


Robert Malone & Albert Bourla & Bancel & Weissman et al. are laughing at all of us! How stupid we are: "Arcturus Therapeutics Receives Clearance from FDA to Begin H5N1 Pandemic Flu mRNA Vaccine
Clinical Trial"; a “Study Can Proceed” notification for the Company’s Investigational New Drug (IND) application, ARCT-2304, a self-amplifying mRNA (sa-mRNA) vaccine candidate for active immunization

Malone must be laughing today saying ‘what a bunch of stupid idiotic fools, morons we all are, that he could dupe us so easily to take our donated money, as one of the inventors of this deadly mRNA technology mRNA vaccine and shill sell it, push us to take vaccine, coerce, stay silent on mRNA reverse transcription and harms of LNP platform, and specifics until he had to speak out as deaths grew, many died of course due to Malone et al. and his stance and coercion, then say para ‘oh, its harmful but still take it’ and para ‘oh, I know of strong data showing it saves lives’, that today the FDA is giving clearance for self-amplifying NOT NEEDED mRNA vaccines to go ahead.
Imagine, a mRNA Malone Bourla et al. vaccine for a fake PCR manufactured non-avian bird flu pandemic, a pandemic that never will be, that ‘is not’, and you have to understand, the move is to make mRNA gene vaccines part of your daily life, to govern all about you, to re-engineer your DNA and alter humanity forever. There is no safe mRNA technology or vaccine, and it is NOT needed.
These people at Pfizer, Moderna, BioNTech et al, these inventors like Malone and Sahin and Kariko et al. have taken humanity now to the brink for they are into making money and fame, while your lives are in the breach for this. Money, power, control, depopulation etc. A deadly, ineffective, not needed, cancer causing, catastrophic cardiovascular illness mRNA vaccine. For what?
Be warned, they are moving to transform your life with mRNA technology.
Malone, Bourla, Bancel, Sahin, Weissman et al. must be taken into proper legal settings and under oath to explain what they did, what they knew, when, and all questions that up to today have not been answered. Under oath, separately and not in any bullshit dog and pony senate or house hearing. I mean real independent tribunals, real legal procedures with judges, juries, courts, to get answers. The FDA also has to go under oath legally, as to how they could have granted EUA for a vaccine that based on the data submitted was ineffective and deadly and now societally we live to tell how dangerous it is and was. This mRNA vaccine must be stopped by POTUS Trump now and first hour after being sworn in. Robert Kennedy Jr. must stand up now, urgently and speak it out, call for the stop of all mRNA gene-based vaccines.
These evil beasts like Malone, Bourla, Bancel et al. must go away for 100 years with proper research, get us proper data, 100 years, with full ethical debate, and then come again and ask us about this. Today it is ineffective, very unsafe, and NOT needed. We had no pandemic, it was all a fraud, a PCR manufactured fraud fake non-pandemic based on lie of asymptomatic transmission (we have found not one case of asymptomatic spread across 5 years of this fraud). All to hurt POTUS Trump in 2020 election and to bring this deadly mRNA shot.
There is no H5N1 (H5N2, H5N8 etc.) avian bird flu pandemic (and no virus going from fowl to cattle to humans, no indication of any pandemic or mass event, no human-to-human transmission) and what they are doing is creating a fraud fake crisis event (calling it pandemic) with a fraud PCR (DNA amplification) process AGAIN as they did for COVID and did for H1N1 fraud non swine flu in 2009 etc. This is all fraud, using PCR to manufacture and create fake pandemic. We never had a pandemic. All a lie, Trump was lied to 100%. He trusted.
Now a self-replicating mRNA vaccine (with more copies of mRNA (self-replicating) and thus enhanced expression of haemagglutinin (HA) and neuraminidase (NA) antigens/bird flu spike protein) for a fraud bird flu non-pandemic that could make more copies of mRNA and thus more spike protein in you for this bird flu virus.
At the same time, these evil CDC, NIH, Fauci types, Francis Collins types, FDA, vaccine makers, Bourlas, Bancels, Malones etc. deepstate beasts could be creating more infectious and lethal variants of this benign bird flu (if it is real) in the lab, making it more infectious (serial passaging) and adding more lethal variants to it (recombination, re-assortment, drift, shift, so called ‘gain-of-function’ or rather a claim of fiction or gain of fiction or claim of function???)…they could be creating man-made more infectious lethal versions to bring to us, so that they can then have a reason to use their deadly mRNA vaccine on us….and we will fall for it. Do you understand they are creating the problem and then offering us the solution that is also deadly? Cloward-Piven?
Ask Malone what he meant below…where is the unambiguous data? Where is the data or evidence that his mRNA gene vaccine saved lives? Why did he promote this vaccine for children when there was zero risk to them, to healthy children and we have not had one case across 5 years in USA in children 0 to 19 years old who got severely ill or died from this fraud COVID. let’s ask him in proper legal trials with Bourla and Bancel and Weissman et al. We need answers. I suggest Malone debate Nicolas Hulscher or Peter McCullough who have shown (see stack below) that Post-COVID-19 Myocarditis is Not More Severe Than COVID-19 Vaccine-Induced Myocarditis…

McCullough:
‘We identified major methodological flaws in their study that led to significantly biased conclusions. Thus, we (Nicolas Hulscher, MPH, Jessica Rose, PhD, and Peter McCullough, MD, MPH) submitted a Letter to the Editor to JAMA to highlight these concerns. Unfortunately, they declined to publish our research letter “because of the many submissions we receive and our space limitations in the Letters section.” We were fortunately able to publish our concerns in the non-partisan journal Science, Public Health Policy, and the Law: Letter to the Editor: Long-Term Prognosis of Patients with Myocarditis Attributed to COVID-19 mRNA Vaccination, SARS-CoV-2 Infection, or Conventional Etiologies:
‘Semenzato et al. incorrectly concluded that patients who develop myocarditis following an mRNA COVID-19 vaccination experience fewer cardiovascular complications at 18 months compared to those with alleged myocarditis following a COVID-19 infection or an unusually large series of those with “conventional” myocarditis allegedly not related to the infection or the vaccine [1]. The study methodology raises numerous concerns. According to Table 2, among the post-COVID-19 myocarditis and ‘conventional’ myocarditis groups, 46.3% and 52.3% received at least one COVID-19 vaccine, respectively. Since Semenzato et al. did not incorporate a proper clinical adjudication protocol for myocarditis, it is likely that a substantial number of patients in the post-COVID-19 and ‘conventional’ groups actually had cardiovascular conditions and laboratory results that triggered automated codes mapping to myocarditis. For example, elevated troponin values commonly found with hospitalized illness do not alone indicate myocarditis. Moreover, vaccine-induced myocarditis was defined as patients diagnosed with myocarditis within 7 days of inoculation, while post-COVID-19 myocarditis was given a 30-day window since the initial infection. The authors cite Le Vu et al. as justification for this methodological choice [2], where 331 hospitalized cases experienced myocarditis or pericarditis from 8 to 21 days following vaccination and were not classified as “post-vaccination cases” because they didn’t occur within 7 days. The 7-day vaccine myocarditis window is obviously biased and may be approximately four times more likely to ascribe myocarditis to the infection as opposed to the vaccine. After COVID-19 vaccination, the mRNA has been found in blood 28 days after injection [3] and the vaccine-derived prefusion stabilized Spike protein is circulatory in blood for at least six months [4], suggesting there is a very large window after vaccination where myocarditis is a plausible vaccine injury syndrome.
To investigate the percentage of vaccine-induced myocarditis that occurs after the 7-day window, the Vaccine Adverse Event Reporting System (VAERS) data was queried using the SYMPTOM and NUMDAYS variables [5]. For this study, we used both the VAERS Domestic and Foreign data sets. A single SYMPTOM variable was constructed by concatenating individual SYMPTOM [1-n] variables. NUMDAYS is the number of days between the onset date and the vaccination date. A query for ‘myocarditis’ and ‘myopericarditis’ was conducted using the SYMPTOM variable yielding N_myo_tot = 18,494 reports, whereby N_myo_tot_ND_valid = 14,224 had valid data with respect to the NUMDAYS variable. Only records with valid NUMDAYS data were included in subsequent calculations; entries with “NA” were excluded. The number of reports that occurred more than 7 days post injection was N_myo_tot_ND_valid_7 days = 4,602. The percentage of reports occurring 7 days post injection was calculated as follows: N_myo_tot_ND_valid_7 days/N_myo_tot_ND_valid×100. 32.4% of myocarditis/myopericarditis cases were reported more than 7 days after the last vaccination, meaning that 67.6% of reports qualify as “vaccine-induced myocarditis” according to the definition provided by Semenzato et al. [1]. Notably, among these reported post-injection myocarditis cases more than 7 days after injection, 67.5% were listed as “not recovered” at the time of the report, of which the mean age was 35. These data indicate that Semenzato et al’s choice of post-vaccine myocarditis limited to 7 days after injection was biased and worked to falsely reduce cases of myocarditis attributed to vaccination. The authors do partially acknowledge this limitation in eTable4, where they redefine cases of post-vaccine myocarditis as having received an mRNA vaccine within the previous 30 days instead of 7 days. This more balanced analysis resulted in a higher weighted hazard ratio (wHR) for the composite outcome in post-vaccine myocarditis cases (wHR = 0.84) compared to the original analysis (wHR = 0.55), which would significantly alter Semenzato et al.’s conclusions.
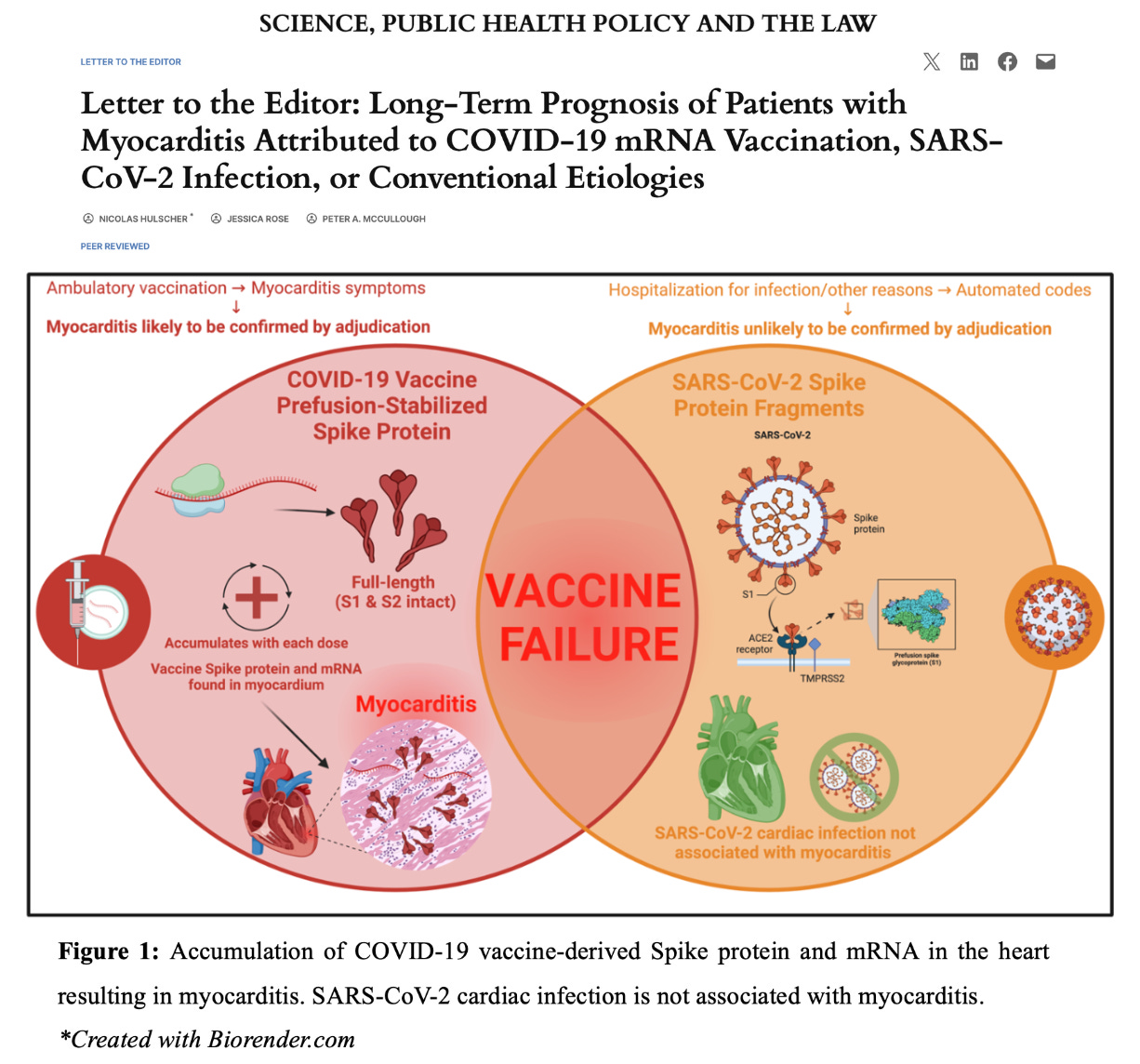
The conclusions made by Semenzato et al. are not consistent with the literature. Watanabe and Hama found that the myocarditis mortality rate ratio (MMRR) was significantly higher in the COVID-19 vaccinated population compared to the general population during the three years preceding the COVID-19 pandemic, with a pronounced increase among young adults (MMRR: 7.80 for individuals in their 30s) [6]. The OpenSAFELY study found that myocarditis occurred only among COVID-19 vaccinated children and not SARS-CoV-2 infected children, with a sample size of over 1 million participants [7]. Both mRNA and vaccine-derived Spike protein with inflammation have been found in the human heart in those who died after COVID-19 vaccination and in those with vaccine-induced myocarditis, respectively (Figure 1) [8, 9]. Whereas autopsies of individuals who died from SARS-CoV-2 infection indicate that cardiac infection with the virus is not associated with myocarditis [10].
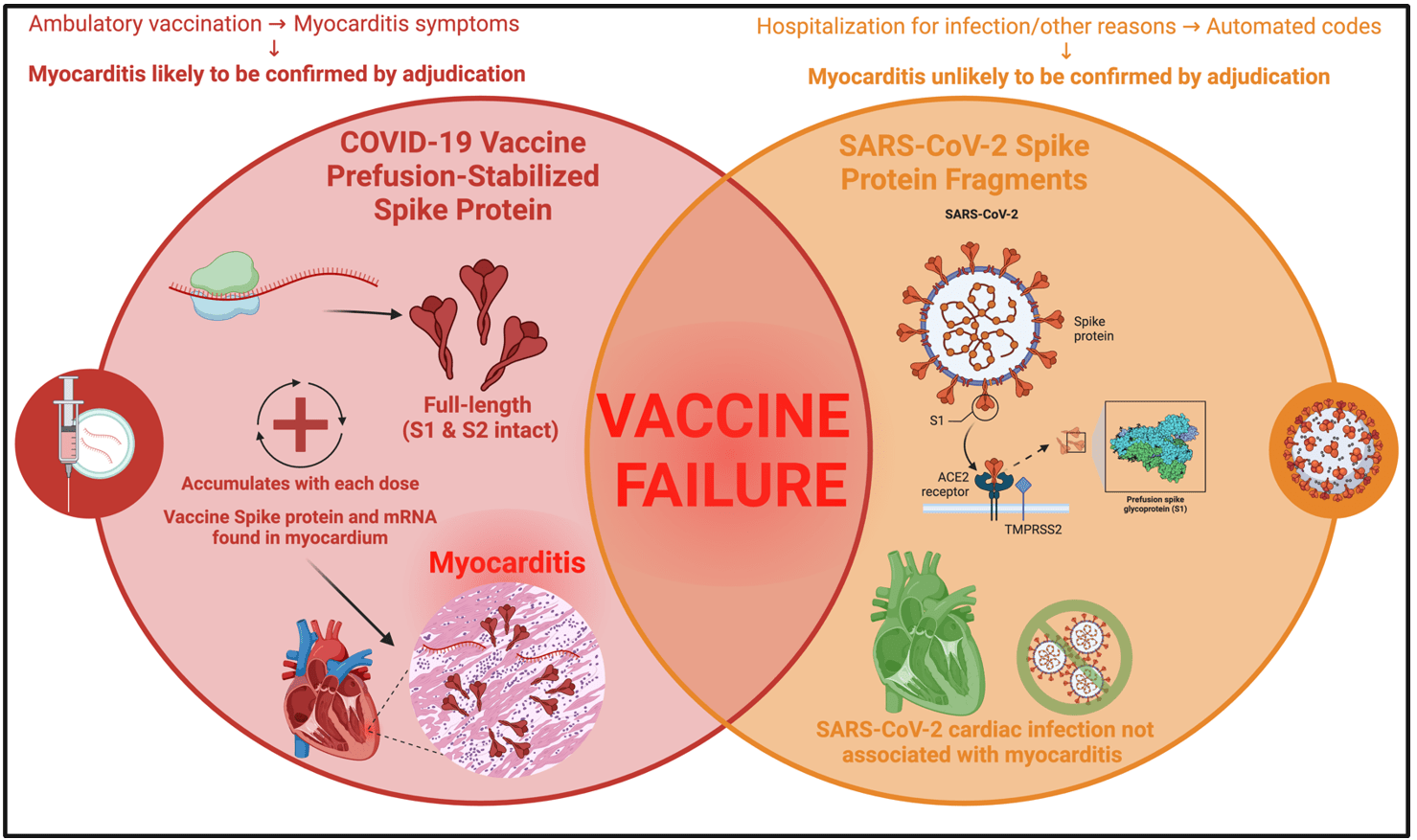
Figure 1.
Accumulation ofCOVID-19 vaccine-derived Spike protein and mRNA in the heart resulting in myocarditis. SARS-CoV-2 cardiac infection is not associated with myocarditis. *Created with Biorender.com
In conclusion, the study by Semenzato et al. is misleading. SARS-CoV-2 infection does not cause serious myocarditis [7, 10], whereas COVID-19 vaccination is well recognized to cause symptomatic and fatal myocarditis [6, 11]. Future prospective cohort studies should classify patients correctly, have extended and equal windows of observation, and clinical adjudication with exam, ECG, blood biomarkers, and cardiac imaging. The use of automated data sources alone should not be relied upon for comparative studies because it is subject to investigator bias and is greatly misleading.
References
1
Semenzato L, Le Vu S, Botton J, et al. Long-Term Prognosis of Patients With Myocarditis Attributed to COVID-19 mRNA Vaccination, SARS-CoV-2 Infection, or Conventional Etiologies. JAMA. Published online August 26, 2024. doi:10.1001/jama.2024.16380 https://doi.org/10.1001/jama.2024.16380
2
Le Vu S, Bertrand M, Jabagi MJ, et al. Age and sex-specific risks of myocarditis and pericarditis following Covid-19 messenger RNA vaccines. Nat Commun. 2022;13(1):3633. Published 2022 Jun 25. doi:10.1038/s41467-022-31401-5 https://doi.org/10.1038/s41467-022-31401-5
3
Castruita JAS, Schneider UV, Mollerup S, et al. SARS-CoV-2 spike mRNA vaccine sequences circulate in blood up to 28 days after COVID-19 vaccination. APMIS. 2023;131(3):128-132. doi:10.1111/apm.13294 https://doi.org/10.1111/apm.13294
4
Brogna C, Cristoni S, Marino G, et al. Detection of recombinant Spike protein in the blood of individuals vaccinated against SARS-CoV-2: Possible molecular mechanisms. Proteomics Clin Appl. 2023;17(6):e2300048. doi:10.1002/prca.202300048 https://doi.org/10.1002/prca.20230004
5
U.S. Department of Health and Human Services. Vaccine adverse event reporting system (VAERS) [Internet],
https://vaers.hhs.gov
(2024, Accessed 27 August 2024).
6
Watanabe S, Hama R. SARS-CoV-2 vaccine and increased myocarditis mortality risk: A population based comparative study in Japan. medRxiv. 2022. DOI: 10.1101/2022.10.13.22281036. https://doi.org/10.1101/2022.10.13.22281036
7
Andrews CD, Parker EPK, Horne E, Walker V, Palmer T, Schaffer AL, et al. OpenSAFELY: Effectiveness of COVID-19 vaccination in children and adolescents. medRxiv. 2024; DOI: 10.1101/2024.05.20.24306810 https://doi.org/10.1101/2024.05.20.24306810
8
Krauson AJ, Casimero FVC, Siddiquee Z, Stone JR. Duration of SARS-CoV-2 mRNA vaccine persistence and factors associated with cardiac involvement in recently vaccinated patients. NPJ Vaccines. 2023;8(1):141. Published 2023 Sep 27. doi:10.1038/s41541-023-00742-7 https://doi.org/10.1038/s41541-023-00742-7
9
Baumeier C, Aleshcheva G, Harms D, et al. Intramyocardial Inflammation after COVID-19 Vaccination: An Endomyocardial Biopsy-Proven Case Series. Int J Mol Sci. 2022;23(13):6940. Published 2022 Jun 22. doi:10.3390/ijms23136940 https://doi.org/10.3390/ijms23136940
10
Lindner D, Fitzek A, Bräuninger H, et al. Association of Cardiac Infection With SARS-CoV-2 in Confirmed COVID-19 Autopsy Cases. JAMA Cardiol. 2020;5(11):1281-1285. doi:10.1001/jamacardio.2020.3551 https://doi.org/10.1001/jamacardio.2020.3551
11
Hulscher N, Hodkinson R, Makis W, McCullough PA. Autopsy findings in cases of fatal COVID-19 vaccine-induced myocarditis. ESC Heart Fail. Published online January 14, 2024. doi:10.1002/ehf2.14680 https://doi.org/10.1002/ehf2.14680’
___
You must not wait for another catastrophic crisis (at times manufactured but we are prevented from making our own basic personal decisions or accessing needed drugs and response tools) to catch you off-guard. We must take charge and be prepared today so that we can enjoy peace of mind tomorrow.
Enter the Wellness Company as a solution and a willing participant in the health care conversation. From telemedicine, prescriptions, memberships, and supplements, TWC is leading America with alternative choices to the traditional health care model.
If you wish to give a donation to help me, you can at:
Zelle:
sr7283@gmail.com
Or Ko-Fi
Ko-fi.com/drpauleliasalexander
Or to my address at:
150 South 8th Street
Unit 170
Lewiston, New York
14092
Alternatively, please consider going from an UNPAID subscriber or follower to a PAID at $5 per month or $30 per year. This can provide me help. If this is not possible at this time, this is ok, please remain a subscriber for FREE and there is no difference between FREE and PAID. No restrictions.
Please consider support of a good PATRIOT company (in this PATRIOT economy) Drs. McCullough, Risch, Thorp, myself support (they are our sponsors), The Wellness Company; see the emergency preparation kit (key component being antibiotics you were denied by doctors, pharmacists, governments during the fraud COVID), first aid kit, travel emergency kit, contagion control kit etc. Please consider the SPIKE SUPPORT (spike protein DETOX dissolving spike from mRNA vaccine, this is critical to remove spike form the mRNA vaccine/and DNA viral vector) formula with NATTOKINASE as well as the triple formula (SPIKE SUPPORT, BROMELAIN, CIRCUMIN)






From the start, early in 2020, I repeatedly said that we were witnessing the largest crime in human history *AND* that if they were allowed to get away with this crime, they would double-down to finish the job.
Well, the criminal perpetrators were NOT taken out and now, here they are, about to enter Phase 2 and finish the job. From the lessons they learned the 1st time around with Covid, this time they'll be more efficient and ruthless - they won't make the mistakes that they did in Phase 1.
Did people expect that they would repent and reform? Seriously? STUPID people!! Psychopath monsters NEVER repent nor reform. Next time they're coming at us with all cylinders firing.
I'll say it for the 847th time: "If we don't take THEM out, they will take US out - guaranteed!!
time to castrate the FDA