


Coronavirus, influenza virus, Vaccination and IGE Cytokine storm; a perfect storm of doing harm; Patients who have received influenza vaccine & coronavirus vaccine have IGE mediated reactions, at risk
upon exposure to the coronavirus antigen that drives the cytokine storm particularly in days 6-8 of the illness; Influenza vaccine increases coronavirus susceptibility by 36%; Irene Mavrakakis M. D.

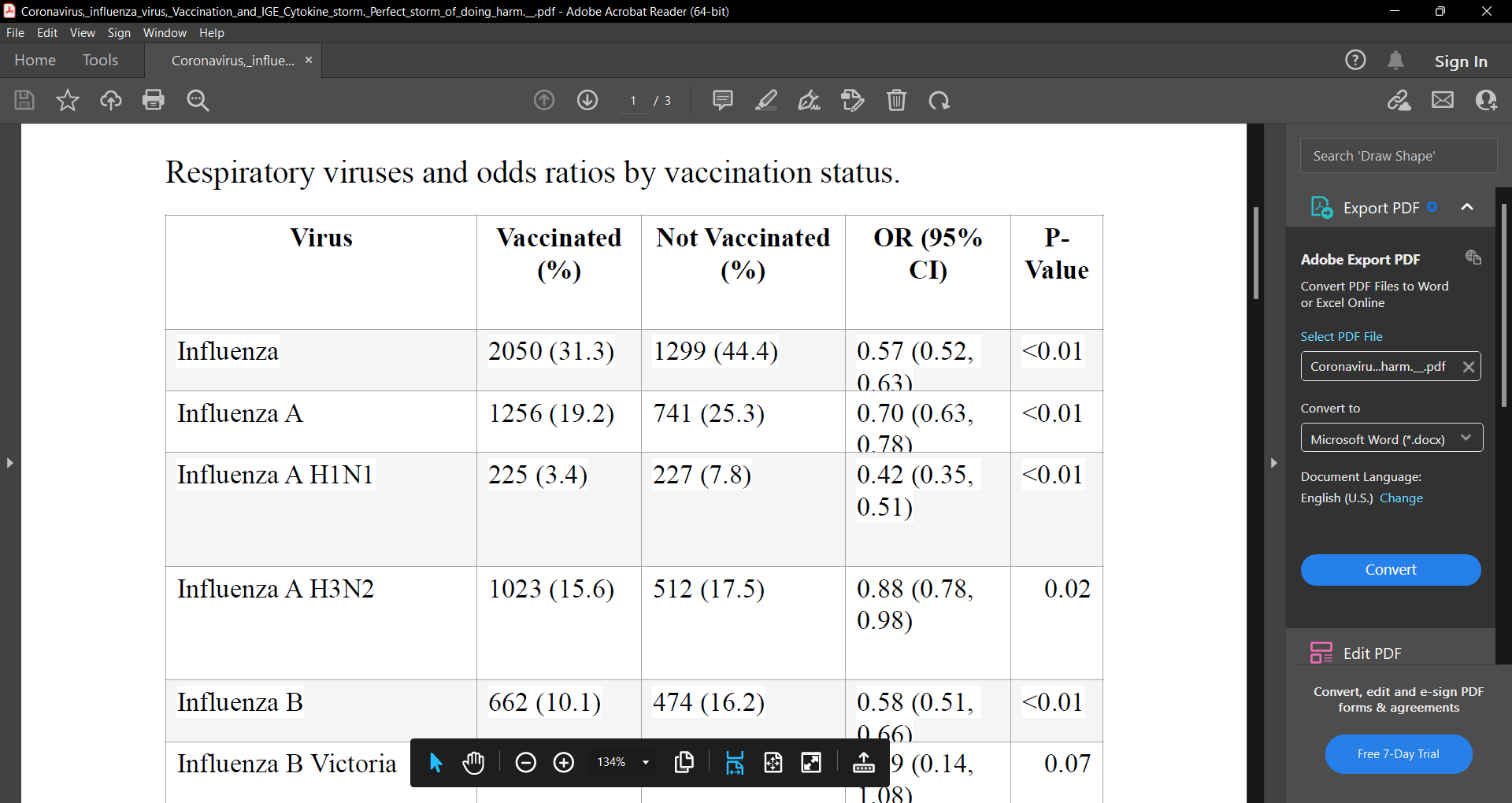
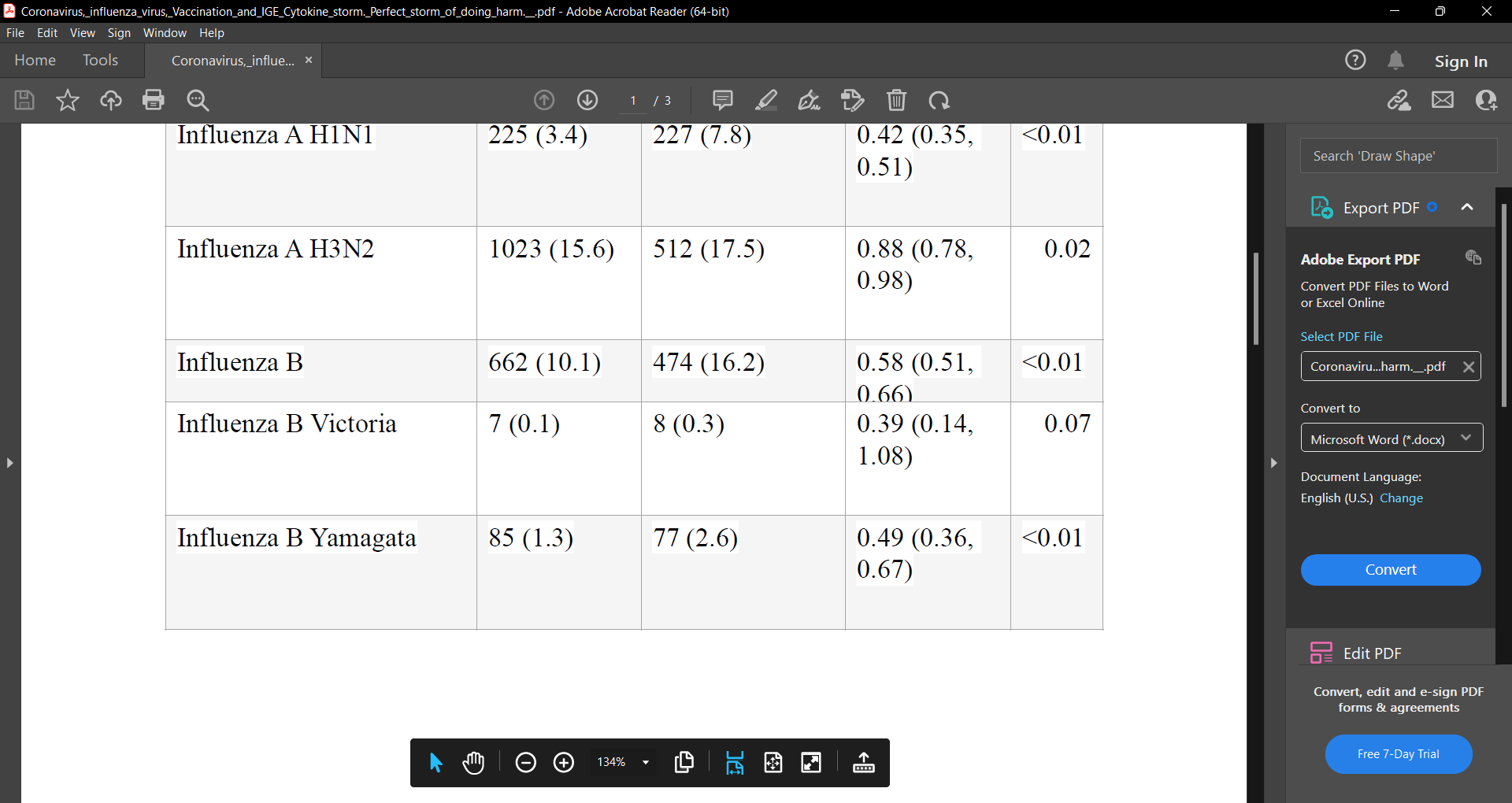
‘Influenza vaccine increases coronavirus susceptibility by 36% according to this study:https://pubmed.ncbi.nlm.nih.gov/31607599/. Influenza vaccination and respiratory virus interference among Department of Defense personnel during the 2017–2018 influenza season, table 5 clearly shows this fact.
Table 5 Respiratory viruses and odds ratios by vaccination status.
‘The increase in coronavirus susceptibility is either because there is
antigenic contamination of the influenza vaccine with the genetic
sequence of coronavirus or the PCR test can not distinguish between
them. Influenza vaccination has not decreased death from influenza since
the inception of the yearly influenza public policy programs. Influenza
vaccinated patients also have an IGE mediated cytokine storm upon
exposure to the influenza antigen. Coronavirus vaccine has been shown to
increase the cytokine storm when the recipient is exposed to the
coronavirus antigen. The mechanism is IGE based. This is the reason for
the improvement in symptoms with allergy treating medications during day
6-8 of symptomatic COVID patients. In this article the mechanism is
explained. Influenza vaccines and dengue-like disease https://
www.bmj.com/content/360/bmj.k1378/rr-15
"Last year's influenza vaccine also contained the same H3N2 strain as this
year's vaccine (A/Hong Kong/4801/2014 (H3N2)-like virus). Many people
would have developed long term IgE mediated sensitization to the H3N2
viral proteins due to last year's vaccine [1–4]. Those who received the
Flublok vaccine can be expected to have an even stronger IgE response
due to its 3X viral protein content [5,4]. This year's vaccine H3N2 proteins
would have been neutralized by these IgE antibodies. Thus resulting in the
observed low vaccine efficacy. [6] When a person making anti-H3N2 IgE is
infected with H3N2, one can expect the course of the flu to be significantly
worse. So the "cytokine storm" being observed in severe cases is likely to
be an infection concurrent with an allergic reaction. Death is caused by
anaphylactic shock but due to the presence of an infection, it is wrongly
classified as septic shock. In the case of food allergy for example, the
allergen exposure can be large enough to cause an immediate
hypersensitivity reaction and anaphylactic shock within minutes/hours. In
the case of influenza allergy, it may take a day or two for the virus to
replicate and produce enough viral exposure for anaphylaxis. So the
anaphylaxis unfolds over a couple of days. “Self-reported vaccination for
the current season was associated with a trend (P < 0.10) toward higher
viral shedding in fine-aerosol samples; vaccination with both the current
and previous year’s seasonal vaccines, however, was significantly
associated with greater fine-aerosol shedding in unadjusted and adjusted
models (P < 0.01). In adjusted models, we observed 6.3 (95% CI 1.9–21.5)
times more aerosol shedding among cases with vaccination in the current
and previous season compared with having no vaccination in those two
seasons.” [7] This result makes a lot of sense. When you have influenza
virus allergy and are infected, you have more mast cell degranulation,
more histamine, more mucus, more sneezing, more viral shedding.
Increased hospitalization rates have been observed in asthma patients that
have received the influenza vaccine. Again, this is as predicted because
asthma patients are likely to produce stronger IgE responses to the viral
proteins upon vaccination. [8] On subsequent virus exposure, they can be
expected to develop severe IgE mediated asthma. Consider dengue
infection. The initial mosquito bite that injects dengue virus into a person,
causes the induction of IgE against dengue proteins. [9] Upon a
subsequent bite that introduces the dengue virus again, the person
develops hives due to a dengue specific-IgE mediated allergic reaction. As
the infection (and thus allergic reaction) progresses and more histamine is
released, vascular permeability increases. The result is hypotension and
dengue shock syndrome. [10] Basically, a type 1 hypersensitivity reaction
caused upon dengue virus exposure following IgE mediated sensitization
to dengue viral proteins. The route of exposure for natural influenza
infection is the respiratory tract, not subcutaneous (SC) or intramuscular
(IM) injection. Influenza vaccines artificially changed the route of initial viral
protein exposure to SC or IM injection thus making it similar to the route of
exposure for dengue. The result is an IgE response to influenza proteins,
similar to the response for dengue. It should therefore not come as a
surprise that we are modifying the course of influenza infection such that it
is acquiring characteristics of a dengue infection (hives and shock). As a
result, allergy medications such as antihistamines and anaphylaxis
treatments may have to be considered to avoid or treat this man-made
influenza shock syndrome. "
To conclude, the injection of respiratory viral antigen or mrna that
produced respiratory viral antigen leads to primary sensitization via IGE.
Subsequent exposure to the antigen leads to an IGE mediated cytokine
storm. There is cross immunity between Coronavirus vaccine and influenza
vaccine with the coronavirus and influenza viral antigens. Treatment with
allergy medications has been implemented. One such protocol was
recently implemented by Dr. Chetty. An important additional medication for
this mechanism of illness is cromolyn sodium which is available in liquid
oral form and inhalation. It stabilizes mast cells and prevents the release of
histamine. This should be added to the armamentarium of medications
used.’
Irene Mavrakakis M. D.







The older population in The UK are in a rush to get their flu and bivalent covid booster. Many are sick afterwards. Some got both on the same day. Which injection made them ill? Who knows, who cares.
I do not know one older person who declined the latest covid booster. That is how brainwashed the elderly Brits have become. It is sad to watch the sheep go to slaughter. Most of them have had covid post earlier covid vaxxes. They simply don’t get it, but why would they, their GPs are totally SILENT for fear of losing their jobs.
I posted this study over two years ago on my social media because I was trying to explain to my friends and family that vaccines have unintended consequences and nonspecific effects that they usually are not tested for and so it’s a bad idea to take vaccines. I used this article as an example. Flu vaccines have been shown in other studies that they increase your risk of other respiratory diseases that the flu shot does not cover. There was also a study done at the beginning of the “pandemic” that showed that getting the flu shot was protective from dying of Covid but when they expand the study to more countries than one, they realized that the flu vaccine had actually been correlated with a higher mortality rate from Covid. Unfortunately, people are so brainwashed about vaccines that they refused to look at evidence that there could ever be anything wrong with them.