SAGE HANA'S incredible scholarship on Glioblastomas (braon cancers) is stunning & frightening! SAGE is talking about a global pandemic of GLIOBLASTOMAS due to the COVID mRNA technology vaccine
Pandemic of brain cancers are rapid, deadly! Herd culling mRNA technology is packaged in lipid nanoparticles able to cross the blood brain barrier; Oncologists & Glioblastoma specialists are silent??


‘Paging all Oncologists and Glioblastoma Specialists.
Are you seeing an uptick of cases?
Glioblastomas can be difficult to treat for the following reasons:
They are fast-growing and invade nearby brain tissue, making 100% removal nearly impossible.
The blood-brain barrier prevents certain treatments from being able to reach the tumor and be effective.
They have many different types of tumor cells (heterogeneous) and can change over time, which makes them difficult to treat.
Because of this, the treatment plan for glioblastoma may combine several approaches, including surgery, radiation therapy, chemotherapy, clinical trials, Tumor Treating Fields (TTFields), and targeted therapies.
Surgery is often the first step in treating glioblastoma. Surgery allows the medical team to get a biopsy and make a diagnosis, relieve pressure on the brain, and safely remove as much tumor as possible. Glioblastomas are diffuse and have finger-like tentacles that infiltrate the brain, which makes them very difficult to remove completely. This is particularly true when the tumors are growing near important regions of the brain that control functions such as language and movement/coordination.
From my board, a comment from Kanada unrelated to the below anecdata from Sarah regarding a Love Canal cluster of events and deaths in Atlanta, home of the lovely CDC.
Speaking of turbo cancer: spent the weekend taking care of my cousin (64, previously in excellent health) who had the injectables two years ago and then the boosters and is now in a near vegetative state, due to turbo glioblastoma. I sat with him this weekend so his wife could go do things like grocery shopping. The decline in this formerly brilliant lawyer/outdoorsman is shocking. And I KNOW it was the injectables.
E’s brother died of a heart attack. Her friend of a glioblastoma.
Two clients in the studio have been recently diagnosed with cancer, and currently in treatment. One has a sister who was diagnosed with endometrial cancer at the same time. Cancer does not run in their family.
H has a CT to look at a cyst on her kidney.
One client with fibroids bleeding out.
Just got another glioblastoma call...😔 D's aunt...That's #6 for glioblastoma in my immediate circle.
G's customer just diagnosed with glioblastoma - 6wks ago...discharged from hospital, sent home to wait to die. Now deceased.
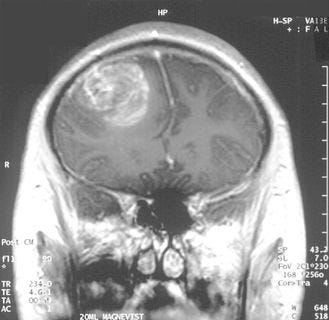
Glioblastoma (GBM) is a malignant grade 4 tumor that is predominantly made up of abnormal astrocytic cells, but also contains a mix of different cell types (including blood vessels) and areas of dead cells (necrosis). It is the most common primary brain cancer, with around 12,000 cases diagnosed in the United States each year.1 GBM is a fast-growing and aggressive brain tumor that invades nearby regions of the brain but generally does not spread to distant organs.0 Initial signs and symptoms of glioblastoma are nonspecific and may include headaches, personality changes, nausea, and symptoms similar to those of a stroke. Symptoms often worsen rapidly and may progress to unconsciousness.2
Glioblastoma (GBM)
Glioblastomas (also called GBM) are malignant (cancerous) grade 4 tumors. The tumor is predominantly made up of abnormal astrocytic cells, but also contains a mix of different cell types (including blood vessels) and areas of dead cells (necrosis). Glioblastomas are diffusely infiltrative and invade nearby regions of the brain. They can also sometimes spread to the opposite side of the brain through connection fibers (corpus callosum) or the ventricular system. It is exceedingly rare for glioblastomas to spread outside of the brain and spinal cord.
Glioblastomas commonly arise de novo, meaning they begin as a grade 4 tumor with no evidence of a lower-grade precursor. De novo tumors are the most common form of glioblastoma. They tend to be more aggressive and are more common in patients 60 years of age or older, though younger patients may also be affected. Alternatively, secondary glioblastomas may progress from a lower-grade astrocytic tumors (grade 2 or 3) and evolve into grade 4 tumors over time. In general, these tumors tend to be slower growing initially, but can progressively become aggressive.
In 2021 the World Health Organization (WHO) updated CNS tumor classifications, incorporating new knowledge gained from additional molecular markers and new diagnostic techniques. What used to be classified as Glioblastoma, IDH mutant is now classified as Astrocytoma, IDH mutant, grade 4. For information on Astrocytoma, IDH mutant, grade 4, please see our web page on Astrocytoma (Adult type). Glioblastomas are now classified as Astrocytoma IDH-wildtype tumors with at least one of the following: microvascular proliferation, necrosis, EGFR amplification, TERT promoter mutation, or combined gain of chromosome 7/loss of chromosome 10 copy number changes.
Location
Glioblastoma is most commonly found in the frontal lobe, followed by the temporal, parietal, and occipital lobes.
Symptoms
Patients with glioblastomas develop symptoms rapidly due to mass effect from the tumor itself or from the fluid surrounding the tumor that causes further brain swelling (edema). Common presenting symptoms at diagnosis include:
Seizures
Severe headaches
Memory and language problems
Changes in personality and behavior
Muscle weakness or paralysis
Fatigue
Issues with coordination
Speech, hearing, and vision problems
Other symptoms may occur depending on the size and location of the tumor.
Treatment
Glioblastomas can be difficult to treat for the following reasons:
They are fast-growing and invade nearby brain tissue, making 100% removal nearly impossible.
The blood-brain barrier prevents certain treatments from being able to reach the tumor and be effective.
They have many different types of tumor cells (heterogeneous) and can change over time, which makes them difficult to treat.
Because of this, the treatment plan for glioblastoma may combine several approaches, including surgery, radiation therapy, chemotherapy, clinical trials, Tumor Treating Fields (TTFields), and targeted therapies.
Surgery is often the first step in treating glioblastoma. Surgery allows the medical team to get a biopsy and make a diagnosis, relieve pressure on the brain, and safely remove as much tumor as possible. Glioblastomas are diffuse and have finger-like tentacles that infiltrate the brain, which makes them very difficult to remove completely. This is particularly true when the tumors are growing near important regions of the brain that control functions such as language and movement/coordination.
More anecdotal evidence.
Someone one degree of separation from me had a tumor behind her eye.
It was excruciating.
Tumor was removed.
It came back.
Yes.
Got the shots. Hubs is a doc.
The topic is not open for discussion as to the nature of the tumor.
As I’ve said a million times, me no STEM.
But I understand the concept of Dual Use.

I have a terrible feeling that we just getting started, y’all.
I see you, Monster.
Or I think I do.’
My daughter in law got the all-clear from her turbo bowel cancer about 4 weeks ago. The family were on a holiday to celebrate being "cancer free." She started showing signs such as in the list above and went to the local hospital last night. Fortunately they were in a capital city that has CAT scan facilities and not hiking as they were several days ago. Anyway, learned a few hours ago that she now has a brain tumour. Its not a GB, but metastasized from the bowel cancer she was apparently free of. So its called a MET tumour which isn't as aggressive as a GB but it's too unstable for her to fly home.
So there she is again, making decisions about cancer treatments etc with a baby and a toddler. My son is devastated as we all are. Surgery is scheduled for Monday morning. She told me she's not going down the chemo path again, but will go to an alternative-treatment Mexican cancer clinic after recovering from the surgery. And yes, 3 or 4 (?) times jabbed. But we are just one family from the many thousands (or millions?) from around the world (Australia) going through this same dreadful ordeal. I have no more words ...
These Glioblastomas Brain Cancers are also linked with heavy cell phone usage. People usually get the cancer on the same side of their brain that they hold their phone up to their ear. I suspect that having a COVID vaccine or two or three or four or five, etc. will probably increase one's likelihood of getting this type of cancer, but also heavy cell phone usage likely increases one's risk as well. Especially among people who hold the phone up to their ear, vs talking on speaker phone a few feet away from one's ear.