

Mass Murdering Of The Elderly; "Midazolam (paralytic) depresses respiration and it hastens death. It changes end-of-life care into euthanasia." - Professor Patrick Pullicino; so I have to ask, with
diamorphine, propofol, Lorazepam, Fentanyl etc., why the fcuk did we do this to our precious elderly? When 95 times of 100 they were false-positive' for COVID as part of the PCR-created fake pandemic?

IMO, hospitals, nursing homes, old-aged home, care homes, long-term facilities etc. used midazolam, these paralytics, to kill people, they knowingly used them as mass murder of our elderly and high-risk vulnerable…the fucking doctors, yes, our medical doctors, the CEOs of hospitals, the government officials at Health Canada, PHAC, CDC, FDA etc., in Canada, US, UK, Australia etc. must be dragged into a court and shackled in trial and made to defend their actions, and if judges say they casued death, then we hang them there…right there. only if judges say so.

The Daily Beagle; THE UNDERDOG
'‘

When talking of a government sponsored mass murder, what do you imagine they would do? How do you imagine it would play out?
Escorting of the elderly one-by-one into some sort of death chamber? Have roving execution vans? Rounding the elderly up into quarantine camps or FEMA camps and delivering a lethal blow?
These are all very over-the-top, overt, obvious things to look for.
What if, surviving members of Nazi Germany’s government, had intended to learn from their mistakes, of what went wrong and their subsequent failures?
Avoiding Resistance
So instead of high key, overt mass murders that are obvious to everyone — invoking a sense of outrage and resistance — they adopted a more low key, subtle approach? How would that look?
Instead of killing the elderly in giant, overt death camps, they quietly came to their care homes and killed them there. Instead of publicly declaring the executions, they smudged and misreported and reclassified the deaths.
Instead of boldly proclaiming the killings, they quietly lied and denied. Instead of using just one approach to kill, they used several, that if the elderly didn’t die by extreme neglect, then they denied supporting family access and killed them by lethal shot.
This is an in-depth dive. What you are about to read will shock you.
Enter Midazolam
Originally highlighted by Jikkyleaks, Midazolam is a benzodiazepine, a class of ‘depressant’ drug. A depressant is a type of chemical that reduces or impedes a certain activity or activities within the body.
Midazolam, like many other benzodiazepines, is a CNS depressant. CNS stands for ‘Central Nervous System’, and the central nervous system regulates things like movement, breathing, heart beat and more. If it involves a muscle, chances are it involves the central nervous system.
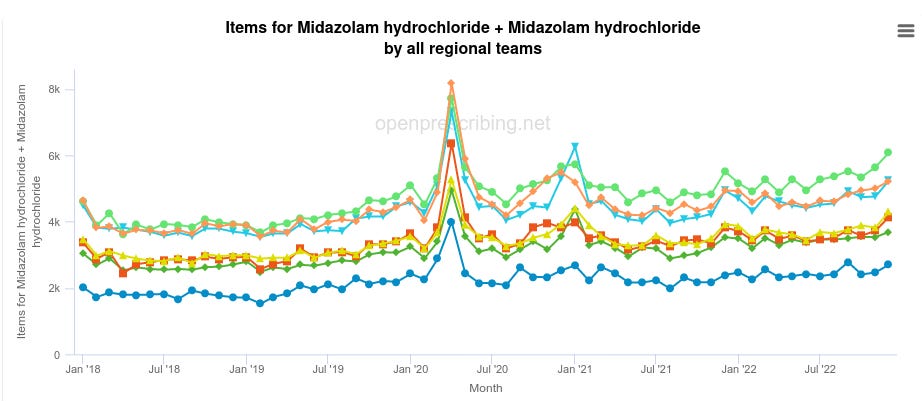
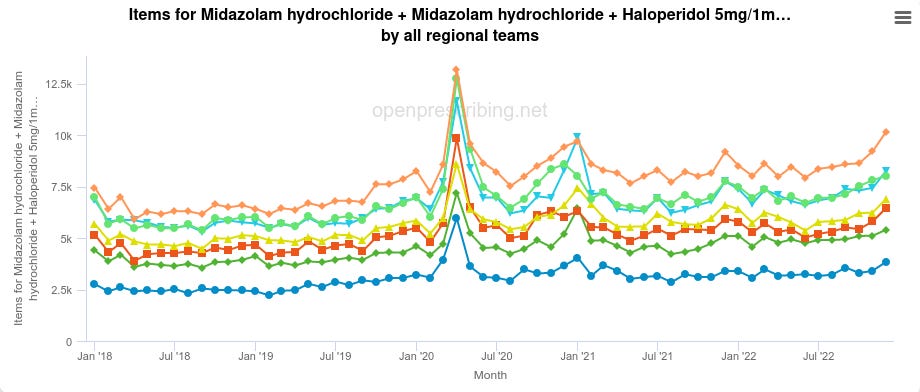
In April 2020, Midazolam prescriptions skyrocketed.
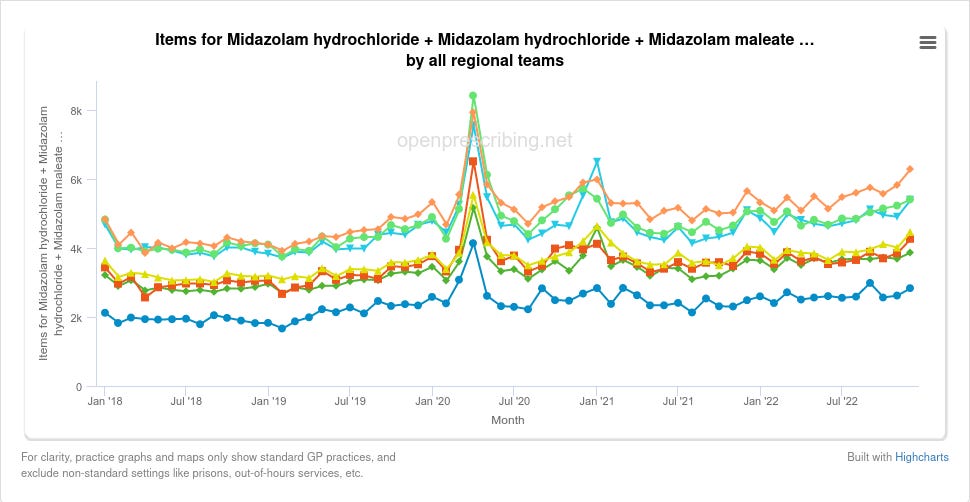
The prescriptions were for Midazolam Hydrochloride, and Midazolam Maleate:

Midazolam Hydrochloride (AKA Midazolam HCL) is the injectable form:
Midazolam Maleate is the oral form:
The majority of the prescriptions were for the injectable form (~97%):
It is unlikely these drugs were taken willingly or with consent given the oral form exists and was not used so extensively.
The Use Of Midazolam
On 3rd April 2020 — NICE (National Institute for Health and Care Excellence) issued guidance NG163 (NG — NICE Guidance) — which recommended the use of benzodiazepines, including Midazolam, for mere “agitation or distress”:
Lorazepam is mentioned, but unlike Midazolam, we don’t see the giant spike in April 2020 for Lorazepam.
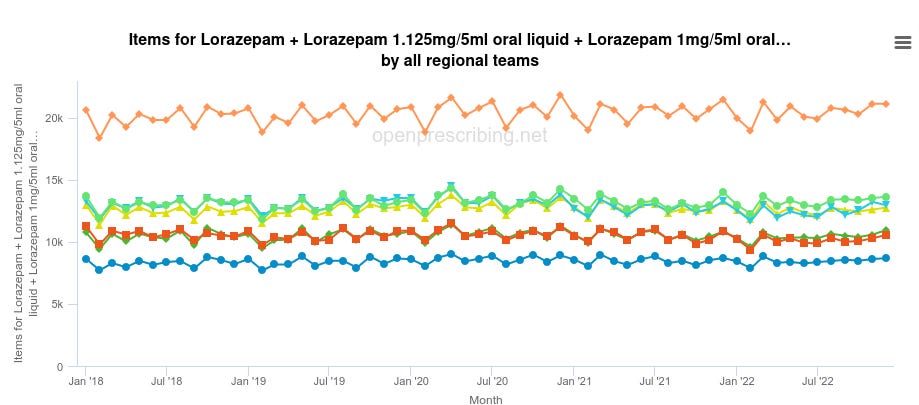
This is likely due to the fact “Midazolam has a faster onset and shorter duration of action than other benzodiazepines such as diazepam and lorazepam lending itself to greater flexibility in dosing than other benzodiazepines”.
The NICE guidance tells administrators of the Midazolam shots to ignore any concerns they might have about causing suffocation (“respiratory depression”; where the patient is unable to breathe due to finding it harder and harder to move their lungs using their diaphram):
Sedation and opioid use should not be withheld because of a fear of causing respiratory depression
Yet within NG163 it contradicts this advice underneath and says benzodiazepines do not have a marketing authorisation “for this indication or route of administration”:

That is to say, what they’re doing is illegal and medically unsound, and NICE know it.
In a two-faced move, a month prior, NICE issued contradictory guidance in a failed attempt to exonerate themselves from the planned mass murder campaign:

Healthcare professionals are advised to only co-prescribe if there is no alternative and, if necessary, the lowest possible doses should be given for the shortest duration.
Does this chart look like they were given the ‘lowest possible doses’ for ‘the shortest duration’?
The UK government also contradicted NICE’s advice:
benzodiazepines (and benzodiazepine-like drugs) and opioid medicines (opioids) can both cause respiratory depression; when used together, additive effects on the central nervous system increase the risks of sedation, respiratory depression, coma, and death
Additive means ‘stacks up’, so the combination of both benzodiazepine-like drugs and opioids has a stacking effect on impeding the ability for the elderly to breathe. Even if, incomprehensibly, you believe this was to “treat” SARS-CoV-2, if SARS-CoV-2 is a respiratory virus, impeding their ability to breathe essentially amounts to assisting their deaths.
End Of Life
Midazolam is used in so-called ‘End of Life care’ (also known as ‘Palliative care’), which is double-speak terms for administering drugs that ‘help’ patients they think are dying to pass on faster, often painted as ‘easing their passage’, when instead it makes things like breathing more difficult.
Midazolam literally causes patients to fall asleep, as one study notes using it as an ‘antipsychotic’ over Haloperidol:
Evidence for the superiority of midazolam over haloperidol for managing motor agitation is encouraging, but it is overly sedating and the majority of patients treated with midazolam fell asleep after intramuscular administration (Mendoza 1987).
Interestingly, as highlighted by Dr John Campbell, injectable Haloperidol — the aforementioned antipsychotic drug — had prescriptions that spiked during April 2020:
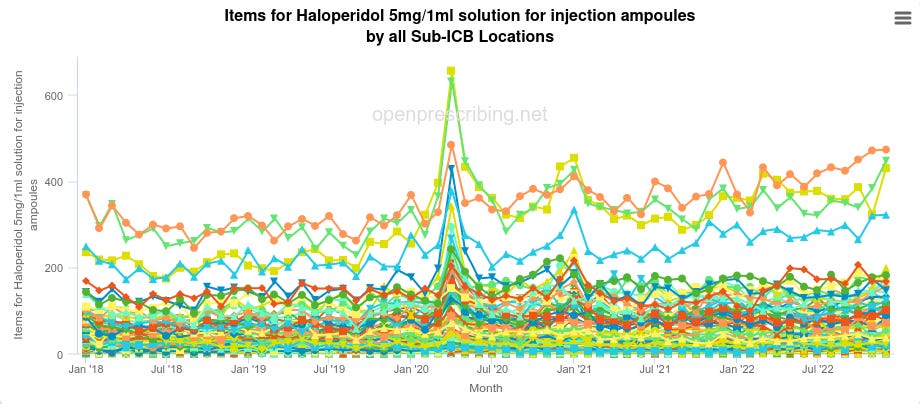
Haloperidol has been shown to cause increases in mortality in the elderly, where:
[…] most of the deaths appeared to be either cardiovascular (e.g., heart failure, sudden death) or infectious (e.g., pneumonia) in nature. […]
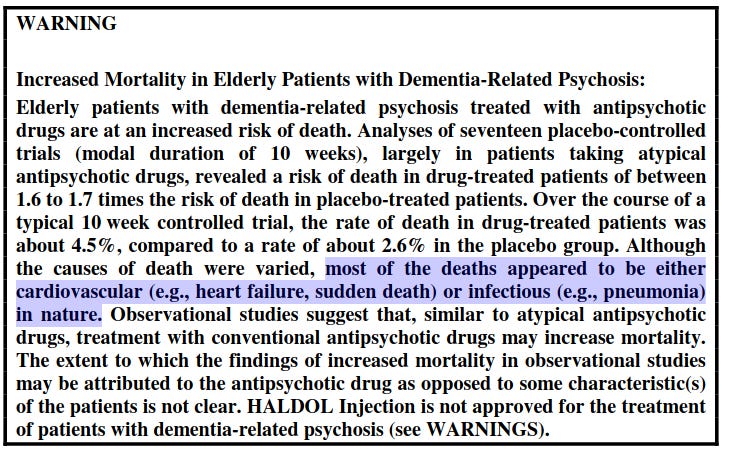
If that sounds vaguely familiar, it ought. Pneumonia is a generalised term for inflammation of the lungs. The same symptomology as COVID-19.
How convenient — administer a drug that causes the same symptomology as COVID-19, then administer another drug to “treat” it resulting in deaths.
Also highlighted by Dr John Campbell was Levomepromazine (AKA Nozinan, Levoprome, Detenler, Hirnamin, Levotomin and Neurocil), is a phenothiazine neuroleptic drug, another antipsychotic drug, also used in ‘palliative care’.
Prescriptions for injectable Levomepromazine also spiked in April 2020:

Levomepromazine is used by NICE as a sedative.
You can see all the drugs prescriptions spiking together in April 2020:
It is unclear how causing someone to fall asleep with Midazolam, sedating them with Levomepromazine, giving them pneumonia and heart issues with Haloperidol, would aid in their breathing clearance or recovery, especially if NICE guidance recommends continual dosage.
Midazolam works so well at depressing the Central Nervous System that in 2009 the New South Wales (NSW) Ministry of Health recommended it for use in epilepsy to stop convulsions in children. The study goes on to note that: “Repeat doses may be effective but increase the risk of complications”.
Notice that the drugs are essentially used to control people with neurological (mental) disorders and spasms. Not breathing disorders.
Harmful Drugs
That is to say, these drugs are not beneficial drugs that bring treatment to a respiratory disease, nor do they aid with breathing, nor do they offer viral clearance, nor secondary bacterial clearance, nor do they supply nutrients, nor oxygen, nor are they intended to help a patient to recover. They either sedate or kill.
At the time of the previously published Cochrane review, there was no evidence for a beneficial effect of benzodiazepines for the relief of breathlessness in people with advanced cancer and chronic obstructive pulmonary disease (COPD).
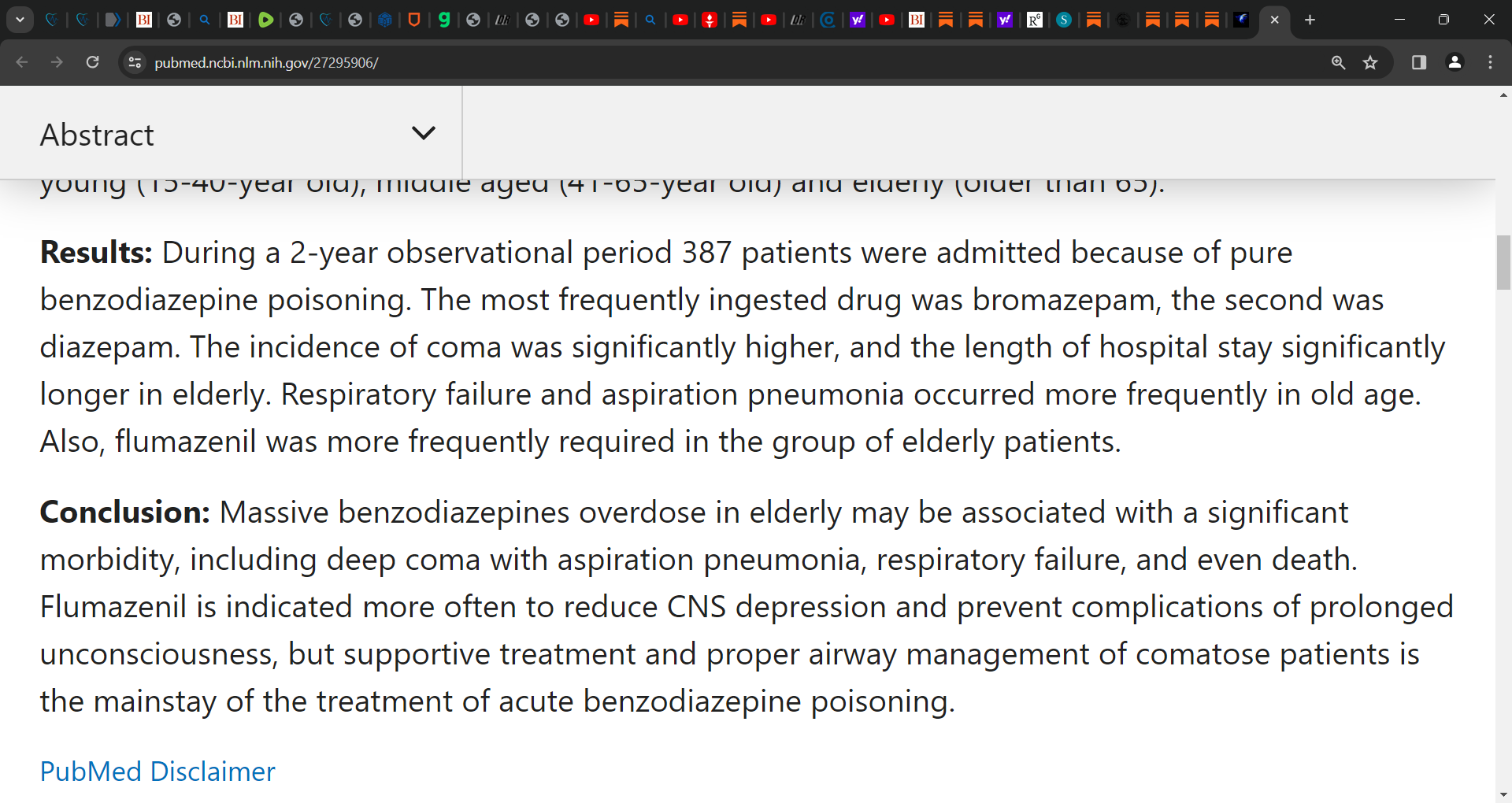
“Benzodiazepine poisoning in elderly”:
Elderly may be at greater risk compared with younger individuals due to impaired metabolism and increased sensitivity to benzodiazepines.
Massive benzodiazepines overdose in elderly may be associated with a significant morbidity, including deep coma with aspiration pneumonia, respiratory failure, and even death.
They are designed to sedate a patient, reduce movement to such a degree they can halt epileptic seizures in their tracks, and when it comes to breathing, greatly impede survival chances when paired with opioids — by the UK government’s own admittance.
[…] increase the risks of sedation, respiratory depression, coma, and death
Elderly Deaths Reclassified; Spike Three-Fold April 2020
Naturally, all these Midazolam overdose deaths have to go somewhere, right?
Well, they weren’t classified as what they are — overdose deaths:
2019: “4,393 deaths related to drug poisoning were registered in 2019 in England and Wales”
2020: “4,561 deaths related to drug poisoning were registered in England and Wales”
2021: “4,859 deaths related to drug poisoning were registered in 2021 in England and Wales”
As you can see, barely the slighest increase in deaths. So, where were the majority of deaths from April hidden?
They were reclassified as dementia deaths. A neurological (mental) disorder that retroactively “justifies” the use of an antipsychotic drug. This isn’t mere speculation either, there’s a peer-reviewed paper stating as much:

Read that again:
[…] 17 316 patients died in England in April, 2020, with “dementia and Alzheimer's disease” recorded on their death certificate. This number of deaths was nearly three times more than expected […]
Over 17 thousand elderly patients died in April 2020; the same month NICE published guidance to use Midazolam regardless of the consequences; the same month Midazolam injectables shot up, the same month 17,316 patients died, three times greater than normal, supposedly from a mental disorder (that mysteriously just cropped up during the peak start of a pandemic)…
…The same month antipsychotic prescriptions shot up:
[…] the overall number of registered patients meant that the proportion of patients who have been prescribed antipsychotics substantially increased […]
Rates in March, April, and May, 2020, were substantially higher than in the same months in 2018 (increased by 4·40%, 6·95%, and 5·22%, respectively) and 2019 (increased by 4·28%, 7·34%, and 4·87%, respectively).
…The same month they were “overrepresented” in the additional deaths
People with late-stage dementia and those within care facilities, who would be the group most likely to be prescribed antipsychotics, were over-represented among the additional deaths in April, 2020
…The same month no justification could be found for the increased prescriptions:
The register does not record specific indications for antipsychotic prescribing, and it is possible that some of the increase related to delirium management or palliative care, although most of the increase was probably in response to worsened agitation and psychosis secondary to COVID-19 restrictions
…where the paper tries to blame “worsened agitation” or “psychosis secondary” caused by lockdown for the sudden jump in mass injections of ‘antipsychotics’.
Whistleblowers Reported Misuse
Back in July 2020, The Daily Mail ran a story asking the question “did care homes use powerful sedatives to speed Covid deaths?”:

The Daily Mail claimed whistleblowers “witnessed misuse of sedatives, with staff told to give them to dementia patients”. The justification? To stop them ‘wandering corridors’. But no mass murder campaign could be based on such a trite reasoning.
The article quotes a number of experts who concur it was nothing but a death machine:
Retired neurologist Professor Patrick Pullicino, who was instrumental in raising concerns a decade ago that the Liverpool Care Pathway was bringing forward patients’ deaths, believes the jump indicated something similar had happened. He said: ‘Midazolam depresses respiration and it hastens death. It changes end-of-life care into euthanasia.’
Professor Patrick Pullicino goes on to observe that:
[…] an official flow-chart intended to help health workers decide if people sick with Covid-19 were suitable for intensive care wrongly consigned those deemed too frail to end-of-life care.
[…] to me this flow-chart encouraged use of end-of-life sedation with midazolam – effectively resulting in euthanasia pathways.
Eileen Chubb expressed that care home workers were under the definite impression not to save elderly lives by sending them to hospital, invoking the neglect portion of the mass murder campaign:
Eileen Chubb, of the charity Compassion in Care, said a number of care-home workers had told her sedatives were used too freely during the pandemic, adding that some staff were under the ‘definite impression’ that very sick care-home residents should not be sent to hospital.
Lie And Deny
Dr Amy Proffitt, a shill for the mass murder campaign, tried to insist that Midazolam would be an “obvious choice” for breathing difficulties and that it wouldn’t “hasten or prolong someone’s death”, despite the fact it makes breathing more difficult, and is not authorised for such usage, and results in death, as admitted by even the UK government:
Dr Amy Proffitt, of the Association for Palliative Medicine, said: ‘I absolutely do not believe that there have been cases of euthanasia in care homes related to Covid-19.’
She said a rise in the use of midazolam was to be expected because the drug would have been an obvious choice to give to those with problems breathing, a symptom of coronavirus.
[…] midazolam will not hasten or prolong someone’s death – it will just give comfort,’ she added.
With such a blatant lie exposed so publicly, with so many fudged statistics coming out of the UK government on mortality data, we can no longer trust these deceivers.
Happening Worldwide
Similar happened in other countries with similar types of drugs over a similar timeframe, such as in Canada:
From March to September 2020, absolute increases were found in the mean monthly proportion of nursing home residents who received prescriptions for antipsychotic medications, antidepressant medications, and trazodone compared with January to February 2020
The study goes on to declare that it was ‘disproportionate’ and did not match other drug prescription trends:
Although absolute increases in prescribing were small, they were disproportionate to expected secular prescribing trends from April 2018 to February 2020, and they were distinct from observed prescribing changes for other drugs during the pandemic.
The study goes on to admit these drugs are also not typically used for those ‘dying of COVID-19’:
Although psychotropic medications may have been prescribed for residents who were dying of COVID-19, drugs such as antidepressants and trazodone are not typically used for acute palliative management
Before us, we have overwhelming evidence of a systematic mass murder campaign of the elderly, organised by the government.
The causation — NICE guidance recommending Midazolam — is undeniable, the follow-on — the mass purchases of Midazolam — is undeniable, and the study showing a mass increase in the use of ‘antipsychotics’ of which Midazolam can be classified as, leading to deaths, is undeniable.
Now what, dear friends?
Evil comes from a failure to think. It defies thought for as soon as thought tries to engage itself with evil and examine the premises and principles from which it originates, it is frustrated because it finds nothing there. That is the banality of evil.
— Hannah Arendt, The Banality of Evil’
Yes, it was mass murder. I put out flyers everywhere in person because Google wouldn’t let me post anything especially with scientific background. I renamed my flyer so that I could send it ...Google stopped it every time. REMDESIVERE takes out the organs. The only thing that killed patients in hospitals was protocol. To intubate lungs that were already filled with fluid was and is murder. Wearing a mask caused sepsis and sent many people to the hospital and then to top it off. ...Substances put in the mask also cause Covid. The test caused Covid. To be a sacrifice for science is murder. I just wish more people would have looked at the science. I wish main stream media would have cared more for the public than their freaking job! Yes, it was and remains mass murder. And how many years has this been going on?
Not only was it used in Covid to execute elderly and chronically ill, it is and has been used for years in Hospice. Some of the already “awake” or knowledgeable having been blowing the whistle on this for a few years. Me in 2018 & 2019 at the Senate Whistleblower Luncheon and subsequent three day Whistleblower Summit in DC. The QALY (quality adjusted life years) scoring for the economic valuation of life = Death Panel, has sent thousands to be executed that were NOT terminal. Hospice pays very well by the government three letter agencies. Sound familiar…. like Covid incentive payouts(payoffs) to kill? Most have no idea Hospice requires a prescription for Nutrition and Hydration! Does that sound “compassionate to you? Our Medical Industrial Complex has been murdering, executing and torturing patients long before the plandemic. The same root cause was the motivation of greed, moral belief that the bureaucrats are “God’s given a right to decide life value and Government corruption!!! Those of us sounding the alarm in 2018 & 2019 were simply viewed as lunatics to suggest hospitals and physicians would kill for many. The “Silver Lining” of covid corruption was the mass exposure of the CEO’s, CFO’s, CMO’s that have no conscience if a profit can be made. You can google NancyGPaul Cheryls Legacy on youtube to see my participation in a panel trying to warn others long before.