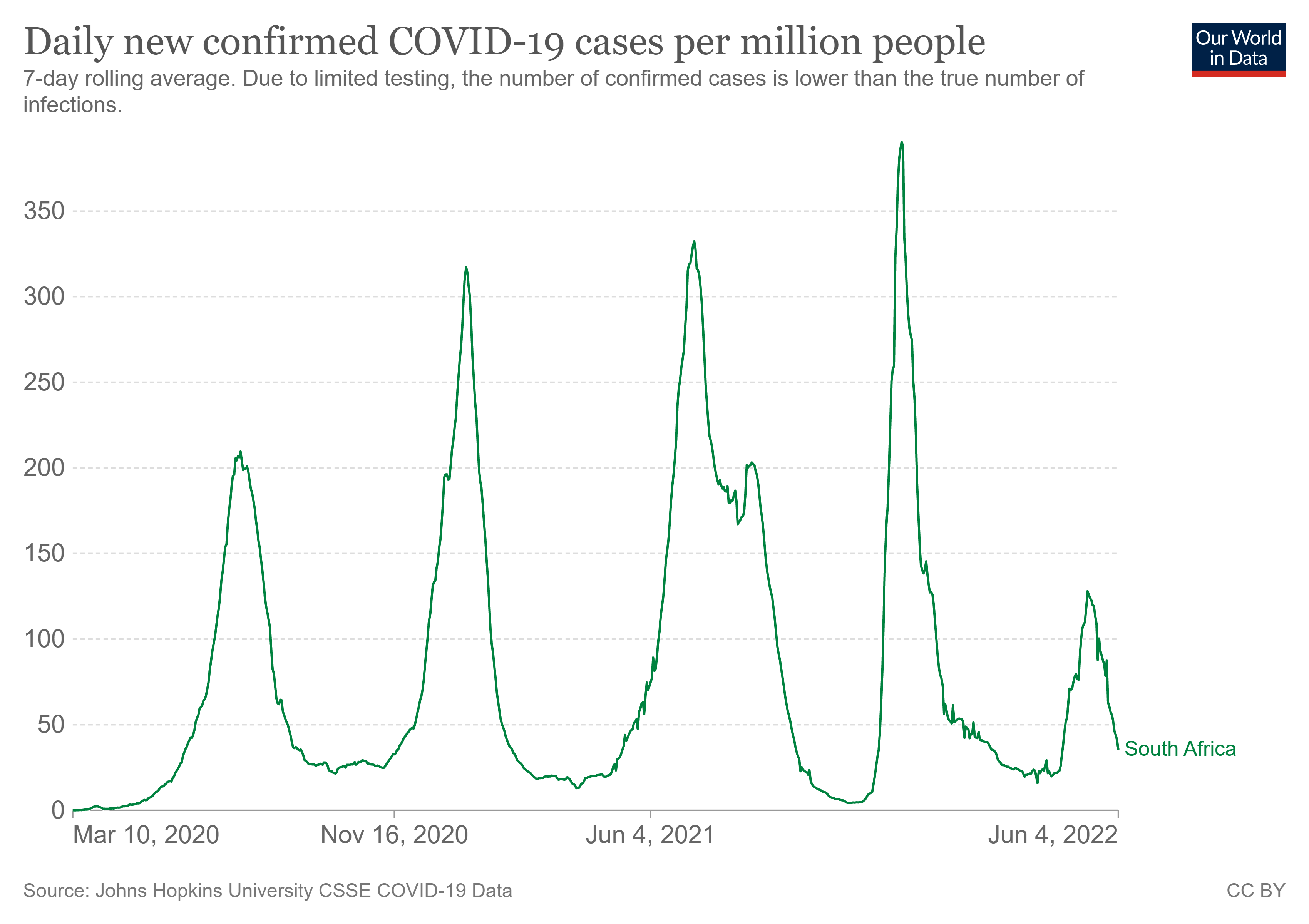
Let us look at the South Africa recent OMICRON BA 4 and BA 5 sub-variant experience with a more blown up graph. See how the peaks get higher each successive curve, they get closer (more rapid), and do not get back to baseline. This is a real huge problem not returning to baseline. Yet see this last 5th wave, it seems that with least vaccinated South Africa, their population has weathered the 5th wave:
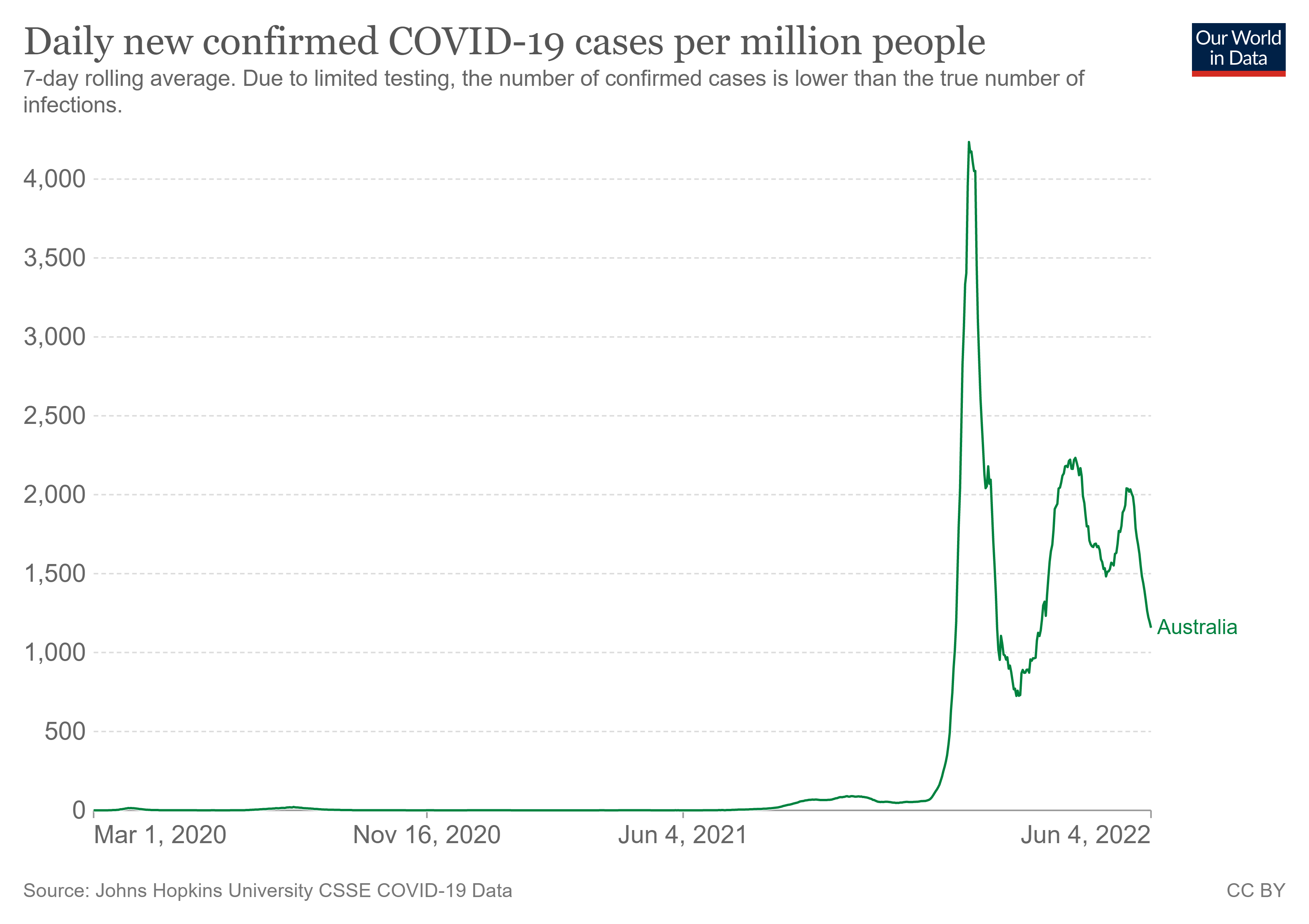
How is Australia doing today with the OMI sub-variants? Do you see the issue with downward side of curves not coming down to baseline?
These two are key studies to keep in mind for further and deeper reading:
“We analyzed data from 1,789 participants (1,298 placebo recipients and 491 vaccine recipients) with SARS-CoV-2 infection during the blinded phase (through March 2021). Among participants with PCR-confirmed Covid-19 illness, seroconversion to anti-N Abs at a median follow up of 53 days post diagnosis occurred in 21/52 (40%) of the mRNA-1273 vaccine recipients vs. 605/648 (93%) of the placebo recipients (p < 0.001).”
This Follmann study shows us alarmingly what the UK data said in week 42, that there was and is subversion of making Abs to the nucleocapsid (more stable ‘conserved’ protein that envelops the mRNA in the core of the virus) in vaccinated persons. This means natural ‘cellular’ immunity (memory) is being impacted and not being induced in vaccinated persons.
I again draw your attention to the seminal study by Yahi et al. “Infection-enhancing anti-SARS-CoV-2 antibodies recognize both the original Wuhan/D614G strain and Delta variants. A potential risk for mass vaccination?”
The key Yahi finding and thus take away phrase IMO is:
“As the NTD is also targeted by neutralizing antibodies, our data suggest that the balance between neutralizing and facilitating antibodies in vaccinated individuals is in favor of neutralization for the original Wuhan/D614G strain. However, in the case of the Delta variant, neutralizing antibodies have a decreased affinity for the spike protein, whereas facilitating antibodies display a strikingly increased affinity. Thus, ADE may be a concern for people receiving vaccines based on the original Wuhan strain spike sequence (either mRNA or viral vectors).”
I sent the following email on this topic a while ago. It supplements what Dr. Alexander is saying.
Igor Chudov has an excellent substack article today, comparing Portugal's experience with that of S. Africa on recent COVID-19 variants (https://igorchudov.substack.com/p/ba5-is-a-variant-for-boosted-people?s=r). Portugal is highly vaccinated and boosted, whereas S. Africa is at the other end of the spectrum.
As Chudov says: "
Both countries are experiencing a “BA4/5” wave
It was no big deal for South Africa
The same wave is deadly for the overboosted Portuguese and the deaths keep rising
Covid looks to be “mostly over” for unvaccinated South Africa and is “only getting started” for totally vaccinated and mostly boosted Portugal."
He states further: "this current wave of infections and deaths in Portugal is driven by reinfections. Why are reinfections happening? Because boosted people are unable to acquire proper immunity upon infection. Thus, they are forced to endure endless Covid reinfections, that further damage their immune systems, inviting more illness."
This outcome was predictable. In a Trial Site News OpEd (https://www.trialsitenews.com/a/have-we-entered-a-self-sustaining-modus-operandi-for-covid-19#comments), I proposed that those who were "vaccinated" against COVID-19 entered into a self-sustaining modus operandi where they effectively became addicted to the COVID-19 shots. The shots themselves suppressed the innate immune system, and opened the recipient to emergence of dormant viruses, cancers, autoimmune diseases, etc. They also made the recipient more vulnerable to infections such as COVID-19, and that's what Chudov is observing in Portugal. If one chooses not to take the boosters, then the waning immunity that follows the shots will result in negative vaccine effectiveness, where again the recipient becomes more vulnerable to infections. That's the self-sustaining situation we are observing. While Chudov focuses on Portugal, this transition to negative vaccine effectiveness has been observed in the UK, New Zealand, Canada, and other countries.
Geert is again being proven right, which is why some now only have non allopathic antivirals combinations to fall back on. But they don't know this, yet.
I'm working up these and have a vested interest as a vaxxed person already infected me with BA.2 and Ivermectin is effectively a prohibited drug in many countries. Berberine with silymarin works just as well by all accounts.
I'm currently collating research on Artemisia.
Therapeutic properties of Berberine,
A literature review.
https://doorlesscarp953.substack.com/p/therapeutic-properties-of-berberine?s=w