


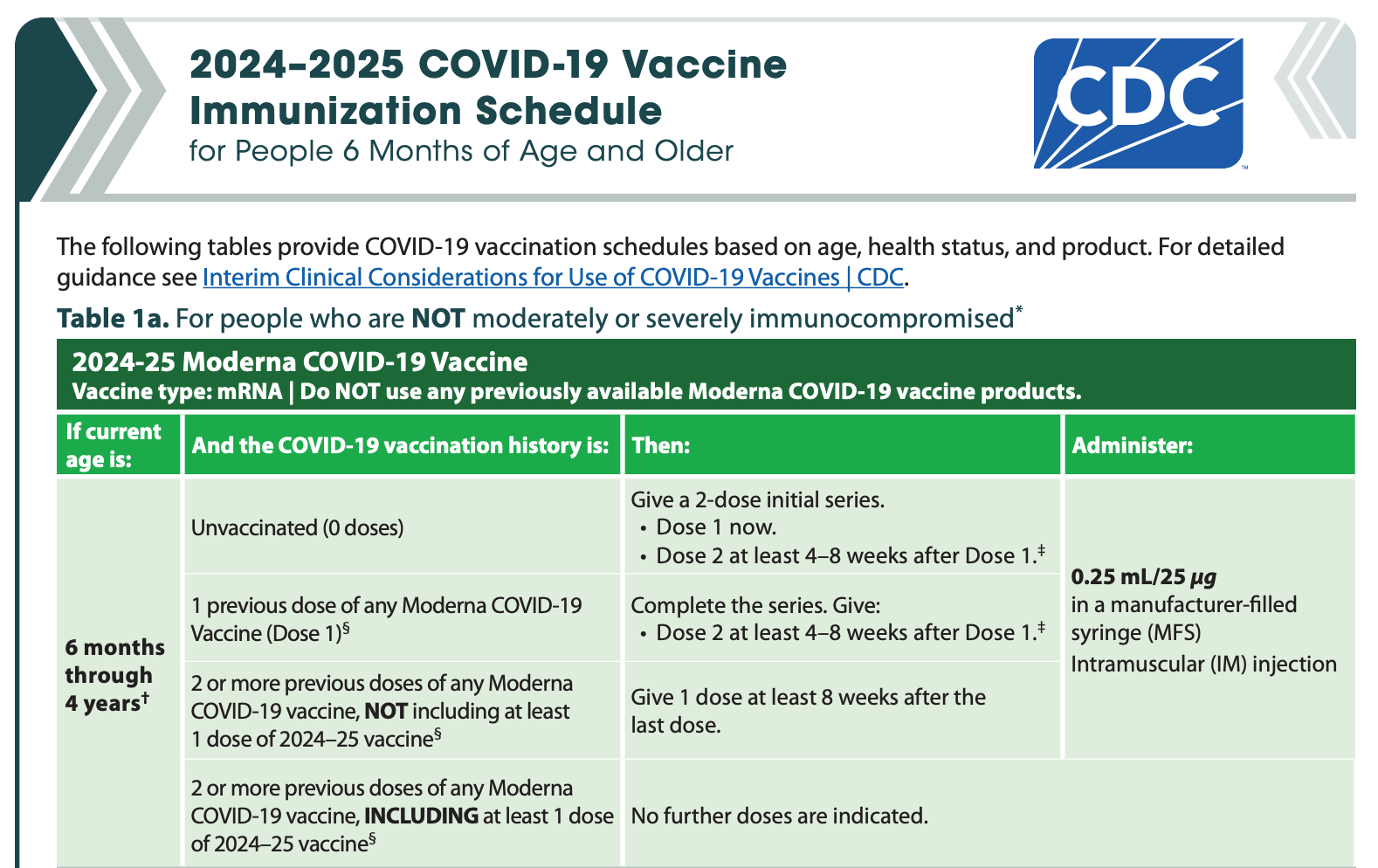
Why is the Malone Bourla Bancel Sahin BioNTech Pfizer Moderna et al. mRNA technology LNP transfection death vaccine still on the CDC's children vaccine schedule? Babies as young as 6 months? Why has
POTUS Trump not called for the removal of the deadly mRNA vaccine from US market? Why has Makary (FDA), Bhattacharya (NIH) remained silent? I am calling on RFK Jr. (Bobby Jr.) to PULL all mRNA vaccine

for babies, children in the United States. Healthy children are not at risk for this fake fraud non-pandemic PCR created ‘lie of asymptomatic transmission’ COVID, they never were. The evidence has accumulated bullet proofed that the mRNA vaccine is ineffective, does not sterilize as does not stop infection or transmission, is non-neutralizing to the circulating clades/variants, and is deadly, prone to myocarditis, strokes, bleeds, clots, paralysis, aneurysms, cardiac arrest etc. Same as the pressing fraud PCR created fake avian bird flu (H5N1, H5N2, H5N8, H7N9 etc.) where no mRNA vaccine can or will ever work for any respiratory pathogen like the fake bird flu that is highly mutable and whereby systemically introduced vaccinal antibodies do not reach the respiratory/oral/pharyngeal mucosal lining.
When will these leaders act? See my paper 3 years, near 4 ago, telling Pfizer/Bourla to leave our EFF in children alone with their fake fraud ineffective, not needed, deadly mRNA vaccine.
I will continue calling on RFK Jr. for I think he wants to do good and is and will try, I do think he is hobbled within a den of thieves and subversive people to MAHA/MAGA…I think RFK Jr. seeks to fix things, for his legacy, for his basic desire to help improve lives and well-being that has defined his life, certainly last half, and thus I am trusting him and calling on him!
I wrote near 4 years ago (see below) to consider your children already vaccinated…to leave them with their healthy functional innate (broadly protective) immune system, let it be trained and develop, let children live free and unfettered, healthy kids, let them roam, no lockdowns, no school closures. No mRNA vaccine. None! Still today! Let them be exposed to environments, harmlessly and naturally, and their innate God given immune system, their acquired adaptive immune systems, their first line of defenses (innate antibodies B-1 cells, natural killer cells NK cells) will vanquish anything. Leave them alone.
‘Pfizer plans to go to the FDA to get authorization for vaccination of 5 to 12 year old children based on a study they claim to have completed. The Biden administration is on board.
This is absolutely reckless, dangerous based on lack of safety data and poor research methodology, and without any scientific basis.
Are children at risk for Covid-19 that would warrant a vaccine? What does the evidence show?
The infection mortality rate (IFR) is roughly similar (or likely lower once all infection data are collected) to seasonal influenza. Stanford’s John P.A. Ioannidis identified 36 studies (43 estimates) along with an additional 7 preliminary national estimates (50 pieces of data) and concluded that among people <70 years old across the world, infection fatality rates ranged from 0.00% to 0.57% with a median of 0.05% across the different global locations (with a corrected median of 0.04%). Survival for those under 70 years is 99.5% (Ioannidis update). Moreover, with a focus on children, “The estimated IFR is close to zero for children and young adults.” The global data is unequivocal that “deaths from Covid are incredibly rare” in children.
The published evidence is conclusive that the risk of severe illness or death from Covid-19 in children is almost nil (statistical zero) and this evidence has accumulated for well over a year now; in fact we knew this for over 18 months. It is clear that children are at very low risk of spreading the infection to other children, of spreading to adults as seen in household transmission studies, or of taking it home or becoming ill, or dying, and this is settled scientific global evidence. Children are less at risk of developing severe illness courses, and also are far less susceptible and likely to spread and drive SARS-CoV-2 (references 1, 2, 3, 4). This implies that any mass injection/inoculation or even clinical trials on children with such near zero risk of spread and illness/death is contraindicated, unethical, and potentially associated with significant harm.
The risk-benefit discussion for children with these Covid-19 injections is a very different one than that for adults. The fact is that this is a completely novel and experimental injection therapy with no medium or long-term safety data (or even definitive effectiveness data). If we move forward with the vaccination of our children without the proper safety testing, then we will present them with potentially catastrophic risk, including deaths in some.
A team of Johns Hopkins researchers recently reported that when they looked at a group of about 48,000 children in the US infected with the virus, they found no (zero) Covid deaths among the healthy kids. Dr. Makary indicated that his team “worked with the non-profit FAIR Health to analyze approximately 48,000 children under 18 diagnosed with Covid in health-insurance data from April to August 2020…after studying comprehensive data on thousands of children, the team “found a mortality rate of zero among children without a pre-existing medical condition such as leukemia.”
With this background, we knew of the very low risk to children in the first place, but wanted scientific documentation (molecular/biological) of why this low risk existed, to help support our argument against these injections in our children. The evidence presented below (including on the risk of the injection itself) may help explain why children are not candidates for the Covid vaccines (here and here) and may well be (are) immune and can be considered “fully vaccinated.”
The key arguments are:
1.) The virus uses the ACE 2 receptor to gain entry to the host cell, and the ACE 2 receptor has limited (less) expression and presence in the nasal epithelium in young children (potentially in upper respiratory airways); this partly explains why children are less likely to be infected in the first place, or spread it to other children or adults, or even get severely ill; the biological molecular apparatus is simply not there in the nasopharynx of children as reported eloquently by Patel and Bunyavanich. By bypassing this natural protection (limited nasal ACE 2 receptors in young children) and entering the shoulder deltoid, this could release vaccine, its mRNA and LNP content (e.g. PEG), and generated spike into the circulation that could then damage the endothelial lining of the blood vessels (vasculature) and cause severe allergic reactions (e.g. here, here, here, here, here).
2) Recent research (August 2021) by Loske deepens our understanding of this natural type biological/molecular protection even further by showing that pre-activated (primed) antiviral innate immunity in the upper airways of children work to control early SARS-CoV-2 infection…resulting in a stronger early innate antiviral response to SARS-CoV-2 infection than in adults.”
3) When one is vaccinated or gets infected naturally, this drives the formation, tissue distribution, and clonal evolution of B cells which is key to encoding humoral immune memory. There is recent research evidence by Yang published in Science (May 2021) that blood examined from children retrieved prior to Covid-19 pandemic have memory B cells that can bind to SARS-CoV-2, suggestive of the potent role of early childhood exposure to common cold coronaviruses (coronaviruses). This is supported by Mateus et al. who reported on T cell memory to prior coronaviruses that cause the common cold (cross-reactivity/cross-protection).
4) Weisberg and Farber et al. suggest (and building on research work by Kumar and Faber) that the reason children can more easily neutralize the virus is that their T cells are relatively naïve. They argue that since children’s T cells are mostly untrained, they can thus immunologically respond more rapidly and nimbly to novel viruses.
5) Risk: There is an emerging discussion that with approximately 570 Covid injection deaths registered in VAERS in children, and the CDC reporting approximately 350 deaths in children since the inception of the emergency (Feb/March 2020), then the vaccine is killing more children than the virus/disease itself (Steve Kirsh, personal communication, September 2nd 2021).
6) A Yale University report (Yale and Albert Einstein College of Medicine report Sept. 18, 2020 in the journal Science Translational Medicine) indicates that children and adults display very diverse and different immune system responses to SARS-CoV-2 infection which helps understanding why they have far less illness or mortality from COVID. “Since the earliest days of the COVID-19 outbreak, scientists have observed that children infected with the virus tend to fare much better than adults…researchers reported that levels of two immune system molecules — interleukin 17A (IL-17A), which helps mobilize immune system response during early infection, and interferon gamma (INF-g), which combats viral replication — were strongly linked to the age of the patients. The younger the patient, the higher the levels of IL-17A and INF-g, the analysis showed…these two molecules are part of the innate immune system, a more primitive, non-specific type of response activated early after infection.”
7) Dowell et al. (2022) recently published and commented on antibody and cellular immunity in children (aged 3-11 years) and adults. Their findings confirm a biological basis for why SARS-CoV-2 infection is generally mild or asymptomatic in children. They reported that antibody responses against spike protein were elevated in children and seroconversion “boosted responses against seasonal Beta-coronaviruses through cross-recognition of the S2 domain. Neutralization of viral variants was comparable between children and adults. Spike-specific T cell responses were more than twice as high in children and were also detected in many seronegative children, indicating pre-existing cross-reactive responses to seasonal coronaviruses.” Very key in the findings were that children maintained and preserved “antibody and cellular responses 6 months after infection, whereas relative waning occurred in adults. Spike-specific responses were also broadly stable beyond 12 months. Therefore, children generate robust, cross-reactive and sustained immune responses to SARS-CoV-2 with focused specificity for the spike protein.”
What can be concluded? Pulling these emerging research findings together strengthens the case that children are not candidates for the Covid vaccines and are to be considered already “fully and completely Covid-vaccinated.” Furthermore, as lucidly outlined by Whelan, it is potentially disastrous to children if we move forward with vaccines without proper study of the possible harms to them. Vaccine developers failed to conduct the proper safety studies and for the duration that would unravel any harms.
Regulators: please slow down and demand safety testing, no matter how long it takes. Conduct proper risk-benefit analyses and see that the injections are contraindicated in children. Particular care is needed with regard to the potential widespread injection of children before there are any real data on the safety or effectiveness of these injections.
There is very little risk and no data or evidence or science to justify any of the Covid-19 injections in children. Under no circumstance should we expose the risk of the injections to children, and to consider putting risk on children so as to protect adults is perverse and reckless and very dangerous. There is no safety data. The focus rather has to be on early treatment and testing (sero antibody or T cell) to establish who is a credible candidate for these injections if properly ethically informed and consented, for it is very dangerous to layer inoculation on top of existing Covid-recovered, naturally acquired immunity (no benefit and only potential harm/adverse effects) (here, here, here, here, here, and here).
We must establish who is Covid-recovered, which is natural immunity, as this is a critical piece of the puzzle before any injection. Additionally, if public health agency leaders Fauci, Walensky, and Collins continue to demand that our children be vaccinated, then they must remove liability protection for all who benefit from it.
What does all of this mean? A biological and molecular (as well as epidemiological) argument was presented that shows children are already ‘vaccinated.’ Pfizer and all Covid vaccine developers (including Walensky of the CDC, Fauci of NIAID, and Francis Collins of the NIH) must step away from our children and only discuss this if they remove liability protection from the table.
If they have no risk on the table, then we cannot take this chance as parents. Something then is not entirely proper about these vaccines in our children. If children are at such low risk, then it should be a problem for these officials and vaccine developers to remove their protection. With such low risk in children and no opportunity for benefit and just costs in terms of possible harms, then these vaccines are a ‘no go’ for our children.’
___
You must not wait for another catastrophic crisis (at times manufactured but we are prevented from making our own basic personal decisions or accessing needed drugs and response tools) to catch you off-guard. We must take charge and be prepared today so that we can enjoy peace of mind tomorrow.
Enter the Wellness Company as a solution and a willing participant in the health care conversation. From telemedicine, prescriptions, memberships, and supplements, TWC is leading America with alternative choices to the traditional health care model.
If you wish to give a donation to help me, you can at:
Zelle:
sr7283@gmail.com
Or Ko-Fi
Ko-fi.com/drpauleliasalexander
Or to my address at:
150 South 8th Street
Unit 170
Lewiston, New York
14092
Alternatively, please consider going from an UNPAID subscriber or follower to a PAID at $5 per month or $30 per year. This can provide me help. If this is not possible at this time, this is ok, please remain a subscriber for FREE and there is no difference between FREE and PAID. No restrictions.
Please consider support of a good PATRIOT company (in this PATRIOT economy) Drs. McCullough, Risch, Thorp, myself support (they are our sponsors), The Wellness Company; see the emergency preparation kit (key component being antibiotics you were denied by doctors, pharmacists, governments during the fraud COVID), first aid kit, travel emergency kit, contagion control kit etc. Please consider the SPIKE SUPPORT (spike protein DETOX dissolving spike from mRNA vaccine, this is critical to remove spike form the mRNA vaccine/and DNA viral vector) formula with NATTOKINASE as well as the triple formula (SPIKE SUPPORT, BROMELAIN, CIRCUMIN)







COVID remains the greatest hoax and crime ever on United States, all of it, from fake virus to origins to lockdowns to mRNA vaccine, all...it was all a lie, all, to harm Trump term one and to impact an election and it did, he lost. Fraud COVID and OWS lockdowns took down Trump, and the mRNA vaccine rollout and mandates took down Biden. And no one responsible have paid a price.
As I have written before, the Children's vaccine schedule was from November 24, from the Biden Administration.
Trump did sign some EOs such as to remove the requirement for the Jab for those applying for adjustment of status to be Permanent Residents. However, it wasn't removed from the CDC website until March 13, after some litigation went through.
The same seems to be happening with the Children's Schedule, and I speculate that holdovers like Peter Marks are stonewalling the changes.
I will post again the link, that says there are changes to be implemented, per Trump EO.
That banner was there in early March, and is still there.
It would not surprise me if the same group is litigating right now.
At least Peter Marks will no longer get in the way:
https://www.cdc.gov/vaccines/imz-schedules/child-easyread.html