


Oster et al. JAMA doi: 10.1001/jama.2021.24110.; risk of MYOCARDITIS after receiving mRNA-based COVID-19 vaccines is increased across multiple age & sex strata & highest after second vaccination dose
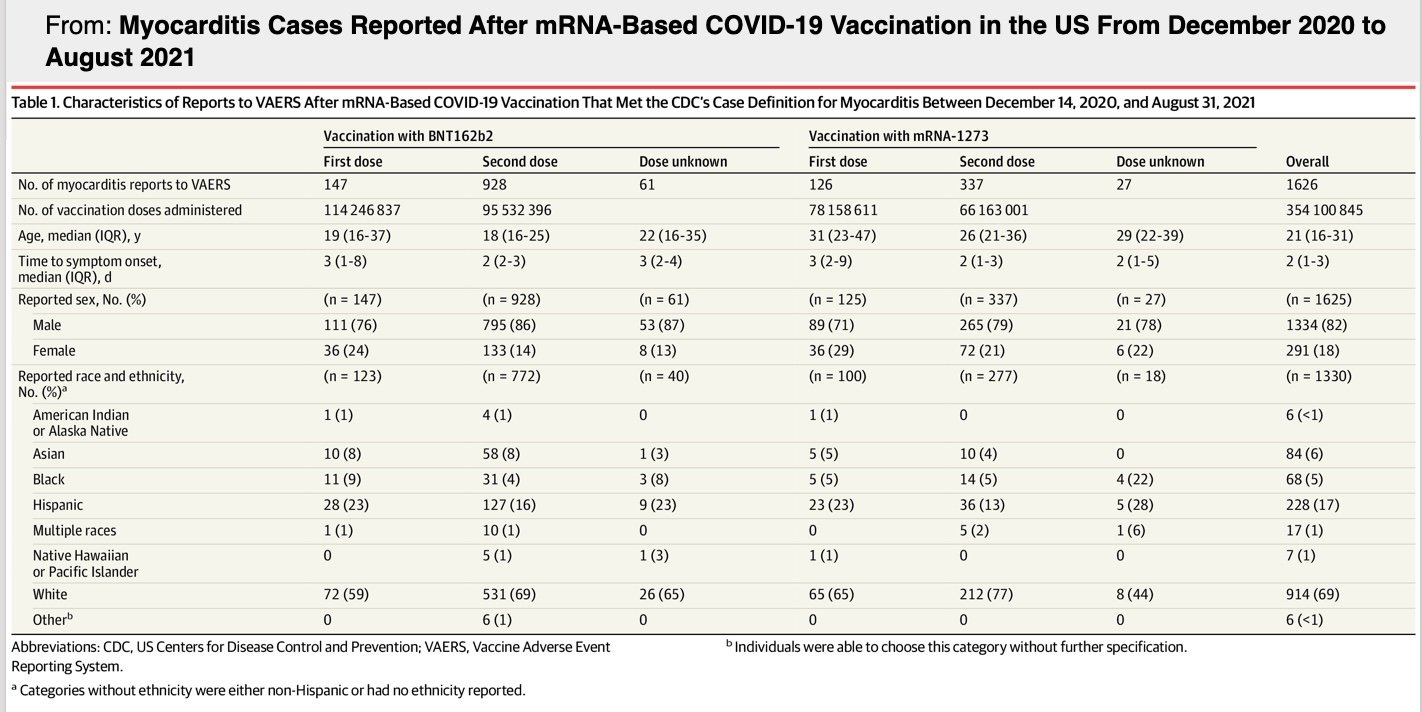
192,405,448 persons receiving a total of 354,100,845 mRNA-based COVID-19 vaccines during the study period, there were 1,991 reports of myocarditis to VAERS & 1,626 of these reports met case definition

I am not sure how this paper was published for it goes against the narrative but it is a welcomed piece of truth we have been arguing for near one year now.
JAMA. 2022 Jan 25;327(4):331-340. doi: 10.1001/jama.2021.24110.
Researchers looked at 192 million persons who received approx. 354 million mRNA-based COVID-19 vaccines across the study period (December 2020 and August 2021). They found 1,991 reports of myocarditis to VAERS and 1,626 of these reports met the case definition of myocarditis.
The primary outcome after the vaccination was the occurrence of myocarditis and the secondary outcome was pericarditis.
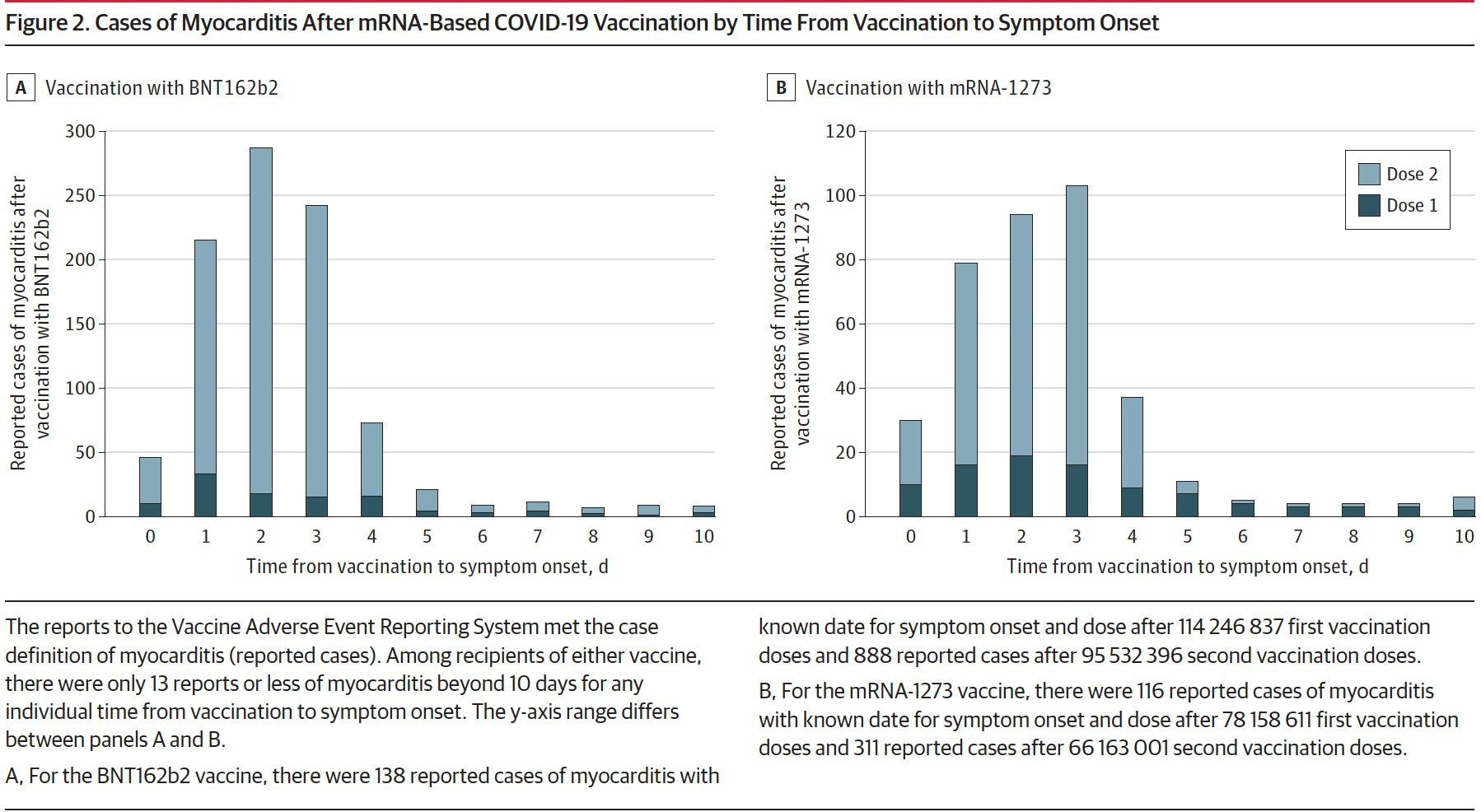
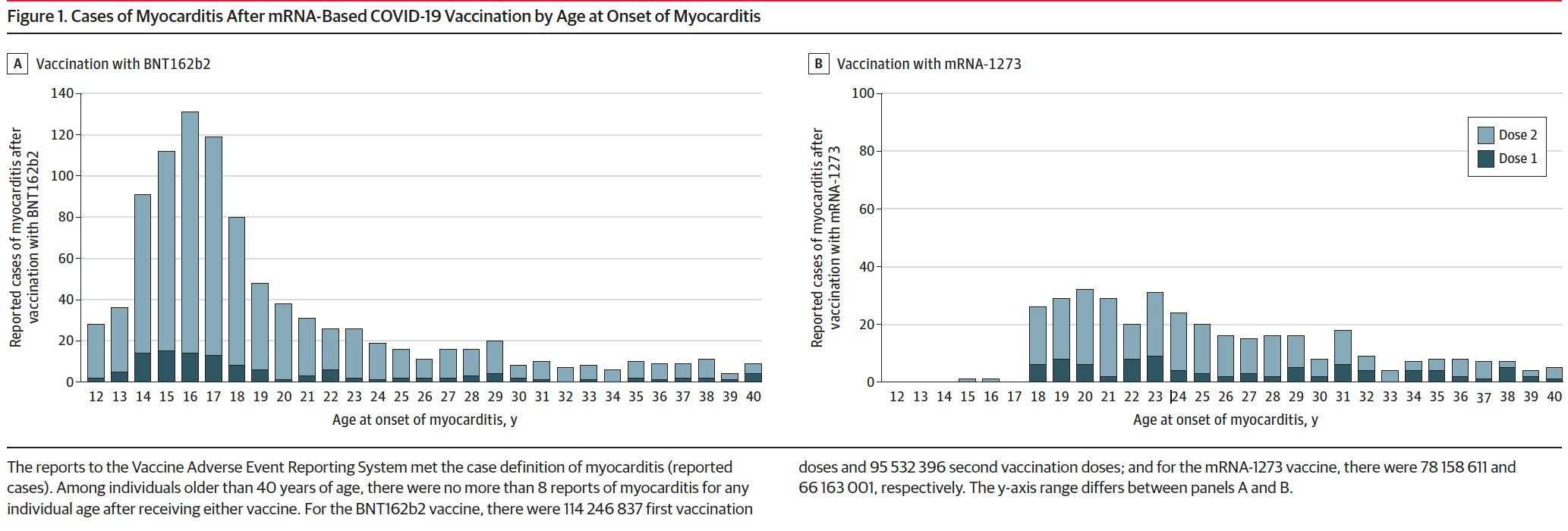
‘Of those with myocarditis, the median age was 21 years (IQR, 16-31 years) and the median time to symptom onset was 2 days (IQR, 1-3 days). Males comprised 82% of the myocarditis cases for whom sex was reported. The crude reporting rates for cases of myocarditis within 7 days after COVID-19 vaccination exceeded the expected rates of myocarditis across multiple age and sex strata. The rates of myocarditis were highest after the second vaccination dose in adolescent males aged 12 to 15 years (70.7 per million doses of the BNT162b2 vaccine), in adolescent males aged 16 to 17 years (105.9 per million doses of the BNT162b2 vaccine), and in young men aged 18 to 24 years (52.4 and 56.3 per million doses of the BNT162b2 vaccine and the mRNA-1273 vaccine, respectively)…
There were 826 cases of myocarditis among those younger than 30 years of age who had detailed clinical information available; of these cases, 792 of 809 (98%) had elevated troponin levels, 569 of 794 (72%) had abnormal electrocardiogram results, and 223 of 312 (72%) had abnormal cardiac magnetic resonance imaging results. Approximately 96% of persons (784/813) were hospitalized and 87% (577/661) of these had resolution of presenting symptoms by hospital discharge. The most common treatment was nonsteroidal anti-inflammatory drugs (589/676; 87%).’
Oster et al. concluded that the ‘risk of myocarditis (and pericarditis) after receiving mRNA-based COVID-19 vaccines was increased across multiple age and sex strata and was highest after the second vaccination dose in adolescent males and young men. This risk should be considered in the context of the benefits of COVID-19 vaccination.’
Limitations to consider in this report:
1.VAERS is a passive reporting system but it works well as a sentinel system; reporting though may be highly incomplete
2. VAERS only captures about 1 to 10% of burden (deaths, adverse effects etc.)
3. subjective reporting; under-reporting as well as over-reporting (former more likely); rates may be even higher
These results mirror
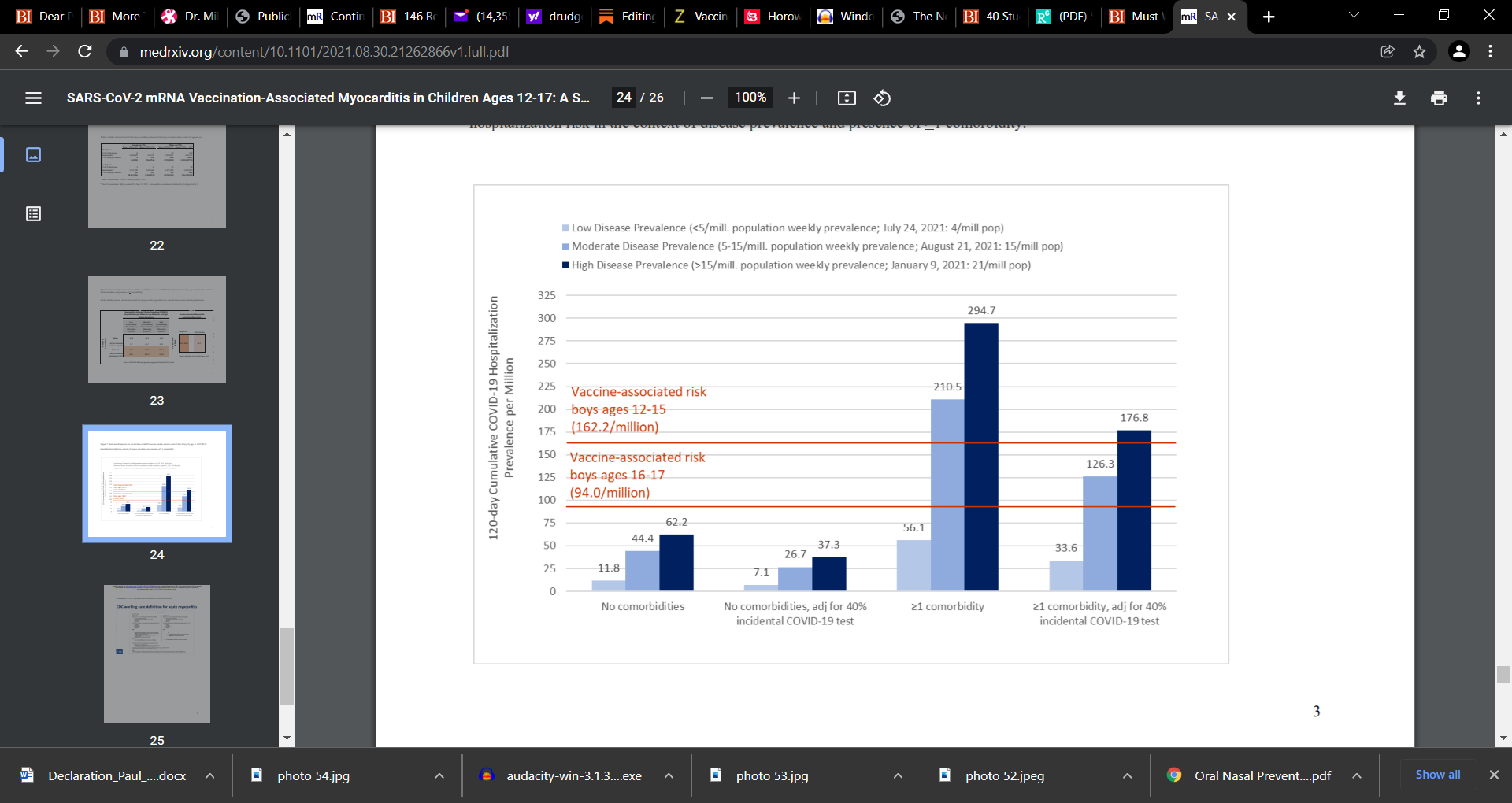
1.) those by Hoeg: MYOCARDITIS: SARS-CoV-2 mRNA Vaccination-Associated Myocarditis Children Ages 12-17: A Stratified National Database Analysis; https://www.medrxiv.org/content/10.1101/2021.08.30.21262866v1 Hoeg et al.
and
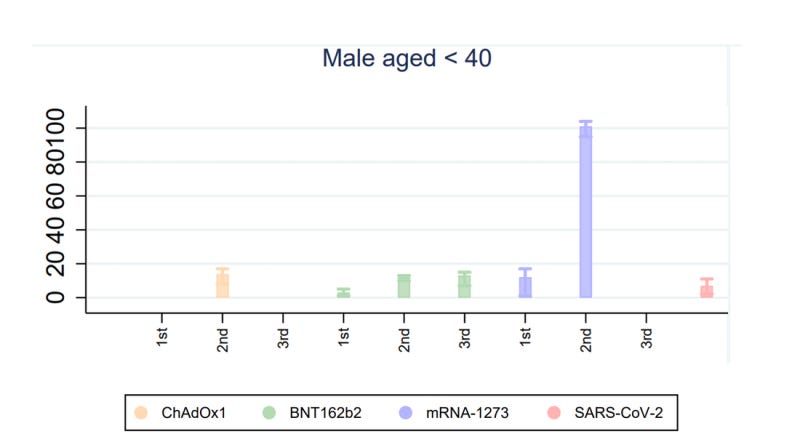
2) these results matches the Patone et al. paper showing that the risk of myocarditis is especially heavy in those < 40 (mainly males) for both the Pfizer and Moderna vaccine (highest after the 2nd shot and booster). https://www.medrxiv.org/content/10.1101/2021.12.23.21268276v1.full.pdf
When Patone et al. updated the research, they pulled the data apart by age and gender (https://www.medrxiv.org/content/10.1101/2021.12.23.21268276v1.full.pdf) which firmly shows that males < 40 (Moderna) are at far greater risk for myocarditis than infection….and for doses 1 and 2. This data also showed that Pfizer doses 2 and 3 result in greater myocarditis than COVD infection(red bar). Some argue that if the younger ages e.g. 16 to 25 or so is pulled out, that the vaccine myocarditis risk is even more markedly elevated.


I am glad I heard your voice on the 2nd Opinion conference. Now I hear a Caribbean accent in my head every article of yours I read. Which makes it even better. Thanks for your work! Bless up!
Thank you for sharing these studies. I will share with our pediatrician who denies any such notion is valid. Needless to say we have left the practice and I was vocal on telling them they have now been compromised with regard to advocating on behalf of the health if children and young adults in the practice. I don't know how they look at themselves in the mirror every day. Shameless.