
RSV: the plot thickens as to the link between COVID gene injections and RSV: "Skewed Fate and Hematopoiesis of CD34+ HSPCs in Umbilical Cord Blood Amid the COVID-19 Pandemic" (Estep) & "Respiratory
RSV: the plot thickens as to the link between COVID gene injections and RSV: "Skewed Fate and Hematopoiesis of CD34+ HSPCs in Umbilical Cord Blood Amid the COVID-19 Pandemic" (Estep) & "Respiratory
syncytial virus in hematopoietic cell transplant recipients and patients with hematologic malignancies" (Khawaja); 3 studies that shed light with exploding RSV; did we screw our kids with COVID jabs?

Are the COVID-19 mRNA gene injections (vaccines) the reason why we are seeing this explosion of RSV across the US and Canada? Was it the lockdowns and school closures that weakened and dampened a normally functional immune system in children? Is it the worthless, ineffective, and harmful blue surgical and white cloth (man-made) masks? Was it social distancing, shielding? That children could not tax and tune up, boost their immune systems, and train their innate immune systems during a critical window? I say all of these caused this heightened risk, and this substack focuses on the impact of the COVID gene injection vaccine and risk for RSV.
Is the COVID gene injection crippling the immune system? Are we witnessing antibody-dependent enhancement of infection (ADEI) and antibody-dependent enhancement of disease (ADED) due to the sub-optimal COVID vaccine induced vaccinal antibodies (Abs) that are not fully matured and at its maximal ‘affinity’ binding capacity, as such driving enhanced infection with RSV? Are COVID vaccinated infants and children at heightened risk of infection with RSV than unvaccinated children?
What we do have now is Pfizer in an urgent panic for the mRNA injections have failed and Paxlovid has failed (and they will be investigated), so now it is on its money making agenda pushing a maternal RSV vaccine to protect infants against RSV. Again, they are withholding data and engaging in a promotional media hype campaign and I am willing to bet the study will be small sample size, short duration, will have bogus non-patient important outcomes as the primary outcome, will not study safety, and will be sub-optimal and woefully inadequate methodologically. As all of their prior studies have been, case in point, the famous 8-mice study used to gain EUA from corrupted FDA for the bivalent booster (based on the Wuhan and BA.4/BA.5 spike).
I wrote about RSV and the corruption in a prior substack that I re-highlight here for background, essentially that I argue we are being played societally by Pfizer, the media, and the medical establishment. I do not think medical doctors understand that they have zero credibility. None today based on what they did during COVID.
Truth is that the necessary comparative effectiveness ‘trustworthy’ high-quality research on RSV is lacking yet some intriguing research is raising questions directed at stem cells. Is there a link with the destruction of Hematopoietic Stem Cells by the COVID gene injections? How would we remedy this destruction of Hematopoietic Stem Cells, if so? This needs urgent study for this would support Vanden Bossche’s call to stop the vaccine in children as to subversion of the innate immune system (innate Abs and natural killer calls (NK)) on the one hand, but we are beginning to see other ways via which the COVID gene injection vaccine can be deranging and devastating in children and it appears that RSV surges and the link to Hematopoietic Stem Cells may hold the answer, at least in part. This is worth considering.
Yet has there actually been a surge in RSV or is this idiosyncratic? It appears that there is an increase. There is a reported 7-times increased risk of hospital admission for RSV in 2022 (in infants and children) over prior years (2018)? Why?
‘About 171 out of every 100,000 infants younger than 6 months were hospitalized with RSV for the week ending Nov. 12, according to the CDC’s surveillance system that tracks 12 states. That is more than double the RSV hospitalization rate for newborns last year and more than seven times the rate in 2018, the last complete season before the Covid-19 pandemic.’
Dr. Geert Vanden Bossche has shared an e-mail among colleagues and one paragraph I wish to share for it carries good news:
“as more and more children get infected with RSV, their innate immunity will get better and better trained and we’ll probably soon see a steep decline in cases (just like we previously witnessed with SC-2-mediated cases of MISC!). The more the kids get their innate immunity trained (due to SC-2, influenza or…. live attenuated childhood vaccines!), the lower the incidence of RSV will become. Of course, one could try to make people aware that all of this is due to the mass vaccination and that we need to stop this.” (GVB, personal electronic communication, November, 20th, 2022).
With this background, let me explain at a 50,000 foot level, how the COVID-19 gene injection may indeed be the culprit in this massive spike in RSV. I stand on the shoulders of immunology, virology, and vaccinology giants like Vanden Bossche, Yeadon, Risch, McCullough, and Bridle. I have learnt much from Geert Vanden Bossche and I describe in lay terms my interpretation best I can (my own view on what is happening), and will follow this by highlighting three (3) studies that also open up the stem cell etiology link. Note, I am not an immunologist or virologist, my training is in evidence-based medicine and epidemiology. Note also, we operate in a ‘black-box’ arena at present so bear this in mind.
I/we can argue that yes, the COVID injection is potentially linked to the surge in RSV in children. How? Well four potential ways may shed light (I explain not as an expert in immunology like GVB but I will try my best to explain in terms of how I understand this):
i)If we induce vaccinal antibodies (via a vaccine) that are indeed fully mature, developed, and perfect (are allowed to develop fully), with high-affinity (high binding ‘full affinity’), yet now face a virus that differs (a circulating variant) than the one the vaccinal antibodies originally targeted, then ADEI and ADED can develop; as such, the antibodies will still recognize the circulating variant but does not match the antigenic constellation (antigens on the surface of the virus); it thus can still recognize the virus variant and bind but cannot neutralize it (it cannot neutralize it as the vaccinal Abs do not match the target antigen e.g. the spike protein epitope binding sites on the new variant); this binding however (but not neutralization) enhances the uptake of the antibody-virus complex into host cells that are susceptible to the virus variant and can promote replication of the virus and thus we get ADEI (that could also lead to ADED). There is potent viral immune escape. Remember, the vaccinal Abs were induced to the initial legacy Wuhan strain of COVID and now faces a virus variant with antigen targets (mutations) that differ (small variations can cause antigenic drift while major recombination and differences can cause antigenic shift). This happens not only for coronavirus, but with other glycosylated virus and other pathogen.
ii)Another way that this ADEI and ADED can also happen is without vaccination. We refer to natural infection. For example, if you were infected with the initial Wuhan strain, and then exposed to and infected quickly (maybe in a few weeks) with another variant e.g. Delta or Omicron, then the vaccinal antibodies that were induced, will not be able to match with the new variant and this can result in ADEI and ADED. Thus this need not only be via the vaccine. There will be binding of the vaccinal Abs to the antigen (epitopes) but this binding and no neutralization enhances the uptake of the antibody-virus complex into cells that are susceptible to the virus, and can promote replication of the virus and thus we get ADEI and ADED.
iii)Also, with a variation to point i) above if we were dealing with Abs that did not yet fully mature and reach its full affinity, maximal binding capacity and thus full neutralization capacity. If the vaccinal antibodies were not fully mature and did not get to its maximal developed ‘binding affinity’ (its full affinity to the antigen e.g. when vaccinating in the midst of a pandemic when virus is circulating and thus the Abs are not allowed to fully mature yet still bind), then this can also result in ADEI and ADED. For example, if you are vaccinating into a pandemic across all age-groups (and in this case also infants and children, young persons) and the population is mounting an immune response (that is sub-optimal as the vaccinal Abs are not yet developed), then the problem is that the induced vaccinal Abs are confronted with virus that is circulating.
Remember, there is ongoing massive infectious pressure (still is today) as omicron is still circulating and other sub-variants are emerging. The vaccinal Abs did not yet reach its maximal binding affinity as this needs time to develop (from 1st prime to boost etc. and thereafter, several weeks e.g. 2-4). If there is not the right amount of time, then the virus is not just waiting around, it will try to infect and the Abs will bind. The vaccinated person that is mounting an immune response does not yet have a fully developed immune response yet confronted with virus. Abs being immature and not fully developed with high binding capacity affinity, will bind to the target antigen yet in binding, the vaccinal Abs will not bind properly and strongly and will thus not neutralize the virus. It will not stop infection, replication, or transmission. This causes multiple variants as the virus replicates and those variants that can overcome the sub-optimal immune pressure will become enriched and the dominant ones are selected forward e.g. omicron BA.5. The point is that the embroidered complex of virus with bound Abs that do not neutralize it, enhances the uptake of the antibody-virus complex into cells that are susceptible to the virus and thus one is at risk for ADEI and ADED.
iv)We know that vaccine induced Abs (from the COVID gene injection vaccine as an example) are high-affinity and can bind more strongly to the target antigen than innate antibodies of the innate immune system (e.g. in infants, children). The innate immune system in children must be initiated and ‘started out’ and trained once the maternal antibodies begin to wane at about 4-6 months post birth. Thus the induced vaccinal Abs (high-binding affinity) will outcompete the innate Abs (that are lower-binding affinity) for the target antigen (the binding epitopes on the spike protein), and will bind and block the innate Abs. The result is the training will not occur (as innate antibodies must bind to viruses to be educated on them (on how to handle them immunologically) and thus can educate and train the innate immune system. You thus have vaccinal Abs that are a mismatch for the antigen and thus cannot neutralize it (as well as not yet reached its full binding affinity post vaccination) that are still binding, and in so doing blocking the innate Abs that are low affinity yet broadly potent that could neutralize the virus. The child then is very vulnerable to infection and disease (ADEI and ADED). This training of the innate immune system is not only for COVID virus but a broad range of other viruses like RSV.
In short, children need to be allowed the time for their innate antibodies to bind to viruses in the environment and to thus train the innate immune system and the COVID injection subverts this. Proper innate immunity responding and training is subverted. Also, if parents are thinking of injecting their children with COVID gene injection, they should ensure that the children receive their proper immunization schedule (via live attenuated replication competent vaccine (virus) before they get the COVID injection. This will ensure that the innate antibodies can at least educate the innate immune system on the various glycosylated viruses that children will encounter and must have immunity for. Innate Abs must be able to bind to virus in order to train the innate immune system (and NK cells) on how to handle viruses the child will encounter in the future.
Thus, if we vaccinate children and infants with the COVID injection before this critical window of training occurs (before the innate Abs can bind and educate the innate immune system on the virus), then the innate immune system will he hobbled as it will not have been educated on i)how to confront pathogen now e.g. omicron ii)how to confront other glycosylated pathogen/virus in the future (that share similar surface patterns and molecules) and iii) will not be trained on how to recognize ‘self’ from ‘non-self’ components (self-like, self-mimicking) and thus the child will be susceptible to auto-immune diseases. It is critical that the child’s innate immune system (with training of the natural killer cells (NK cells)), be afforded this training so as to not attack the child.
Thus it is very possible and highly likely that the COVID gene injection vaccine has subverted the innate immune system of children and sidelined the innate antibodies from its proper functional capacity training. The result is the COVID injection is crippling the immune system. It is likely now that innate antibodies (post COVID vaccine) are not handling the RSV virus optimally and not neutralizing it. Normally, with proper innate Ab function that educates and trains the innate immune system and NK cells, the innate immune system will recognize other glycosylated viruses (with similar surface patterns e.g. sugars, glycans etc.) and a broad range of virus and pathogen. It is likely now we subverted and damaged the innate immune system of children, and instead of the innate immune system effectively handling RSV, the child is actually at heightened risk of infection (and subsequent disease).
What do the following 3 studies I wish to highlight say, as to the stem cell-RSV-COVID gene injection vaccine link? These studies raise a very interesting and troubling hypothesis that the COVID injection is damaging stem cells and
SOURCE 1:
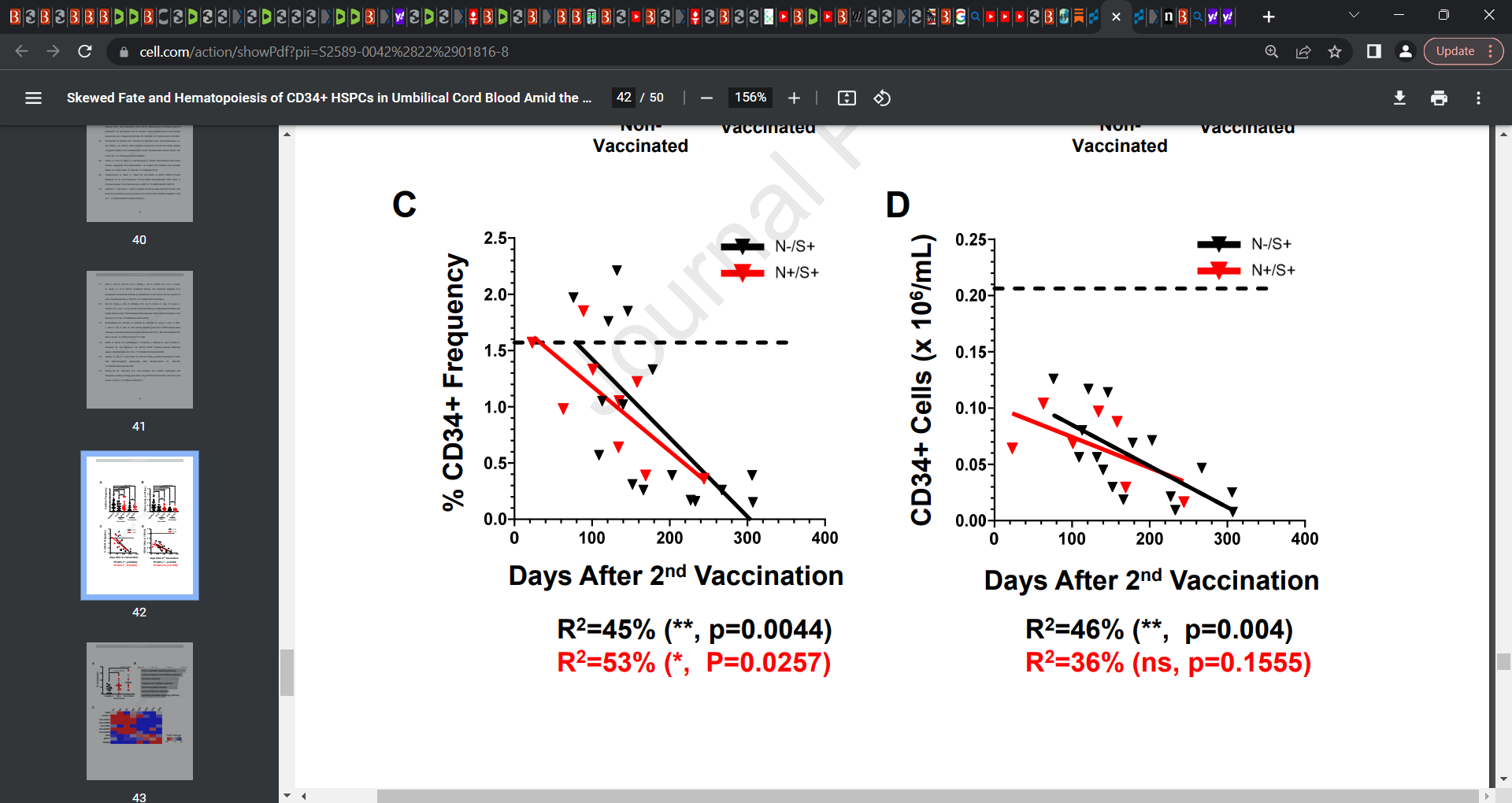
Estep et al.: Skewed Fate and Hematopoiesis of CD34+ HSPCs in Umbilical Cord Blood Amid the COVID-19 Pandemic
These researchers raised the prospect that COVID-19 gene injection vaccination (as well as natural infection) plays a role in impairing the functionalities and survivability of hematopoietic stem progenitor cells in umbilical cord blood.
“Umbilical cord blood (UCB) is an irreplaceable source for hematopoietic stem progenitor cells (HSPCs). However, the effects of SARS-CoV-2 infection and COVID-19 vaccination on UCB phenotype, specifically the HSPCs therein, are currently unknow. We thus evaluated any effects of SARS-CoV-2 infection and/or COVID-19 vaccination from the mother on the fate and functionalities of HSPCs in the UCB.
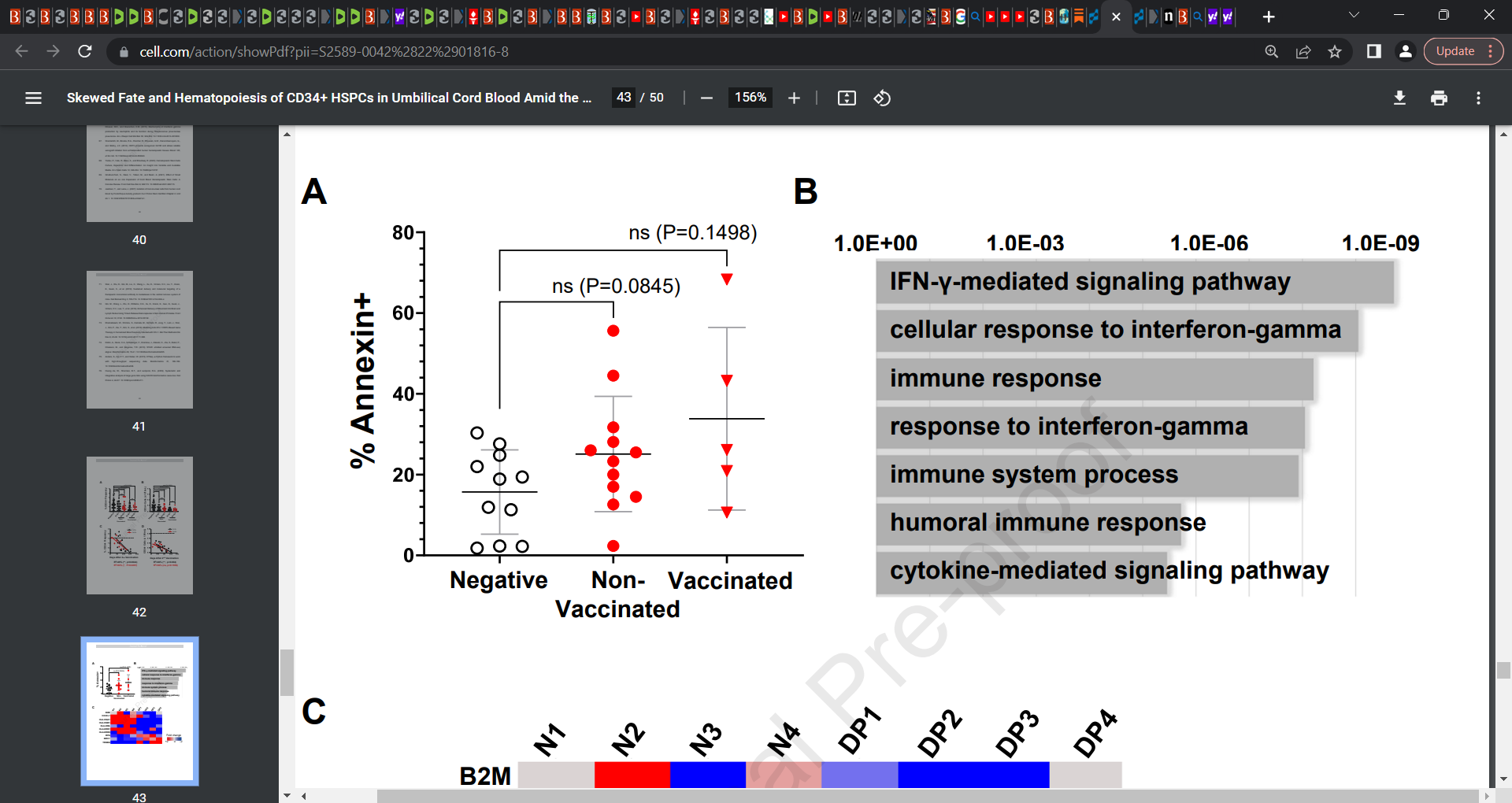
The numbers and frequencies of HSPCs in the UCB decreased significantly in donors with previous SARS-CoV-2 infection and more so with COVID-19 vaccination via the induction of apoptosis, likely mediated by IFN-γ-dependent pathways.
Two independent hematopoiesis assays, a colony forming unit assay and a mouse humanization assay, revealed skewed hematopoiesis of HSPCs obtained from donors delivered from mothers with SARS-CoV2 infection history. These results indicate that SARS-CoV-2 infection and COVID-19 vaccination impair the functionalities and survivability of HSPCs in the UCB, which would make unprecedented concerns on the future of HSPC-based therapies.”
“Reduced CD34+ cell frequencies and thus lower CD34+ cell numbers were observed in the UCB from the nonvaccinated but previously infected donor group and even more so in the vaccinated donor group, which was attributed to the induction of apoptosis. Furthermore, these reductions in CD34+ cell numbers & frequencies correlated with the timing of the 2nd -vaccination in donors ― the numbers & frequencies inversely correlated with the period after the vaccination until delivery, indicating that factors causing these damages are maintained over the gestation period. In addition, the CD34+ cells, which would be residual cells following apoptosis, showed skewed hematopoiesis profiles, indicating that previous SARS-CoV-2 infection, and likely vaccination based on the observed trends, interferes not only with the fate of CD34+ cells but also the hematopoietic abilities, phenotype, and survivability of populations thereof, which could result in a shortage of available CD34+ HSPCs from cord blood banking, processing for use towards HSPC-based therapies, as well as unpredictable hematological issues in HSPC recipients.”

SOURCE 2:
Khawaja & Chemaly: Respiratory syncytial virus in hematopoietic cell transplant recipients and patients with hematologic malignancies
The review study examined Hematopoietic cell transplant (HCT) recipients and patients with a hematologic malignancy (HM). The researchers reported that “One of the most common community respiratory viruses that may lead to the death of HCT recipients and HM patients is respiratory syncytial virus (RSV),4–10 whose incidence is second only to that of influenza according to prior reports;4,5,8,11,12 other viruses include parainfluenza virus, metapneumovirus, adenovirus, rhinovirus, and bocavirus.” The findings appear to indicate that HCT and HM patients (limited or absent stem cells) are at a much elevated risk of RSV (higher mortality) and more problematic RSV.
“The most significant complication of RSV infection in HM patients and HCT recipients is progression to LRTI, which is associated with a higher mortality rate.5,20,22,24,25,42–51 Many risk factors for progression have been identified in the hopes that target populations that could benefit from early therapy could be identified.”
“High mortality rates have been reported in HM patients and HCT recipients with RSV infection. RSV-attributable mortality rates in HCT recipients vary between 0% in outbreak situations,48,62,67 in which some patients received reduced-intensity conditioning regimens,62 and 43% in other circumstances.5,20,22,24,25,42–51 When HCT recipients develop RSV LRTI, the mortality rate can range from 21% to 83% 4,31,42,43,45,46,48,68 Of note, when HCT recipients with RSV infections were classified into those with possible RSV LRTI (only radiological evidence of chest abnormalities and negative or no bronchoscopy data) or proven RSV LRTI (RSV detected in the lower respiratory tract),31 the mortality rate increased from 0% to 26%, respectively.31 Multiple other risk factors for mortality from RSV have been identified, most of which are host-related, including neutropenia and lymphopenia, time from transplant to infection, cell source, older age, steroid exposure, graft-versus-host disease, hypoxia, and the use of myeloablative chemotherapy.25,42,43,46,47 The RSV-ISI has been validated to predict mortality risk in HCT recipients12,53,56”
SOURCE 3:
More evidence exists that COVID-19 spike protein damages hematopoietic stem cells and ties into the prior 2 mentioned studies (Source 1 and Source 2). Researchers specifically reported that “Mounting evidence accumulates that hematopoietic stem/progenitor cells (HSPCs) and endothelial progenitor cells (EPCs) are damaged during severe SARS-Cov-2/COVID-19 infection”. What does this mean? Well we can extrapolate that if spike protein from infection can damage stem cells, then it is more than likely the same damage will occur due to the spike protein generated from the COVD gene injection.

Effect of COVID-19-derived SP (20 nM, S1 + S2 ECD, His tag) and rhACE2 (20 nM) after 16 h exposure of UCB-sorted HSCs (A) and EPCs (B) on activation of caspase-1 evaluated by Caspase-Glo® 1 Inflammasome assay (Promega). Experiments were repeated three times *p < 0.01 and **p < 0.001. C, D Nlrp3 inflammasome inhibitor MCC950 recovered clonogenic potential of UCB HSPCs from the inhibitory effect of COVID-19-derived SP. Cells were exposed to SP ± MCC950 (10 µM). The data show the number of CFU-Mix (C) and CFU-GM (D) clonogenic progenitors obtained from UCB HSPCs. HSPCs were cultured in methylcellulose medium supplemented with appropriate cytokines, and CFU-Mix and CFU-GM colonies were counted using inverted microscope after 14 and 11 days of culturing. The data are presented as means ± SEM. Experiments were repeated three times #p < 0.01. Effect of COVID-19-derived SP (S1 + S2 ECD, His tag) after 16 h exposure of UCB-sorted HSCs (E) and EPCs (F) on activation of caspase-1 evaluated by Caspase-Glo® 1 Inflammasome assay (Promega). rhACE2 (20 nM) and TLR4 blocking agent (TAK-242, 5 μM) we employed alone or together. Experiments were repeated three times **p < 0.01 and #p < 0.0001. G SP-mediated activation of Nlrp3 inflammasome in CD34+ HSPC was inhibited in a presence of MCC950 (10 μM).
Now, have others opined on this RSV-COVID injection vaccine link?
The Vigilant Fox does a nice touch on this topic and huge praise for the scholarship:

Jaxen presents some Pfizer and Moderna data also worth considering:
‘And they did so using FDA documents involving Pfizer and Moderna’s own clinical trials.
Moderna
Two to Five-Year-Olds

Within 28 days after vaccination, some respiratory tract-related infections were reported with greater frequency in the mRNA-1273 group than in the placebo group. Events of pneumonia were reported by 0.3% and 0% 0f mRNA-1273 and placebo recipients, respectively. Respiratory syncytial virus (RSV) infection was reported by 0.4% and <0.1% of mRNA-1273 and placebo recipients, respectively.
“So FOUR TIMES THE AMOUNT OF RSV in the vaccinated group compared to the unvaccinated group that hadn't received it,”
Moving on to Six to Eleven-Year-Olds

Within 28 days after vaccination, some respiratory tract infection-related PTs were reported more frequently in the vaccine group compared to the placebo group, such as Respiratory syncytial virus infection (0.3% vs 0%) and Upper respiratory tract infection (3.9% vs 2.5%).
“So you're giving a shot to kids that's INCREASING their upper respiratory tract infections with RSV quite a bit, actually,”
Pfizer
Six-Month to Four-Year-Olds (Third Dose)

SAEs (serious adverse events) reported in the BNT162b2 group included RSV bronchiolitis (5 participants).
SAEs reported in the placebo group included bronchiolitis or RSV bronchiolitis (3 participants).
Igor Chudov also did excellent scholarship in his RSV piece:

Remember.... NOBODY has focused on the potential damage to the FETAL THYMUS gland from the C19 vaxxx ! All of the lipid nanoparticles from the vaxxx are also concentrated in fetal thymus gland. The fetal thymus gland is the SEED of T-cell lymphocytes for the entire human lifetime.
https://gettr.com/post/p1z1zfr6457
What is the thymus?
The thymus is a small gland that’s part of your lymphatic system. Your lymphatic system is made up of a network of tissues, vessels and organs such as your tonsils, spleen and appendix. Your lymphatic system is a part of your immune system. It helps defend against infection and disease
The primary function of the thymus gland is to train special white blood cells called T-lymphocytes or T-cells. White blood cells (lymphocytes) travel from your bone marrow to your thymus. The lymphocytes mature and become specialized T-cells in your thymus. After T-cells have matured, they enter your bloodstream. They travel to your lymph nodes (groups of cells) and other organs in your lymphatic system, where they help your immune system fight disease & infection.