

The Wellness Company’s (TWC) Spike Support recovery formula contains Nattokinase (natural blood thinning fibrinolytic) & may help in the rash of pulmonary embolism (lung clots) following mRNA shots
Alike 'silent' heart myocarditis after the mRNA COVID shots that is being seen, people could also be afflicted with fatal lung blood clots unknowingly & is catastrophic! Thromboembolism is serious!

Devastating and often fatal pulmonary embolism (lung clots) following the mRNA technology gene injections are becoming a routine occurrence while the media remains silent and the government health agencies such as CDC, NIH, FDA, Health Canada, SAGE, PHAC etc. pretend there is no link to the COVID mRNA gene injections.
I present evidence of the potential risk of thromboembolism (lung blood clots) after the COVID mRNA technology based gene injections and raise the good news about TWC’s Spike Support formula that contains NATTOKINASE blood thinning. This may be an option as the science fully matures and is refined as to the benefits of NATTOKINASE. Lung blood clots can be fatal (often) and both women and men are afflicted.
TWC’s revolutionary Spike Support Formula is the only product that contains Nattokinase and dandelion root, researched to block and dissolve spike proteins inside your body.
You may consider getting the daily Spike Support and protecting you and your family against the effects of COVID, vaccines, and shedding.
Spike Support Formula contains all natural, non-GMO, scientifically-supported ingredients:
Nattokinase has been researched to dissolve spike proteins and blood clots. Plus, it's soy-free.
Dandelion root may prevent spike protein from binding to your cells.
Selenium to help reduce stress, aiding in helping the body repair itself and recover.
Black sativa extract may facilitate cellular repair.
Green tea extract provides added defenses at the cellular level through scavenging for free radicals.
Irish sea moss is mineral-rich and could help rebuild damaged tissue and muscle.
See link to product here:
https://www.twc.health/collections/covid19/products/long-haul-formula?ref=Paul
Dr. Peter McCullough’s presentation here is riveting and really links the Spike Recovery with NATTOKINASE as a possible support solution to handle the ravages of the spike protein:
SOURCE:
https://rumble.com/v2i7r9u-hearts-destroyed-by-myocarditis-this-spike-protein-is-a-killer.html
Evidence of lung blood clots after the mRNA technology gene injections? Yes, strong, a strong temporal link, biological plausibility etc. I present cases including evidence by my coplleague Dr. Makis (substack):
These cases are often being referred to as vaccine-induced immune thrombotic thrombocytopenia (VITT).
People are reporting adverse effects of the mRNA technology gene injections and need support now. Silent myocarditis and lung clots etc. may benefit from the natural blood thinning dissolving action of NATTOKINASE (similar substances) and TWC’s Spike Support formula may hold benefit in dissolving the spike protein (from the virus as well as COVID gene injection). The mRNA technology gene injection is proving to be deadly and people must read and reflect and consider low-risk options such as NATTOKINASE as we move past and try to recover from the effects of the gene injection which in my mind have been catastrophic.
To me, and I know you too, it was criminal to experiemnt on humans with untested unsafe mRNA technology and we are paying the price. This was money making God like complex people (so called scientists, yet I call them criminals especially the vaccine makers) who cared not one bit about the implications of their lab experiments, just fame and money and nobel prizes. The deaths accumulating post COVID mRNA injections rests at their feet. We will never forget and we will get accountability and justice in the right legal forums. People are waking up!
For example:
1)
SOURCE:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9295046/
This person took the Moderan mRNA technology shot and developed lung blood clots. Vaccine-induced immune thrombotic thrombocytopenia (VITT) was highly suspected.
This person was ‘initially treated with low molecular weight heparin (enoxaparin sodium) for the first 3 days, and direct oral anticoagulants (dabigatran 110 mg twice daily) was added thereafter’.
‘Thromboembolism is a safety concern with these vaccines, especially adenovirus (AstraZeneca) vaccines. However, although not rarely reported, mRNA vaccines have also been associated with the risk of thromboembolism, especially in East Asian populations. Herein, we describe a previously asymptomatic patient who presented with acute pulmonary embolism shortly after receiving the Moderna mRNA-1273 SARS-CoV-2 vaccine.’
Here is a 70-year-old East Asian male, a current smoker who had a prior medical history of ‘hypertension and an old cerebrovascular accident, with independent activities of daily living.’
This man got the ‘first dose of the Moderna mRNA-1273 vaccine 5 weeks prior to this episode.’ He presented to emergency department with ‘progressive shortness of breath for 5 days. A physical examination revealed blood pressure of 120/70 mmHg, heartbeat of 102 beats per min, and SpO2 around 90%. Resting 12-lead electrocardiography revealed sinus tachycardia and a typical S1Q3T3 pattern. Laboratory data showed normal platelet count, hemoglobin and fibrinogen levels. A SARS-CoV-2 polymerase chain reaction was negative. The D-dimer level was 4895 ng/mL, and chest computed tomography angiography showed bilateral saddle pulmonary embolism.’

Bilateral pulmonary embolism noted on computed tomography angiography (white open arrows).
‘To further survey the pulmonary embolism, we conducted examinations in order to verify the possible etiology, including autoimmune disease markers (including antinuclear antibody, C3, C4, lupus anticoagulant, anticardiolipin immunoglobulin), tumor markers (including CEA, alpha-fetal protein, CA199, and PSA), coagulant function tests (including protein C function, antithrombin III, prothrombin time, partial thromboplastin time), all of which were within normal limits. Protein S function was 25.4% (normal value 62.6-150.4%) and the anti-platelet factor 4 (PF4) antibody titer was 50.01 ng/ml (cutoff value of 50 ng/ml) with an optical density of 0.424 units (weakly positive, cutoff value of 0.4 units). Left popliteal vein thrombosis was found by peripheral Doppler sonography.’

Peripheral Doppler revealed probable thrombus with partial occlusion at the right popliteal vein (white open arrow).
2)
Here is another case of a 59-year-old man who presented ‘with a 2 week history of sudden onset dyspnea and a week history of productive cough. No associated chest pain or hemoptysis. No preceding history suggestive of leg pain/swelling. The patient had the booster dose of Moderna (mRNA) COVID-19 vaccine a month before the onset of symptoms.’ This case is presented as a likely COVID-19 Vaccination Associated Bilateral Pulmonary Embolism.
SOURCE:
https://www.hindawi.com/journals/cripu/2022/9596285/
3)
Here is another case of a 24-year-old male patient who presented to the Hematology clinic ‘for management of a recently diagnosed right lower extremity deep venous thrombosis (DVT) and PE. His medical history is unremarkable, with no previous thrombotic events reported. Two months earlier, he had received the second dose of Pfizer BioNTech mRNA COVID vaccine. Twenty-four hours post vaccination, the patient started to experience left sided pleuritic chest pain which was not relieved by paracetamol.’
SOURCE:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8791702/
Dr. Makis evidence here (see his substack):
Boise, ID - 42 year old photojournalist Theresa Marie Palmgren died suddenly on April 5, 2023 while at work from pulmonary embolism (click here)

St.Louis, MO - 27 year old artist and Twitch streamer Katlyn “Katie” Mae Cuneo died suddenly (from pulmonary embolism) on March 17, 2023
Guatemala - Pennsylvania mother of two boys, 27 year old Rocio “Rose” Michelle Roberts died suddenly on March 15, 2023, 4 days after giving birth, from a pulmonary embolism.
Eugene, OR - 46 year old Bethany Jessica Scott Price, age 46, died of a pulmonary embolism on March 6, 2023, according to those familiar with her death (click here)
UK - 31 year old beauty therapist Gemma Harries collapsed and died Jan.16, 2023. She was found to have blood clots in her lungs and legs (click here)

UK - 41 year old Clare Duffy went to take a nap after waking up with a sore shoulder and died suddenly of pulmonary embolism on Jan.8, 2023 (click here)
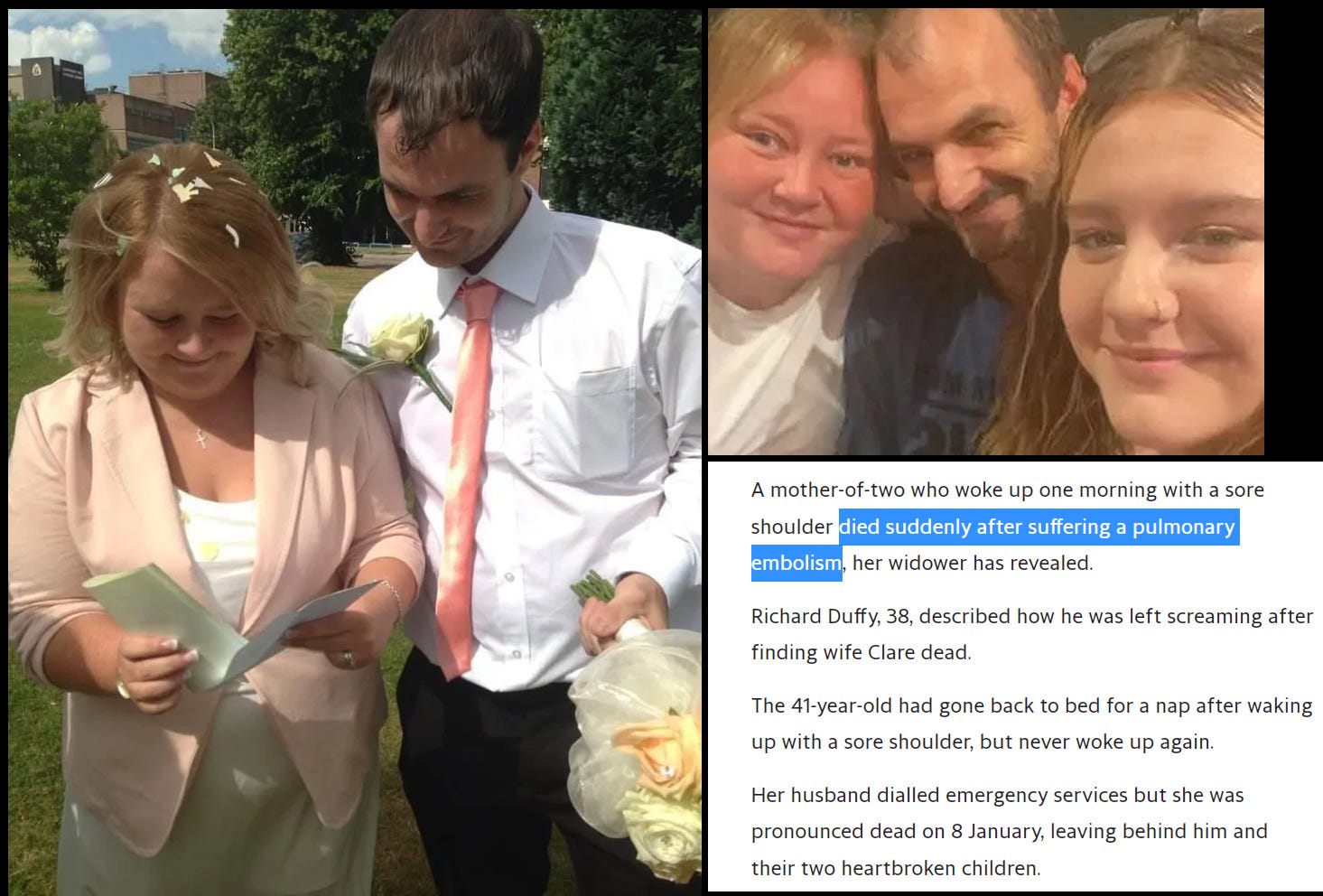
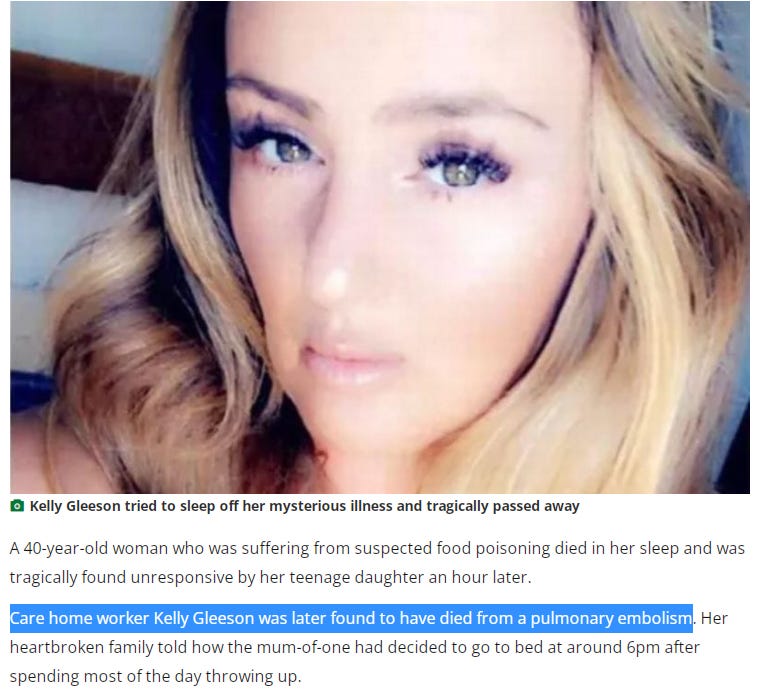
UK - 40 year old healthcare worker Kelly Gleeson died of a pulmonary embolism on Dec.29, 2022 (click here)
Little Rock, AR - 18 year old cheerleader Victoria Moody died suddenly of pulmonary embolism on Oct.23, 2022, after her dad took her to the hospital because she wasn’t feeling well on Sunday evening (click here)

Fareham, UK - 27 year old NHS nurse (who worked for Child and Adolescent Mental Health) Anna Harriman died suddenly in July 2022 of pulmonary embolism (click here)

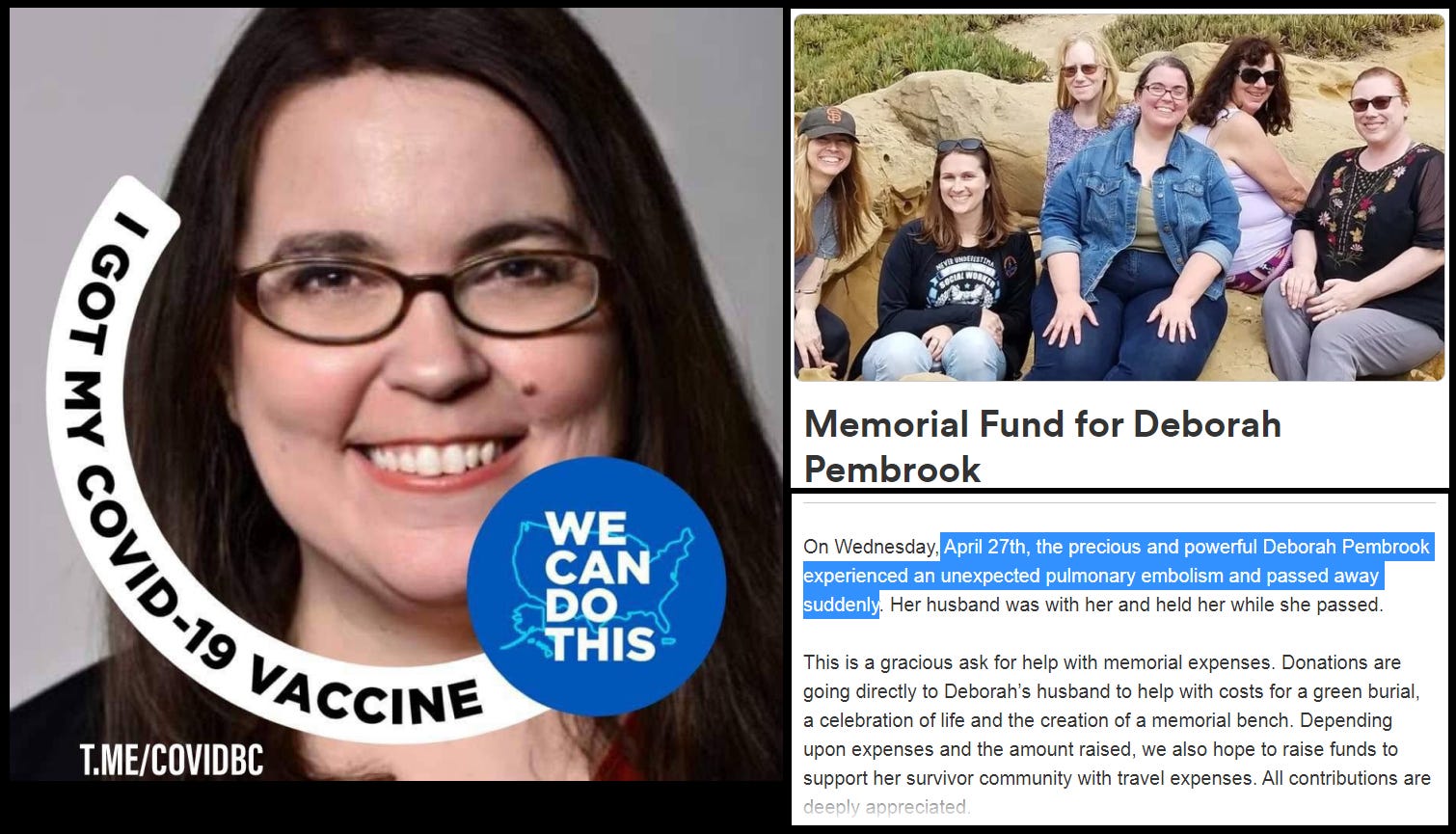
Monterey, CA - 51 year old Human Trafficking Outreach Manager Deborah Pembrook died suddenly on April 27, 2022 from a massive pulmonary embolus (click here)
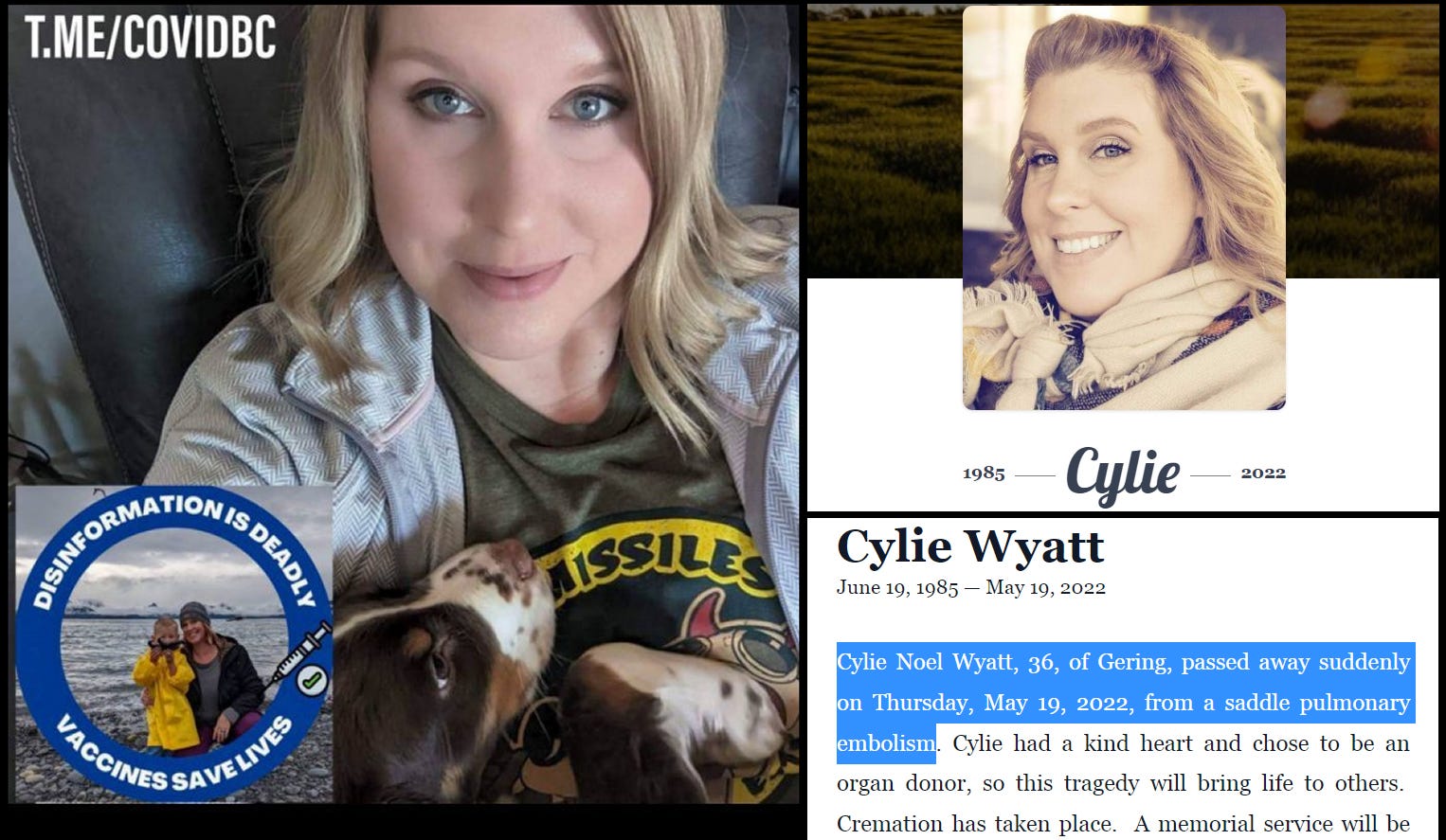
Gering, NE - 36 year old Cylie Noel Wyatt died suddenly from a saddle pulmonary embolism on May 19, 2022 (click here)
Houston, TX - Rice University director of student media, 46 year old Kelly Lash died suddenly on Feb.21, 2022 died of pulmonary embolism (click here)

Washington, DC - 28 year old law student at Howard University, Saron Berhe, died suddenly of pulmonary embolism on Jan.17, 2022 (click here)


A twenty three year old young special needs woman whom i have know most of her life died suddenly April 8 of pulmonary embolism. I went to the memorial service yesterday.
Why is nattokinase superior to other enzymes?